Aortocaval compression occurs often when gestational age is > 20 weeks. This compression significantly compromises the chances of maternal survival in cardiac arrest. Because it is often difficult to know the exact gestational age, it is commonly recommended that emergency C-section in maternal cardiac arrest be performed when the fundus extends above the level of the umbilicus.
GOUT part 1
Gout is an inflammatory arthritis that classically affects the first metatarsal phalangeal joint
Gout prefers cool ambient temperature hence gouty tophi prefer the great toe (one of the coldest parts of the body) and avoids "warmer" joints such as the hip and shoulder.
Remember that gout can affect other joints as well (elbow, wrist, knee and ankle) and can cause painful bursitis and tendonitis
Multiple joints can be involved simultaneously (leading to confusing with RA and OA)
The involved joint will often be red, hot, swollen and very painful leading to easy confusion with cellulitis and or a septic arthritis
Diagnose gout by demonstrating monosodium urate crystals in the synovial fluid.
**Remember previous pearl by Dr. Bond regarding the coexistence of gout with septic joint**
Serum uric acid levels are commonly elevated but can be normal or even low
Use caution with this test because asymptomatic hyperuricemia is much more common than gout
Note that yesterday's Neurology pearl should have read as follows -
Amongst others, diagnostic criteria for NMS includes:
Exposure to a dopamine ANTAGONIST (NOT AGONIST) or dopamine agonist withdrawal within past 72 hours.
Apologies for the type-o.
Could this be another risk factor for DVT/PE. Maybe not yet but it is worth mention. A recent observatioal study in BMJ showed that there was an associated increase with DVT or PE. From a database of 25,532 patients over a 3 year period of time and finding match controls, the results were:
Limitations were this is was an observational study with missing data. BMI was missing in these records and it is always difficult to tease out the multiple medications these patients are on. Also don't have a great biological mechanism (yet). Still makes you go hmm....
Antipsychotic drugs and risk of venous thromboembolism, Parker, BMJ, 2010.
- Exposure to dopamine agonist or dopamine agonist withdrawal within past 72 hours
- Hyperthermia
- Rigidity
- Mental status alteration
- Elevated creatinine phosphokinase
- Sympathetic nervous system lability (2 or more of the following: elevated blood pressure, fluctant blood pressure, urinary incontinence, diaphoresis)
- Tachycardia and tachypnea
- Negative work-up for infectious, metabolic, neurologic, or toxic etiologies.
Aspiration Pneumonitis and Pneumonia
Rib fractures are associated with significant morbidity and mortality in the elderly, and the risk increases dramatically with each successive rib fractured. An elderly patient with 3 rib fractures has a mortality of 20% and risk of pneumonia is 31%. As a general rule, you should really think twice about discharging home any elderly patients with rib fractures.
[credit to Dr. Joe Martinez for bringing forth this information]
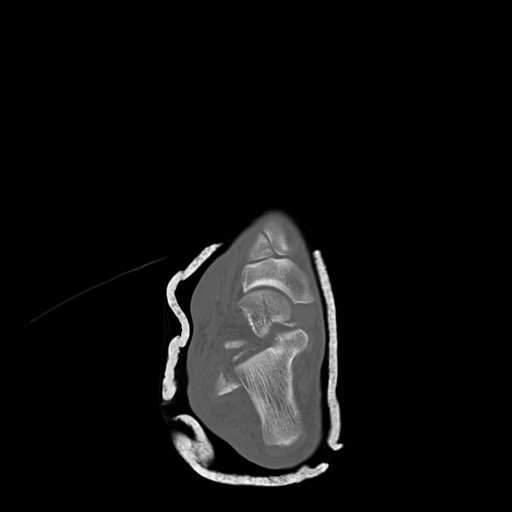
Talar Neck Fractures
Have a high rate of avascular necrosis (AVN), nonunion, and arthritis. Almost all require ORIF


Most have converted from succinylcholine to rocuronium for their choice of paralytic in RSI. Succinylcholine-induced hyperkalemia secondary to muscle fasciculations is considered usually clinically insignificant though there may be a hyperkalemic renal patient that this may tip them over. The fasciculations also may worsen traumatic long bone fractures. Here is the argument in a head to head comparison:
| Succinylcholine | Rocuronium | Winner | |
| Onset | 1-1.5min | 1.5-3min | Tie |
| Duration Recovery Index | 3-7min 2min
| 30-40min 10min | Mild S |
| Fasciculations | Yes | No | Roc |
| Histamine | Yes - Released | None | Roc |
| Pulse | Rare Brady | Rare Tachy at high dose | Tie |
Duration = injection of drug to 25% recovery of single twitch height (clinically relevant recovery in ED - essentially breathing may return)
Recovery Index = time from 25% to 75% recovery of single twitch height
The main reason succinylcholine was utilized was because of its fast onset and short duration. Rocuronium is comparable enough to succinylcholine in these characteristics tilting the overall benefits to rocuronium. If the FDA ever approves it, suggamadex is a possible reversal agent for rocuronium - currently used in Europe. Imagine having that in your RSI kit.
Many changes in pulmonary physiology occur during pregnancy. These changes are generally well tolerated but can become problematic when pathologic states arise.
Here are a few examples of the normal changes and potential consequences:
Progesterone increases tidal volume and respiratory rate.
“Normally" a mild respiratory alkalosis pH 7.4-7.47, PaCO2 28-32, and bicarbonate 17-22 (renal compensation).
Low metabolic reserve with systemic illness.
Weight gain, anasarca, and breast size reduces chest wall elasticity.
Potential for restrictive physiology and reduced lung volumes.
Can be challenging to to mechanically ventilate due to decreased compliance and intra-thoracic pressure
Mechanical displacement of abdominal and thoracic contents by growing uterus.
Reduced lung volumes leading to reduced oxygen reserve and decreased apnea time.
Aim higher if placing chest tube (avoid abdominal contents)
Uterine pressure on stomach can increase aspiration risk and pulmonary injury.
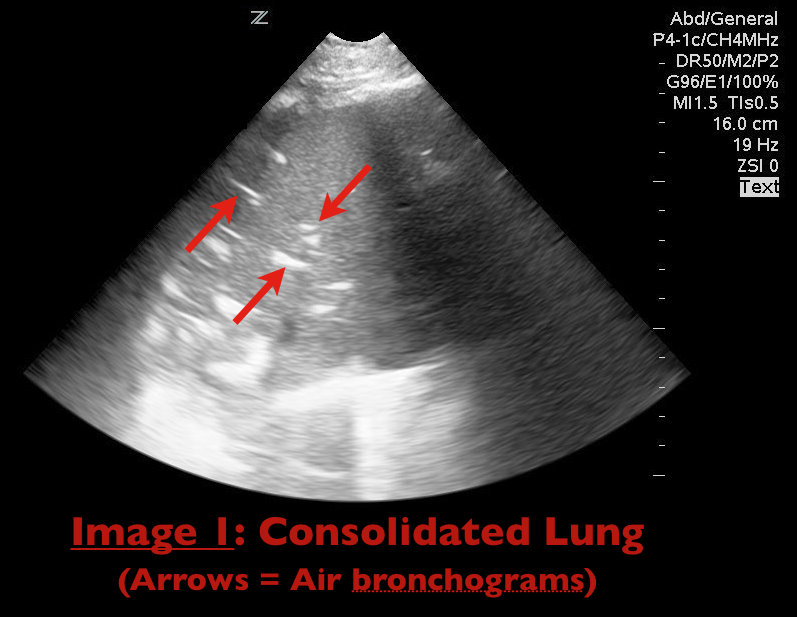
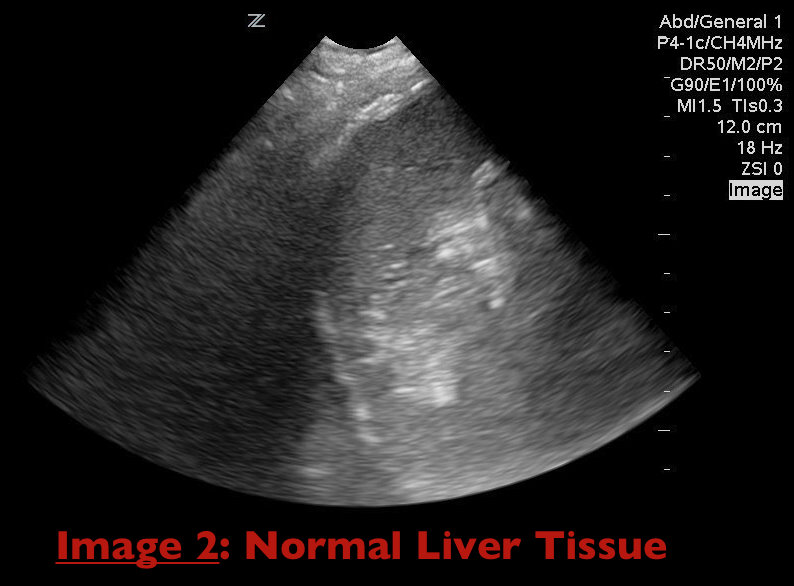
65 yo female with breast cancer presents with dyspnea and CXR shown below. Diagnosis? Can anything help clarify the diagnosis?

Elderly patients are prone to hypovolemia for the following two major reasons:
1. They have a decreased thirst response.
2. They have decreased renal vasopressin response to hypovolemia.
The result is that elderly patients have an impaired ability to compensate for a decreased cardiac output, which causes them to develop shock earlier and more easily with stressor.
Takeaway point: Always assume that most elderly patients are hypovolemic, and when they are stressed, give them fluids early!
Cubital Tunnel Syndrome aka Radial Tunnel Syndrome
Several medications/chemicals can cause unique toxicologic reactions in pediatric patients.
The onset of idiopathic seizures typically affects patients between ages 5 and 20.
Therefore, be highly suspicious of a diagnosable etiology in patients who present with new onset seizure prior to age 5 or after age 20.
Common causes of such seizures include:
The Severely Hypoxemic ED Patient
Adverse drug effects are a major issue in geriatrics.
Elderly patients take, on average, 5 prescription medications + 2 over-the-counter medications.
Adverse drug effects account for approximately 5% of all hospital admissions.
Nearly 20% of patients brought to the ED for psychiatric complaints have symptoms that are primarily caused by medication effects.
Be very wary whenever prescribing ANY new medications for even a short time to elderly patients.
Sulfamethoxazole (SMX)/trimethoprim (TMP) is the treatment of choice for PCP pneumonia. The IV formulation has been unavailable for almost a year due to shortage. It is contraindicated in patients with sulfa allergy. Here are the alternatives with adverse effects. You'll quickly see why pentamidine should generally be reserved for those with sulfa allergy and G6PD deficiency.
Mild-to-moderate disease:
Moderate-to-severe disease:
Adverse Effects: