When may an ED thoracotomy be futile?
13 year-old right-hand dominant male following assault with blunt object. Diagnosis?


Here are a few important points to keep in mind when evaluating elderly patients in the ED or when prescribing a new drug:
Pay special attention to medication lists and new prescriptions in the elderly....much more attention than with younger patients!
1) C-A-B for CPR. Now recommended to start compressions immediately instead of the conventional rescue breaths.
2) Capnography during CPR. Continuous capnography recommended during CPR to guide the resuscitation, especially the effectiveness of chest compressions.
a. If ETCo2 is less than 10 to 15 mm Hg consistently, focus your efforts on improving chest compressions.
3) Etomidate for RSI induction. Okay to use in infants and children, BUT not recommended for pediatric patients in septic shock. Etomidate was not addressed in 2005 guidelines.
4) Cuffed ET tubes. Acceptable to use in infants and children.
5) Limit FiO2 after resuscitation. Keep O2 sats ≥94%. Avoid hyperoxia.
6) Therapeutic hypothermia after cardiac arrest. Recommendation based off of adult data, no pediatric prospective RCT done on this. This is beneficial in adolescents with out-of-hospital VF arrest.
a. Consider therapeutic hypothermia for infants and children.
b. Cool to 32oC-34oC
o The FDA is now asking manufacturers to limit the amount of acetaminophen in combination products to 325 mg per dose.
o The higher dose formulations will be phased out by 2014.
o The FDA is also considering lowering the maximum total to 3 gm per day, and a maximum dose of 650 mg per dose
o This does not pertain to OTC, but this is likely to change in the near future; Johnson & Johnson (manufacturer of Tylenol) has already adopted these recommendations.
Pregnancy causes many physiologic changes, which may be challenging during trauma resuscitations. A few pearls on the ABC’s:
Airway
Breathing
Circulation
In a 1991 article published by Wrenn and Slovis, the ten commandments of emergency medicine are discussed. This is an awesome article and a must read for everyone in EM.
Michelle Lin recently mentioned these on her blog, Academic Life in Emergency Medicine....
The Ten Commandments of Emergency Medicine:
1. Secure the ABC's
2. Consider or give naloxone, glucose, and thiamine
3. Get a pregnancy test
4. Assume the worst
5. Do not send unstable patients to radiology
6. Look for common red flags
7. Trust no one, believe nothing (not even yourself)
8. Learn from your mistakes
9. Do unto others as you would do to your family (and that includes coworkers)
10. When in doubt, always err on the side of the patient
These are great teaching pearls for new interns and for the rest of us as well....
Wound Repair
A pearl last year addressed the irrigation of wound and the fact that the type of fluid (sterile versus tap water) does not affect infection rates but rather the volume of irrigation is most important.
Sterile versus unsterile gloves have also been studied, and it turns out that clean unsterile gloves have the same rate of infection as sterile gloves but come with a substantial cost savings.
When caring for a contaminated wound it is most important to remove any gross contamination, and then irrigate the wound as much as possible. A 20 mL syringe with an 18G angio-catheter provides the proper pressure to remove debris without causing tissue damage. The wound can then be closed wearing the gloves that are most comfortable or accessible to you.
Finally, from a medicolegal standpoint it is always best to inform the patient that you have tried to remove all of the contamination but there is still a chance that the wound can get infected.
Acute Poststreptococcal Glomerulonephritis (APSGN) is a sequela of group A beta-hemolytic streptococci (GAS) infection of the skin or pharynx with nephrogenic strains of GAS. Damage to the kidneys is due to deposition of antigen-antibody complexes in the glomeruli.
Presentation:
Testing:
Treatment:
Prognosis (favorable):
Reference:
Kit, Brian. Assess the volume status and electrolytes in children with poststreptococcal glomerulonephritis. Avoiding Common Pediatric Errors. 2008. p356-57.
The incidence of tendon rupture related to fluoroquinolone use is reported to be in the range of 1 in 6000.
The risk of tendon rupture associated with FQ use is increased in those older than 60 years of age, those taking steroids, and in patients who have received heart, renal, or pulmonary transplants.
There is no evidence that tendon rupture is more likely for patients taking levofloxacin compared to other FQs.
