Category: Pharmacology & Therapeutics
Keywords: Droperidol, QTc (PubMed Search)
Posted: 5/7/2022 by Wesley Oliver
Click here to contact Wesley Oliver
A recent prospective cohort study investigated the effect of low-dose droperidol on QTc in an emergency department:
Low-dose droperidol has a small effect on QTc and most patients remained below 500 ms.
Hernández-Rodríguez L, Bellolio F, Cabrera D, et al. Prospective real-time evaluation of the QTc interval variation after low-dose droperidol among emergency department patients. Am J Emerg Med. 2022 Feb;52:212-219.
Category: Pediatrics
Keywords: autism spectrum disorder, neurodevelopmental disorder (PubMed Search)
Posted: 5/6/2022 by Rachel Wiltjer, DO
(Updated: 6/22/2026)
Click here to contact Rachel Wiltjer, DO
Category: Critical Care
Keywords: in-hospital cardiac arrest, IHCA, resuscitation, code, epinephrine, vasopressin, methylprednisolone (PubMed Search)
Posted: 5/2/2022 by Kami Windsor, MD
Click here to contact Kami Windsor, MD
Based on prior studies1 indicating possibly improved outcomes with vasopressin and steroids in IHCA (Vasopressin, Steroids, and Epi, Oh my! A new cocktail for cardiac arrest?), the VAM-IHCA trial2 compared the addition of both methylprednisolone and vasopressin to normal saline placebo, given with standard epinephrine resuscitation during in hospital cardiac arrest (IHCA).
The use of methylprednisolone plus vasopressin was associated with increased likelihood of ROSC: 42% intervention vs. 33% placebo, RR 1.3 (95% CI 1.03-1.63), risk difference 9.6% (95% CI 1.1-18.0%); p=0.03.
BUT there was no increased likelihood of favorable neurologic outcome (7.6% in both groups).
Recent publication on evaluation of long-term outcomes of the VAM-ICHA trial3 showed that, at 6-month and 1-year follow-up, there was no difference between groups in:
Bottom Line: Existing evidence does not currently support the use of methylprednisolone and vasopressin as routine code drugs for IHCA resuscitation.
Basic study characteristics:
Some of the limitations:
Category: Orthopedics
Keywords: Elbow, osteochondritis, capitellum (PubMed Search)
Posted: 4/23/2022 by Brian Corwell, MD
(Updated: 4/24/2022)
Click here to contact Brian Corwell, MD
9-year-old male left hand dominant, presents with left elbow pain.
He is a future “star pitcher,” says his coach dad. “Doc, I bet you didn’t know that although only 10% of people throw with their left hand almost a 1/3rd of MLB pitchers are lefties. He is 3x more likely than a righty to pitch in MLB.” “Maybe I’m asking him to throw too much.”
Hx: Lateral elbow pain and “stiffness” worse with activity that is better with rest
PE: Lateral elbow tenderness (capitellum) with slight (approx. 20 degrees) decreased loss of extension. Minimal swelling noted.
Dx: Panner's disease refers to osteochondrosis of the capitellum (similar to Legg Calve Perthes). Likely due to AVN from repetitive trauma. May also be due to endocrine disturbances.
Affects the dominant elbow of boys between the ages of 5 and 10
Associated with the repetitive trauma of throwing or gymnastics.
Must be differentiated from osteochondrosis dissecans which occurs in the older child >13yo when the ossification of the capitellum is complete
Radiology:
The articular surface of the capitellum may appear irregular or flattened with areas of radiolucency (43%). Loose bodies not seen with Panners, much more likely with OCD lesions.
Treatment: Ice and NSAIDs. Avoid pitching/gymnastics etc. until full radiographic and clinical healing. If significant pain and/or swelling place patient in long arm posterior splint for 7-10 days. Resolution may take several months and up to one year.
Category: Critical Care
Posted: 4/19/2022 by Mike Winters, MBA, MD
(Updated: 6/22/2026)
Click here to contact Mike Winters, MBA, MD
ED Low-Tidal Volume Ventilation
Monnin KE, et al. Low tidal volume ventilation for emergency department patients: A systematic review and meta-analysis on practice patterns and clinical impact. Crit Care Med. 2022; published online Feb 7, 2022.
