-- Age > 80 years old
-- NIH Stroke Scale > 25
-- History of combination of previous stroke and diabetes
-- On anticoagulation medication, regardless of INR
Acute LV Dysfunction in the Critically Ill
Great resource for teaching in the emergency department....
Here is a great new app that you can use when teaching residents and students in the ED. It's the NEJM app. Great pics, videos, audio, procedures, and articles. And, it's FREE.

Just go to the App store and search "NEJM"
For those that listen to EmedHome's EM Cast, you may have already heard this but I thought it's worth sharing with everyone else:
Many of us learned in our training that you should never give calcium to a hyperkalemic patient that is on digoxin or has digoxin toxicity. However, there's a paucity of data to support this contention. Here's one more article suggesting that calcium in the presence of digoxin or dig-toxicity may, in fact, be okay.
Levine and colleagues retrospectively evaluated 161 patients with digoxin toxicity, of whom 23 patients received calcium for hyperkalemia. None of the patients developed significant dysrhythmias in the first hour after calcium, and there was no increase in mortality rate.
Though not definitive, this is further support for treating hyperkalemia with calcium even in the presence of digoxin toxicity.
Many patients report an allergy to iodinated RCM, sometimes adding to the complexity of diagnostic decision making. Here are a few pearls to help:
Bottom line: Despite the lack of cross reactivity with shellfish/iodine allergies AND the very low risk associated with today’s low osmolality agents, premedication is still indicated in patient’s with a history of IHR to RCM.
Head injuries in children under 2yo are stress provoking, particularly with regard to when you should be getting a head CT. Luckily, a large (42,412 children, 10,718 <2yo) multi-center trial exists to guide your behavior.
The optimal hemoglobin concentration during critical illness is unknown. Although a liberal transfusion strategy (Hb 10-12 g/dL) was once believed to be beneficial for hemodynamics, evidence suggests targeting a conservative strategy (Hb 7-9 g/dL) does not increase mortality, while the unnecessary transfusion of blood products can cause harm (transfusion associated lung injury, infection, etc.) in the non-hemorrhaging patient.
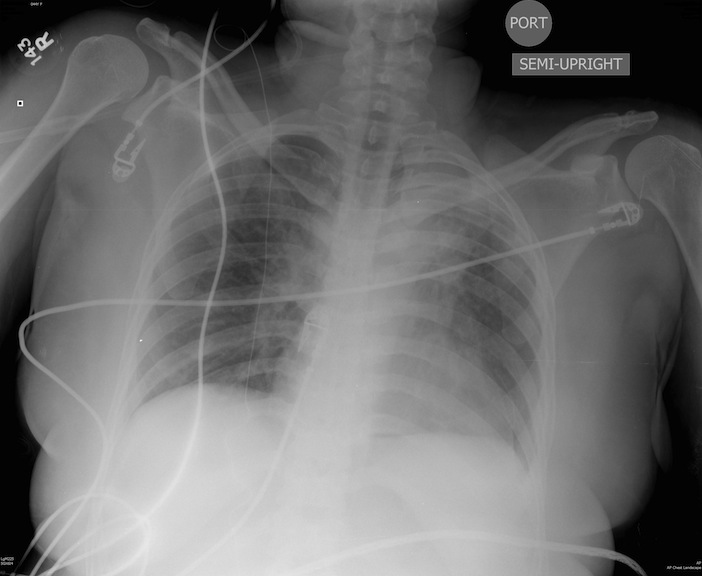
44 y/o female restrained driver s/p motor vehicle crash complaining of chest pain and shortness of breath.
Dabigatran (Pradaxa), an antithrombin medication, was discussed in an earlier pearl and thought I would play devil's advocate and explain the possible concerns:
Toxicology Mantra: You never want to be the first person or the last person to use a drug
|
Valproic Acid in Status Epilepticus
Well, there may finally be a replacement for patients with atrial fibrillation who take warfarin (Coumadin).
In late 2010, the FDA approved the drug Dabigatran (Pradaxa) for use in patients with atrial fibrillation.
Dabigatran is an oral direct thrombin inhibitor that has been approved for stroke prevention in patients with A Fib. The drug does not need monitoring like warfarin, and has been deemed to be safer than warfarin.
Be on the lookout for Dabigatran...
Bretylium was touted for many years as the drug of choice for patients with ventricular dysrhythmias in the setting of hypothermia...in fact it still is recommended by some. Bretylium was actually touted to be effective based on animal studies in which the dogs were PRE-treated with bretylium and then hypothermia was induced. It was found that dogs that were pretreated had fewer episodes of ventricular fibrillation than dogs that were not pretreated. On the other hand, if bretylium was used as a treatment for VFib rather than a prophylactic, it was ineffective. The bottom line....don't bother with bretylium.
Iliotibial band syndrome (ITBS)
http://footcarexpress.com/foot-orthotics/wp-content/uploads/2009/01/iliotibial-band-syndrome.jpg
Hx -
PE-
Tx
Brain death is the permanent absence of cerebral and brainstem functions (coma, absent pupillary reflexes, no spontaneous respiration, etc.). Legally, brain death is equivalent to cardiopulmonary death.
If brain death is suspected, confirmation is necessary. The apnea test is most commonly used, evaluating for spontaneous breaths when disconnected from the ventilator. If apnea testing is not possible (e.g., ambiguous clinical exam or cardiopulmonary instability) ancillary testing is needed:

Boxer's (or Brawler's) Fracture
Up to 30-40% of patients with infective endocarditis have neurological symptoms as a result of embolization. This is a good reminder of the frequency of embolization, and also that infective endocarditis should always be part of the differential when you are evaluating a patient with fever + neurological abnormalities.
{kind=link}