49 y.o. female on Trimethoprim/sulfamethoxazole presents with rash and oral mucus membrane lesions. Diagnosis?

Paroxysmal supraventricular tachycardia (PSVT) is a common tachydysrhythmia encountered in ED practice. PSVT in itself has not been found to be an isolated manifestation of myocardial infarction or unstable angina (i.e. "isolated" = in the absence of other concerning symptoms, such as anginal-type pain, etc.). Nevertheless, some physicians will routinely test cardiac troponin levels to evaluate for ACS in these patients. We should all remember, though, that tachydysrhythmias including PSVT are a potential cause of elevated troponin levels in the absence of coronary disease, and these elevations do NOT correlate with adverse outcomes unless other concerning symptoms/signs are present as well.
A recent study1 corroborated this point: 11 out of 38 patients with PSVT had a positive troponin level. Only 2 of the 11 ruled in for ACS, and all of the patients were well at 30 days. Both patients presented with hypotension (SBP in the 70s) and also had other concerning symptoms, such as chest pain (both), dizziness (both), and dyspnea (one).
The takeaway point is simple: if you routinely send troponin levels on your patients for PSVT in the absence of other concerning symptoms/signs, you'll find yourself chasing a lot of false-positive levels.
Pes Anserine Bursitis is an inflammatory condition of the medial knee
Occurs at the bursa of the pes anserinus which overlies the attachment of the 1) Sartorius 2) gracilis and 3) semitendinosis tendons
Note the location is 2-3 inches below the knee joint on the medial side
http://kneespecialistsurgeon.com/images/uploaded/Pes%20anserinus%20bursitis%20image.jpg
http://eso-cdn.bestpractice.bmj.com/best-practice/images/bp/en-gb/575-27_default.jpg
Patients complain of pain (especially with stair climbing)
PE: Tenderness to palpation of the bursa with mild swelling
DDx: MCL tear, medial meniscus injury, medial (knee) compartment arthritis
Treatment: Cessation/modification of offending activities, Icing and ice massage, NSAIDs, hamstring stretching and physical therapy. Failure of the above should prompt referral for bursal steroid injection.
Cancer patients admitted to ICUs with AKI or who develop AKI during their ICU stay have increased risk of morbidity and mortality. AKI in cancer patients is typically multi-factorial:
Causes indirectly related to malignancy
Septic, cardiogenic, or hypovolemic shock (most common)
Nephrotoxins:
Aminoglycosides
Contrast-induced nephropathy
Chemotherapy
Hemolytic-Uremic Syndrome
Causes directly related to malignancy
Tumor-lysis syndrome
Disseminated Intravascular Coagulation
Obstruction of urinary tract by malignancy
Multiple Myeloma of the kidney
Hypercalcemia
Because AKI increases the already elevated morbidity and mortality in these patients, prevention (e.g., using low-osmolar IV contrast, avoiding nephrotoxins), early identification (e.g., strict attention to urine output and renal function), and aggressive treatment (e.g., early initiation of renal replacement therapy) is essential.
There are several complications of acute aortic dissection that emergency physicians must be familiar with.
These include:
*Key Pearl: If a patient with suspected or confirmed acute aortic dissection suddenly arrests consider cardiac tamponade.
Patients with Non-STE-ACS should not be given any NSAIDs aside from aspirin...that includes COX-2 agents. These medications in patients with acute or recent NSTE-ACS have been associated with an increased risk of hypertension, reinfarction, heart failure, myocardial rupture, and death.
Kocher Criteria for Septic Arthritis in Children:
Septic arthritis should be suspected in children that have a painful joint especially if they do not want to weight bear. Orthopedics uses the Kocher Criteria to determine the probability of whether the joint is infected.
Four elements make up the criteria:
If only one sign is present there is a 3% chance the child has a septic joint.
The true incidence of drug-induced seizure is very difficult to determine, however, a nice poison center study attempted to determine clinical factors associated with complications (potentially life-threatening) of drug-induced seizures. They found 3 predictors that demonstrated statistically significant associations:
They found a 60% complication rate in drug-induced seizures which is much higher than epileptic seizures. Makes sense since these patients are often sedated/altered or vomiting.
Stimulant Exposure is much more prominent in this population and has increased in mortality.
Interesting point with hyperglycemia, may be a novel marker for poor prognosis. Several studies have confirmed an association between hyperglycemia and increased neuronal injury and mortality in other settings like CVA and TBI.
Take home point - Drug-induced Seizure has a high complication rate in the ED. Watch for the 3 predictors as that may clue you in to the increased risk.
AKI in the Critically Ill Cancer Patient
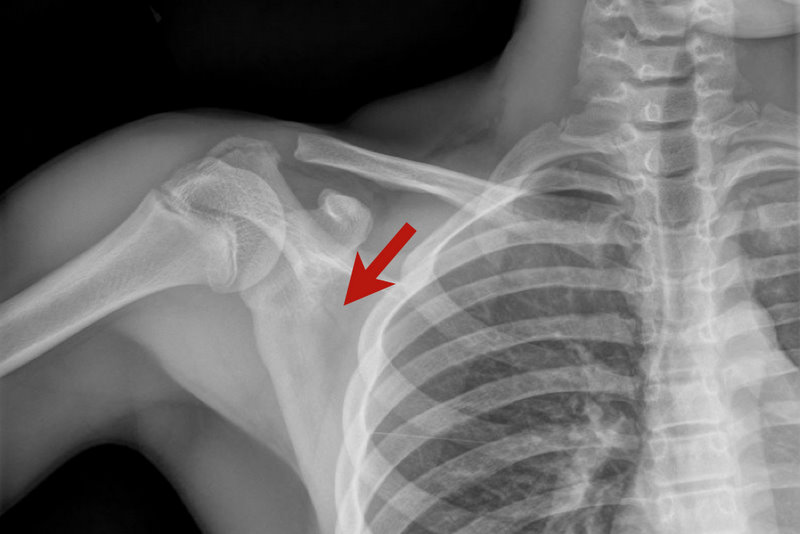
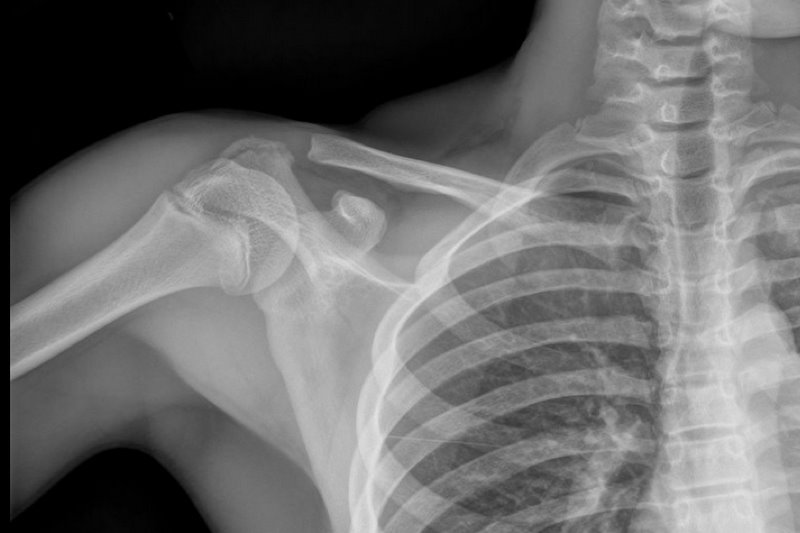
13 y.o. with shoulder trauma (during basketball game). Arm held in adduction and exquisite scapular tenderness. Diagnosis?
Proton pump inhibitors should be avoided in patients being treated with clopidogrel. PPIs appear to attenuate the effect of clopidogrel, and there's even some suggestion that the addition of PPIs to the medication regimen of patients taking clopidogrel may be associated with an increased risk of rehospitalization or death.
Kienbock’s disease is a rare entity involving collapse of the lunate due to avascular necrosis and vascular insufficiency.
Occurs most commonly in young adults aged 15 to 40 years.
Cause is unknown but believed to be due to remote trauma or repetitive microtrauma in at risk individuals.
Patients complain of wrist pain, stiffness and swelling
On exam, limited range of motion, decreased grip strength and passive dorsiflexion of the 3rd digit produces pain.
Dx: plain film in the ED and with MRI as an outpatient.
Tx: Wrist immobilization with splint and refer to orthopedics. Ultimate treatment is individualized and there is no clear consensus.
Lunate sclerosis seen on plain film
http://orthoinfo.aaos.org/figures/A00017F02.jpg
AVN of the lunate seen on MRI
http://www.assh.org/Public/HandConditions/PublishingImages/KeinbocksMRI_figure3.JPG
If there is a single truth of pediatric emergency medicine, it is that kids love to stuff things into their noses. A particular danger (aside from batteries, covered in a previous pearl) is the magnet.
Specifically, two magnets (as seen with magnet ear and nose rings, frequently worn by children and teens whose pesky parents won't allow piercings), attracted across the nasal septum can cause necrosis and perforation within hours.
Here's how to save yourself (and some noses):
Dehydration and subsequent prerenal acute kidney injury can result when temperatures begin to rise in the summer months. As a result, medications with narrow therapeutic indices that are primarily renally excreted may accumulate. Here are the specific ones to look out for:
Bleeding associated with uremia is a spectrum, from mild cases (e.g., bruising or prolonged bleeding from venipuncture) to life-threatening (e.g., GI or intracranial bleed). The exact pathologic mechanisms are not understood, but are likely multi-factorial (e.g., dysfunctional von Willebrand’s Factor (vWF) and factor VIII, increased NO, etc.)
Besides dialysis, treatments for uremic bleeding include:
A 20 year-old female presents with bilateral neck pain that occurred at rest. No other complaints. See if you can find the subtle clue on the x-ray...