Category: Pediatrics
Keywords: abdominal trauma, MVC, CT scans, radiation (PubMed Search)
Posted: 4/15/2022 by Jenny Guyther, MD
(Updated: 6/22/2026)
Click here to contact Jenny Guyther, MD
Fornari M and Lawson S. Pediatric Blunt Abdominal Trauma and Point of Care Ultrasound. Pediatric Emergency Care 2021. 37 (12): 624-629.
Category: Orthopedics
Keywords: Concussion, psychiatric, hospitalization (PubMed Search)
Posted: 4/9/2022 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
A recent study investigated the association between concussion and subsequent mental health conditions in a pediatric population.
Retrospective cohort study. Pediatric patients aged 5 to 18 years who presented to an ED, PCP or mental health practitioner from April 2010, to March 2020, in Ontario, Canada.
Primary outcome: Time to first diagnosis with a mental health condition during follow-up
Secondary outcomes: 1) self-harm 2) psychiatric hospitalization 3) death by suicide.
Mental health conditions: anxiety and neurotic disorders, adjustment reactions, behavioral disorders, mood and eating disorders, schizophrenia, substance use disorder, suicidal ideation, and disorders of psychological development.
Study group, almost 450,000 patients. Age and sex matching between those with concussion and those who experienced an orthopedic injury.
A significant association (P < .001) was found between concussion and mental health conditions
A significant association emerged between concussion and self-harm and psychiatric hospitalization
No association with suicide
Conclusion: Concussion was significantly associated with risk of mental illness, psychiatric hospitalization and self-harm but not death by suicide.
Concussed patients had an almost 40% higher rate of mental health conditions compared to controls (adjusted hazard ratio 1.39)
Take home: Screen patients who return to the ED with post concussive symptoms for mental health symptoms/concerns and provide appropriate awareness for parents
Ledoux A, Webster RJ, Clarke AE, et al. Risk of Mental Health Problems in Children and Youths Following Concussion. JAMA Netw Open. 2022;5(3):e221235.
Category: Critical Care
Keywords: APRV, low tidal volume, COVID-19 (PubMed Search)
Posted: 4/5/2022 by Quincy Tran, MD, PhD
(Updated: 6/22/2026)
Click here to contact Quincy Tran, MD, PhD
During the height of the pandemic, a large proportion of patients who were referred to our center for VV-ECMO evaluation were on Airway Pressure Release Ventilation (APRV). Does this ventilation mode offer any advantage? This new randomized control trial attempted to offer an answer.
---------------
1.Settings: RCT, single center
2. Patients: 90 adults patients with respiratory failure due to COVID-19
3. Intervention: APRV with maximum allowed high pressure of 30 cm H20, at time of 4 seconds. Low pressure was always 0 cm H20, and expiratory time (T-low) at 0.4-0.6 seconds. This T-low time can be adjusted upon analysis of flow-time curve at expiration.
4. Comparison: Low tidal volume (LTV) strategy according to ARDSNet protocol.
5. Outcome: Primary outcome was Ventilator Free Days at 28 days.
6.Study Results:
7.Discussion:
8.Conclusion:
APRV was not associated with more ventilator free days or other outcomes among patients with COVID-19, when compared to Low Tidal Volume strategies in this small RCT.
Ibarra-Estrada MÁ, García-Salas Y, Mireles-Cabodevila E, López-Pulgarín JA, Chávez-Peña Q, García-Salcido R, Mijangos-Méndez JC, Aguirre-Avalos G. Use of Airway Pressure Release Ventilation in Patients With Acute Respiratory Failure Due to COVID-19: Results of a Single-Center Randomized Controlled Trial. Crit Care Med. 2022 Apr 1;50(4):586-594. doi: 10.1097/CCM.0000000000005312. PMID: 34593706; PMCID: PMC8923279.
Category: Pharmacology & Therapeutics
Keywords: haloperidol, agitation, sedation (PubMed Search)
Posted: 4/2/2022 by Ashley Martinelli
(Updated: 6/22/2026)
Click here to contact Ashley Martinelli
Diphenhydramine (B) has historically been utilized in combination with haloperidol 5mg (5) and lorazepam 2mg (2) in the treatment of acute agitation. The most common rationale for adding diphenhydramine is prevention of EPS, however literature to support this is lacking. A recently published paper examined diphenhydramine/haloperidol/lorazepam combination (B52) vs haloperidol/lorazepam combination therapy (52) to compare the need for additional agitation treatments as a surrogate for clinical efficacy.
This retrospective, multicentered noninferiority study included 400 emergency medicine patients, 200 per treatment arm. On average, the patients were 40 years old, 64% male, and predominantly Caucasian. More patients in the B52 group had psychiatric illness listed as their primary cause for agitation compared to the 52 group. The two most frequently reported substances on urine drug screens, if collected, were amphetamines (35%) and cannabinoid (35.5%).
Results:
-No difference in the use of additional agitation medications within 2 hours
-More patients in the 52 group were noted to receive anticholinergic medications within 2 days, but indications varied and were not associated with EPS treatment
The B52 combination was associated with:
---Increased length of stay 17 h (10-26) vs 13.8 h (9-12), p = 0.03
---Increased use of restraints 43% vs 26.5%, p = 0.001
---Hypotension 16% vs 3.5%, p <0.001
---Use of nasal canula oxygen 3% vs 0%, p < 0.01
The addition of diphenhydramine may not be necessary to prevent EPS in patients receiving haloperidol for agitation and is associated with increased length of stay and adverse events, likely due to its additive sedative properties.
Jeffers T, et al. Efficacy of combination haloperidol, lorazepam, and diphenhydramine vs. combination haloperidol and lorazepam in the treatment of acute agitation: a multicenter retrospective cohort study. J Emerg Med. 2022 Mar 11;S0736-4679(22)00057-9. doi: 10.1016/j.jemergmed.2022.01.009
Category: Pediatrics
Keywords: inborn error of metabolism (IEM), organic acidemia (PubMed Search)
Posted: 4/1/2022 by Rachel Wiltjer, DO
(Updated: 6/22/2026)
Click here to contact Rachel Wiltjer, DO
Laura L. Guilder, Jonathan B. Kronick; Organic Acidemias. Pediatr Rev March 2022; 43 (3): 123–134.
Category: Critical Care
Keywords: OHCA, shock, epinephine, norepinephrine, cardiac arrest (PubMed Search)
Posted: 3/23/2022 by William Teeter, MD
(Updated: 6/22/2026)
Click here to contact William Teeter, MD
The use of catecholamines following OHCA has been a mainstay option for management for decades. Epinephrine is the most commonly used drug for cardiovascular support, but norepinephrine and dobutamine are also used. There is relatively poor data in their use in the out of hospital cardiac arrest (OHCA). This observational multicenter trial in France enrolled 766 patients with persistent requirement for catecholamine infusion post ROSC for 6 hours despite adequate fluid resuscitation. 285 (37%) received epinephrine and 481 (63%) norepinephrine.
Findings
Limitations:
Summary:
Norepinephrine may be a better choice for persistent post-arrest shock. However, this study is not designed to sufficiently address confounders to recommend abandoning epinephrine altogether, but it does give one pause.
Epinephrine versus norepinephrine in cardiac arrest patients with post-resuscitation shock. Intensive Care Med. 2022 Mar;48(3):300-310. doi: 10.1007/s00134-021-06608-7.
Category: Pediatrics
Keywords: peds, chest xray, pneumonia. (PubMed Search)
Posted: 3/18/2022 by Jenny Guyther, MD
Click here to contact Jenny Guyther, MD
Lipsett, Susan C. MD*,†,‡; Hirsch, Alexander W. MD*,†; Monuteaux, Michael C. ScD*,†; Bachur, Richard G. MD*,†,‡; Neuman, Mark I. MD, MPH*,†,‡ Development of the Novel Pneumonia Risk Score to Predict Radiographic Pneumonia in Children, The Pediatric Infectious Disease Journal: January 2022 - Volume 41 - Issue 1 - p 24-30.
Category: Critical Care
Posted: 3/15/2022 by Duyen Tran, MD
(Updated: 6/22/2026)
Click here to contact Duyen Tran, MD
Acute liver failure is defined as new and rapidly evolving hepatic dysfunction associated with neurologic dysfunction and coagulopathy (INR >1.5). Most common cause of death in these patients are multiorgan failure and sepsis. Drug-induced liver injuy most common cause in US, with viral hepatitis most common cause worldwide.
