Prasugrel is a new thienopyridine alternative to clopidogrel and is now listed as an option in the 2011 ACC/AHA Non-STEMI ACS Guidelines. Studies comparing it versus clopidogrel show a slight benefit in terms of adverse cardiac events, but at the expense of a slight increase in bleeding complications. Though the guidelines state no preference between prasugrel vs. clopidogral for NSTEMI ACS patients, prasugrel is finding a role in patients who appear to have a genetic resistance to the effects of clopidogrel (unlikely you'll know this in the ED, but you'll start seeing more patients started on this medication in the outpatient setting).
Prasugrel is contraindicated in patients with a history of TIA or stroke and it should not be given before cath is performed (in contrast, some protocols push for clopidogrel as early as possible, even before cath).
Pathophysiology: Angiotensin converting enzyme (ACE) catalyzes the conversion of angiotensin I to angiotensin II. It also degrades bradykinin. Thus, ACE inhibitors have the effects of decreasing angiotensin II and increasing bradykinin. In the presence of ACE inhibition, bradykinin can accumulate and interact with vascular bradykinin B2 receptors, causing vasodilation, increased vascular permeability, increased c-GMP, and release of nitric oxide.
Treatment: Even though we generally treat with standard allergic reaction medications, none counteract the mechanism causing the problem. Steroids, H1-blockers, and H2-blockers should still be considered but may not alter the progression. Airway monitoring and management is paramount.
Certain medications can cause a certain dermatologic pattern. Many fall into a generic waste basket of "contact dermatitis" but here are some more characteristic findings and the drugs that can cause them:
Alopecia - anticoagulants, chemo, phenytoin, retinoids, selenium, thallium
Erythema multiforme - allopurinol, barbiturates, carbamazepine, cimetidine, some antibiotics
Toxic Epidermal Necrolysis (TEN) - allopurinol, bactrim (sulfonamides), mithramycin, PCN, sulfasalazine, nitrofurantoin, phenytoin, prazocin
| PERIPHERAL | CENTRAL | |
| Nystagmus | ||
| Direction | Fast phase away from lesion; never reverses direction | Sometimes reverses direction if looking in direction of slow phase |
| Type | Horizontal with torsional component, never purely torsional or vertical | Can be in any direction |
| Other neurologic signs | Absent | Often present |
| Postural instability | Unidirectional instability, walking preserved | |
| Effect of visual fixation | Suppressed | Not Suppressed |
| Deafness or tinnitus | May be present | Absent |
Cardiovascular Complication of ESLD
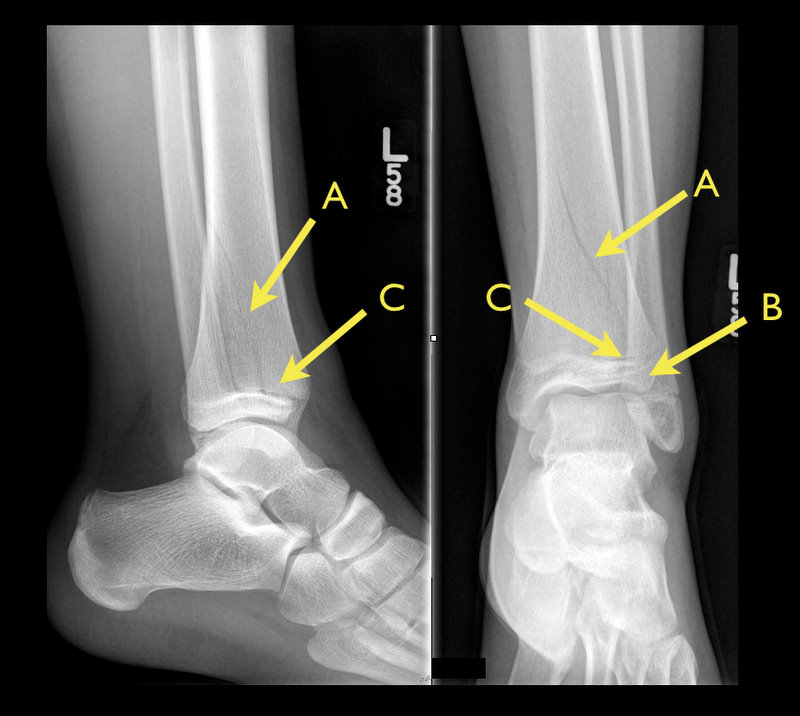
13 y.o. female with ankle pain following fall down escalator. What's the diagnosis? (Hint: Look very closely)

Therapeutic hypothermia in post-cardiac arrest patients with return of spontaneous circulation + coma (GCS < 8) is now well-accepted, and the current recommendations are for continued sedation of these patients. Consider avoiding the use of midazolam for sedation in these patients. Midazolam is metabolized more slowly in hypothermic patients, resulting in accumulation and the potential for longer ventilation and ICU time.
Transient brachial plexopathies aka Burners and Stingers
Brachial plexus injuries are the most common peripheral nerve injuries seen in athletes.
49-65% of all college football players have experienced at least one burner with a 87% recurrence rate.
Injuries most commonly occur at C5-C6 but may involve any root level.
3 Mechanisms: Commonly due to
1) Traction caused by lateral flexion of the neck away from the involved side
2) Compression of the upper plexus between shoulder pads and scapula
3) Nerve compression caused by neck hyperextension and ipsilateral rotation.
CC: Burning or numbness in the neck, shoulder and/or arm
Symptoms are UNILATERAL and tend to usually last seconds to minutes
Symptoms are reproduced by the Spurling maneuver.
Function gradually returns from the proximal muscle groups to the distal muscle groups.
Because most burners are self-limited, the most important goal is to rule out an unstable cervical injury.
TIP: Suspect when abdominal pain presents 10-14 after chemotherapy (when PMNs are lowest).

Iliopsoas tendonitis and Iliopsoas Syndrome
The following list of medications have been associated with the development of Lupus Anticoagulants. Though it sounds like they should anticoagulate, they interfere with the Protein C system which means that they could induce a pro-thrombotic state - good short list to know:
Chlorpromazine (Thorazine
Procainamide (sorry Amal, I know you love that drug)
Hydralazine
Quinidine
Phenytoin
(1) do not have increased risk for clinically significant ICH,
(2) have early clinical improvement similar to younger patients, and
(3) have poor outcomes related to increased mortality (odds ratio 30% versus 12%), rather than
to higher rates of functional dependence (i.e. Modified Rankin Score 3 to 5).
Acute Liver Failure (ALF)
Ever see that patient who shows up in the ED with blue painful toes? You look at the foot (or feet) and quickly determine that clot has embolized into the foot.
What is the differential diagnosis to consider in patients with evidence of embolic phenomenon in the feet (i.e. blue, painful toes)?
Things to consider:
Clearly we can't do the complete workup of embolic foot lesions, and many if not most of these patients will need to be admitted to complete their workup.

It is now well-accepted that induction of hypothermia should be initiated in victims of cardiac arrest who regain spontaneous circulation and remain unresponsive. Studies are now being performed and published that suggest that the earlier that hypothermia is induced, the better the neurological outcome. With this in mind, some experts are now recommending that cool IVF be the initial resuscitation fluid that these patients receive when resuscitation is initiated. It appears that aggressive use of cool IVF right from the initiation of attempted resuscitation results in improvements in survival to hospital admission and discharge.
The bottom line here is that when caring for victims of primary cardiac arrest, we should be certain to cool the patients fast and early!
Meralgia Paresthetica - caused by entrapment of the lateral femoral cutaneous nerve (LFCN)
The LFCN is responsible for sensation of the anteriorlateral thigh.
http://www.chiropractic-help.com/images/Meralgia-Paresthetica.jpg
NOTE* It has no motor component!
Associated with pregnancy, wearing tight pants, belts, girdles, and in diabetic and obese patients.
Symptoms include numbness, paresthesias and pain (not weakness). Worse w walking, standing. Better w sitting.
Diagnosis is clinical but may be confirmed with nerve conduction studies
Treatment includes, NSAIDs, injection and surgery for refractory cases.
"Ear to sternal notch" positioning has gained wide acceptance in the emergency medicine and anesthesia literature. Most often, this teaching is brought up with respect to obese adult patients whose large body habitus requires the raising of the neck and head to achieve airway alignment.
However, the correct anatomic positioning principle applies to all ages. Specifically, with regard to neonates, a shoulder roll is often placed indiscriminately to put the patient into the now out-dated "sniffing position," usually worsening the view of the airway.
Though this positioning is frequently misused, it can be easily adapted to apply ear to sternal notch positioning to neonates, whose misaligned airway is the result of a large occiput rather than a large torso. In all ages, if you follow these positioning principles, you will improve your view of the airway:
1. Align the ear to the sternal notch
2. Keep the face parallel to the ceiling (do NOT hyperextend the neck, as in the sniffing position)
3. In adults, the head usually needs to be raised (Image 1), while in infants, the torso usually needs to be raised (image 3).


Several patients have recently presented with a medication history including tapentadol (Nucynta), the newest opioid formulation. It is approved for treatment of acute moderate-severe pain. Here are some key points: