Causes of Pulsatile Tinniitus
Although oral metronidazole is indicated for mild to moderate Clostridium difficile associated diarrhea, oral vancomycin should be considered first-line therapy in critically-ill patients with moderate to severe disease. Vancomycin dosing should begin at 125mg PO q6 and increased to 250mg q6 if poor enteral absorption exists. Consider adding metronidazole IV if either reduced enteral absorption or severe disease exists.
Recently, fidaxomicin has been shown to be non-inferior to oral vancomycin in the treatment of mild to moderate C. difficile. While promising, the study population was not critically-ill and extrapolation should be avoided.
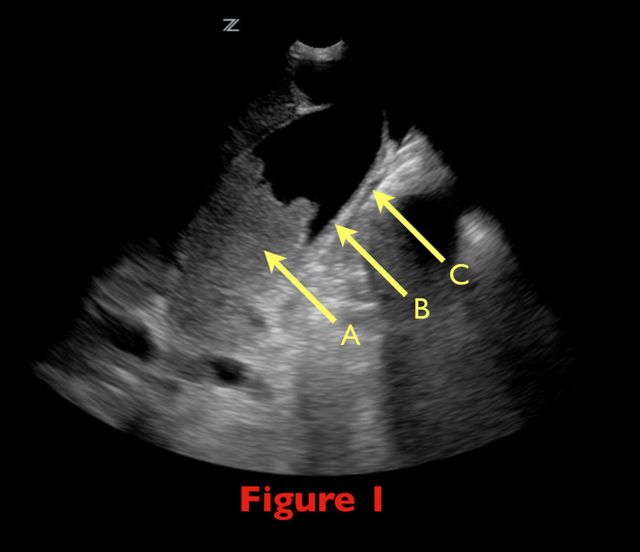
70 yo female from nursing home with fever. RUQ ultrasound is shown below. Diagnosis?

Beck's triad is well known to many physicians, but here's some simple things you may not have known.
Beck actually described two triads, one for acute and one for chronic tamponade.
The triad for chronic tamponade consists of increased CVP (JVD), ascites, and a small quiet heart (muffled heart sounds).
The triad for acute tamponade consists of JVD hypotension, and muffled heart sounds.
Almost 90% of patients have at least 1 of the signs, but only one-third have all 3. Furthermore, it appears that the simultaneous occurrence of all 3 signs is a very late manifestation of tamponade, usually preceding cardiac arrest.
Tendon Lacerations:
A reasonable approach to all tendon lacerations is to close the wound and splint in the hand in the position of function until the patient can be seen by a hand surgeon in the next 1-3 days. These injuries do not require immediate surgical repair.
Continuing the theme of endotracheal tube size pearls... You get a box call for a pre-term baby delivered precipitously by mom at home and baby is blue. EMS is bagging but unable to secure a definitive airway. What size ETT do you reach for? If you try to apply the formula "uncuffed ETT = (age/4) + 4", how much smaller than size 4 can you go?
IV acetaminophen has been approved for use since November 2010
It is indicated for the:
The results of studies demonstrating opoid sparing effects have been mixed; some studies have not demonstrated either a reduction in opioid dose or opioid side effects.
The dose is the same for acetaminophen administered by other routes.
It must be administered over 15 minutes, and onset of activity is 15 minutes. Peak effect occurs at one hour.
The MAJOR drawback is the cost, which is $13 dollars per vial. This is compared to oral acetaminophen and ibuprofen, which are pennies.
Lithium Toxicity
Gastrointestinal Changes of Obesity that Complicate Critical Illness
I found this neat little pearl on Michelle Lin's blog, Academic Life in Emergency Medicine, and thought it was worth sharing with everyone:
"In my theme of detoxifying malodorous smells in the ED (see Toxic Sock Syndrome and abscess drainage), I recently learned of a new way of masking odors. Imagine the stress on your olfactory nerves from the combined effects of urinary and fecal incontinence from a nursing home patient.
An ingenious nurse proposed nebulizing actual coffee within the room. Unfortunately, our ED was out of coffee at the moment.
Trick of the Trade:
Nebulized orange juice
I only learned of this trick after walking into the patient's very subtly foggy room. About 4 cc of orange juice had been nebulizing for a few minutes. The room smelled a little like a Jamba Juice (a smoothies/ juice shop). Quite pleasant actually. I was shocked to find that it masked the odors quite well."
Thanks for the tip, Michelle. Freshly-squeezed anyone??
Cocaine-associated MI occurs fairly early after acute cocaine use. 50% of MIs occur in patients prior to their arrival in the ED, and 24% of the total will occur within the first hour of cocaine use. If a patient has not ruled in by 12 hours post-arrival in the ED, it is extremely unlikely that the patient will rule in or suffer ACS-related complications from the cocaine....thus the concept behind using rapid rule out protocols in these patients.
The most important thing we as physicians can do for these patients is to strongly emphasize discontinuation of cocaine use and refer to rehab whenever possible. If the patient discontinues using cocaine, the prognosis for absence of subsequent cardiac events is excellent.
[thanks to Dr. Ellen Lemkin for her contribution to this pearl}
Tendon Lacerations:
Hand lacerations need to be carefully explored in order to determine whether there is an associated tendon laceration. These can be be difficult to find unless a systematic approach is followed:
Future pearls will cover techniques on how to repair tendon lacerations. Stay tuned.
You decided to intubate a child and wisely remembered that you should also follow with an NG/ OG after intubation to decompress the stomach. In order to avoid the blank stare when asked "what size"? Here's a nice mneumonic about Pediatric "tube" sizes... easy as 1-2-3-4!!! Please note ETT = endotracheal tube size.
So for example, a 4-year-old child would get intubated with a 5-0 ETT inserted to depth of 15 cm (3x ETT), a 10Fr NG/OG/foley (2x ETT), and a 20Fr chest tube (4x ETT).
Also, remember that you can use cuffed tubes in any child except neonates but the formula needs to be adjusted as follows: cuffed endotracheal tube ID (mm) = (age/4) + 3.5
Treating a patient with clinical hypoglycemia (neuroglycopenia if you want to sound cool) is with "1 amp of D50". Then some are starting D5 drips and D10 drips. Here is the actual breakdown of what you are giving:
1 amp of D50 = 50% dextrose = 50g/100mL = 25g x 4Kcal/g carbs = 100 calories bolus
1 L D5W at 100mL/hr = 5% Dextrose = 5g/100mL x 1L = 50g x (4Kcal/g) = 200 cal infusion of 20 cal/hr!
1 L D10W at 100mL/hr = 10%D= 10g/100mLx1L= 100g x (4Kcal/g)= 400 cal at infusion of 40 cal/hr!
Snickers Bar = 271 calories in one serving - most people will eat in 5 minutes = 54.2cal/min
Take home message is feed your patient once they are awake and alert. Much more effective.
Contraindications to performing lumbar puncture (LP):
- INR > 1.4 or other coagulopathy
- Platelets < 50
- Infection at desired puncture site
- Obstructive / non-communicating hydrocephalus
- Intracranial mass
- High intracranial pressure (ICP) / papilledema (relative contraindication depending on etiology; especially a concern with intracranial mass lesion secondary to the increased risk of transtentorial or cerebellar herniation)
- Focal neurological symptoms/signs, decreased level of consciousness
- Partial / complete spinal block
- Acute spinal trauma
A mortality benefit from combination antimicrobial therapy has not been clearly demonstrated in sepsis. However, when only the most severely-ill patients (i.e., septic shock) are considered in subgroup analysis, there appears to be a mortality benefit to using two antimicrobials against a suspected organism.
Combination antimicrobial therapy may reduce mortality through three mechanisms.
Always obtain appropriate cultures before initiating therapy. Although identification and susceptibility of the organism may take some time, eventually narrowing antimicrobial therapy to monotherapy in the ICU is still recommended.
Patient presents with the following X ray after yawning. Diagnosis?

Traditional teaching for many years has been that new or presumed new LBBB in patients with anginal type of symptoms should be treated as a STEMI, i.e. with immediate PCI or lytics. However, that teaching is based on poor evidence. Newer, increasing evidence is suggesting that new/presumed new LBBB in patients with anginal symptoms is actually not associated with acute MI any more often than when a patient has an old LBBB with those symptoms.
Probably the best management in patients with anginal type of symptoms and a new/presumed new LBBB is to contact the cardiologist on call and ask them for their preference in terms of treatment. Those patients are not necessarily definite AMIs.
Gout treatment considerations
Treatment is directed to relieve pain and inflammation
NSAIDs, steroids and narcotics are the mainstays of treatment. All 3 should be used in combination.
Aspirin should be avoided as it may increase uric acid levels
Note: not in prevention doses (81mg) in treatment doses (325-650mg q4h)
NSAIDs and steroids take time to be effective. Provide appropriate analgesia with oral narcotic medication for short term relief
Don't forget the benefit of splinting a "hot" joint (the ankle or wrist for example)
NSAIDs: Use may be limited in the elderly and in those on coumadin or with peptic ulcer disease. 5-7 days of treatment is usually sufficient. Indomethacin is most commonly used (50 mg TID, which may be tapered to 25 mg TID after 3 days)
Steroids: Likely more effective than NSAIDs. Oral prednisolone is more effective than naproxen (1). Use prednisone 30-50 mg for 3-5 days without tapering (as we use for asthma). May be useful to supplement with NSAIDs on the tail end to prevent a rebound flare. If tapping the joint consider intraarticular steroids. If there is concern for medical noncompliance with oral steroids consider IM steroids (triamcinolone 60mg or methylprednisolone).
The ability to determine whether or not a patient is an alcoholic or will go into alcohol withdrawal syndrome (AWS) is not amenable to a clinical decision rule though many attempts have been made. The strongest predictor that a patient can develop AWS is a positive family history of AWS. Some clinical and biochemical predictors are:
ALT >50 U/L
K <3.6
These two in one study have had an odds ratio of 9.0 and 5.7 respectively though specificity was quite low. Ethanol levels has also found to be contradictory. Being able to predict AWS does not currently seem plausible but the treatment of AWS should and can involve a clinical decision rule like CIWA-Ar which is a scoring system that takes into account N/V, tremor, sweats, anxiety, agitation, hallucinations, headache and sensorium. Take a look at the scoring system that is most validated and utilized for symptom triggered therapy - often considered the most effective treatment for alcohol withdrawal.