Blood Pressure in the Critically Ill Obese Patient
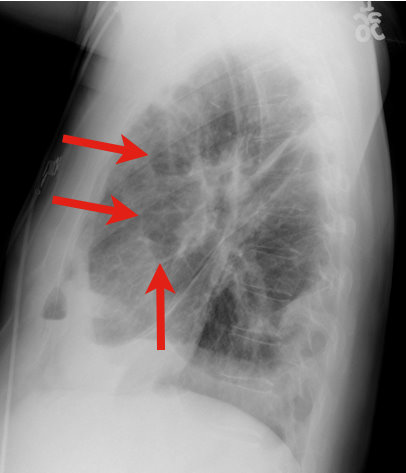
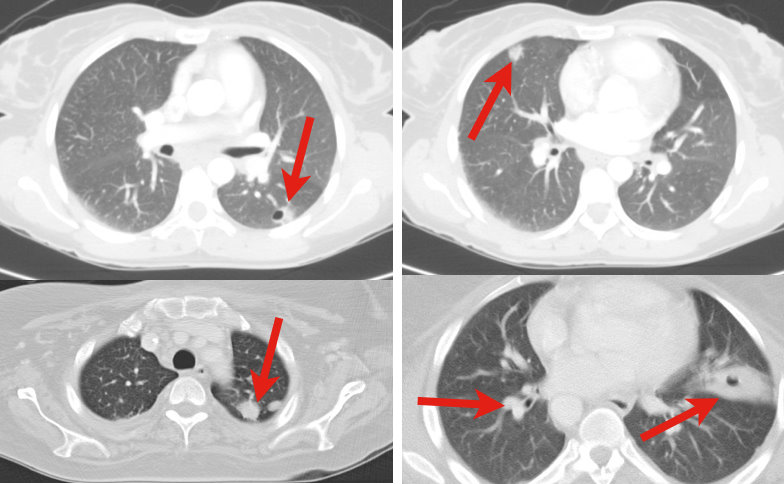
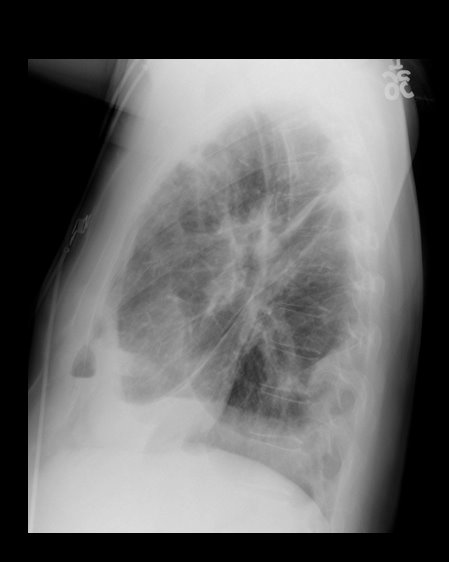
34 y.o. male with history of IVDA (intravenous drug abuse) complains of fever, chills and cough. Diagnosis?
Clues to RV infarction:
1. This almost always occurs in the presence of a concurrent inferior MI.
2. Clinical findings may include the triad of hypotension, JVD, and clear lungs.
3. ECG clues: in the presence of inferior lead ischemia or injury pattern, look for:
a. Combination of ST depression in lead V2 + ST elevation in lead V1; OR
b. Combination of ST depression in lead V2 + isoelectric ST segments in leads V1 and V3; OR
c. ST elevation in lead III markedly greater than the ST elevation in lead II; OR
d. ST elevation in right-sided leads (requires you to obtain right-sided leads)
Why is this diagnosis important?
1. It suggests a larger infarction and worse prognosis, so BE AGGRESSIVE in management.
2. Be very cautious with preload-reducing medications (e.g. nitrates) in the acute management of these patients, as they may induce significant reductions in blood pressure and extension of the infarction. Be aggressive with IVF, while maintaining close attention to the lung sounds.
Refractory Osteomyelitis is defined as a chronic osteomyelitis that persists or recurs after appropriate interventions have been performed or where acute osteomyelitis has not responded to surgery and antibiotics.
Case series, animal data and non-randomized prospective trials suggest that the addition of Hyperbaric Oxygen therapy to routine surgical and antibiotic management of previously refractory osteomyelitis is safe and improves the rate of infection resolution.
In patients with osteomyelitis involving spine, skull, sternum, HBOT is recommended prior to surgical intervention.
Typically patients require 20-40 daily dives for sustained therapeutic benefit.
How does HBOT work in osteomyelitis?
1. Restoration of normal to elevated O2 level in infected bone.
2. Leukocyte mediated killing of aerobic bacteria is restored when low O2 tension intrinsic to osteomyolitic bone is restored to physiologic or supra-physiologic levels.
3. HBOT is noted to exert direct suppressive effects on anaerobic infections.
4. HBOT augment the transport of certain abx (aminoglycosides and cephalosporins) across bacterial cell wall.
5. Enhance osteogenesis
6. Enhance angiogenesis
thank you to Dr. Sethuraman for this pearl
You're called to bedside to evaluate a "lethargic" infant. You wisely ask for a POCT glucose which returns at 35. How much dextrose do you give (since you know it's not just "an amp" of D50?
Here's a simple mnemonic:
Rule of 50-100 = multiply type of dextrose solution by ____ factor (ml/kg) to total 50-100
D10 (neonate) x 5-10 ml/kg = 50-100
D25 (infant) x 2-4 ml/kg = 50-100
D50 (child/adolescent) x 1-2 ml/kg = 50-100
There are increasing reports of bath salts which are crushed and then either injected, insufflated or taken orally. The actual substance has been found to be mephedrone as well as MDPV.(1) Both are amphetamine derivatives and the psychosis seen can appear like schizophrenia to the point that some of these patients have been admitted to the psychiatric wards. (2)(3) For those who have seen methamphetamine patients "tweaking" - where they use the drug for several days in a row without sleep - the presentation is quite similiar.
Synthetic drugs continue to present legal and regulatory problems since the compound is a "designer" synthesized drug that may not be on the DEA Schedule list. The product is labeled "Not for human consumption". Head shops and the internet remain primary sources of the drug. Bath salts present a serious and dangerous public health risk.