Management of complications associated with acute liver failure
Montrief T, Koyfman A, Long B. Acute liver failure: A review for emergency physicians. Am J Emerg Med. 2019 Feb;37(2):329-337. doi: 10.1016/j.ajem.2018.10.032. Epub 2018 Oct 22. PMID: 30414744.
Category: Airway Management
Keywords: PRP, hematoma, muscle tear (PubMed Search)
Posted: 3/12/2022 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Treatment of Hamstring Strains in Athletes
28 year old athlete presents to the ED and diagnosed with a hamstring strain
Localized swelling, moderate pain and a small limp. Incomplete tearing of the muscle
He is worried that he will miss the remainder of his season and when he returns will reinjure the same hamstring
Consider referral to sports medicine/orthopedics
A recent study looked at use of ultrasound guided hematoma aspiration followed by platelet-rich plasma (PRP) treatment on recovery in acute hamstring injuries
55 male athletes between ages 18 -32 weighing between 170 and 260lbs
27 with treatment protocol plus rehabilitation and 28 treated conservatively (rehabilitation)
All had Grade 2 hamstring injuries diagnosed on MRI
Partial muscle tear (<50% cross sectional area)
Note: Grade 2 hamstring injuries are often associated with INTERmuscle hematoma and subsequent scarring. This can lead to persistent pain/discomfort and reinjury
Average return to play time was 32.4 days in the standard of care group
Average return to play time was 23.5 days in the intervention group (P<0.001)
Recurrence rate of hamstring strain was 28.6% in the standard of care group
Recurrence rater of hamstring strain was <4% in the intervention group (P=0.025)
Athletes with grade 2 hamstring injuries treated with hematoma aspiration and PRP injection into the strain had significantly shorter return-to-play and much lower recurrence rate that athletes treated with rehabilitation alone
Trunz LM, et al. Effectiveness of Hematoma Aspiration and Platelet-rich Plasma Muscle Injections for the Treatment of Hamstring Strains in Athletes. Med Sci Sports Exerc. 2022 Jan 1;54(1):12-17.
Category: Pediatrics
Keywords: SCIWORA, trauma, pediatrics, myelopathy (PubMed Search)
Posted: 3/4/2022 by Natasha Smith
Click here to contact Natasha Smith
Pediatric spines are elastic in nature.
SCIWORA is a syndrome with neurological deficits without osseous abnormality on XR or CT.
Many patients with SCIWORA have myelopathy.
Mechanism of injury: Most commonly caused by hyperextension or flexion. Other possible mechanisms include rotational, lateral bending, or distraction.
Population: More common in younger children. This comprises 1/3 of pediatric trauma cases that have neuro deficits on exam.
Severity depends on degree of ligamentous injury. It can be mild to severe, and cases have the potential to be unstable.
Management: Immobilize cervical spine and consult neurosurgery. Patients often need prolonged spinal immobilization.
If the patient is altered and an adequate neurological exam cannot be obtained, a normal CT or XR of the cervical spinal is not sufficient to rule out spinal cord injury. It is important to continue monitoring neurological status. One possible etiology is spinal cord hemorrhage, and serial exams are essential.
Nagler J, Farrell CA, Auerbach M et al. "Trauma." Atlas of Pediatric Emergency Medicine, edited by Binita S, 3rd edition. McGraw Hill, 2019, 996-997.
Category: Critical Care
Keywords: Mechanical Ventilation, PEEP (PubMed Search)
Posted: 3/2/2022 by Mark Sutherland, MD
Click here to contact Mark Sutherland, MD
How to set the correct PEEP remains one of the most controversial topics in critical care. In fact, just on UMEM Pearls there are 55 hits when one searches for PEEP, including this relatively recent pearl on PEEP Titration.
A recent Systematic Review and Network Meta-Analysis looked at existing trials on this issue. They found that:
1) Higher PEEP strategies were associated with a mortality benefit compared to lower PEEP strategies
2) Lung Recruitment Maneuvers were associated with worse mortality in a dose (length of time of the maneuver) dependent fashion.
This fits with recent literature and trends in critical care and bolsters the feeling many intensivists are increasingly having that we may be under-utilizing PEEP in the average patient.
Bottom Line: As an extremely broad generalization, we would probably benefit the average patient by favoring higher PEEP strategies, and avoiding lung recruitment maneuvers. Do keep in mind that it is probably best to continue lower PEEP strategies in patient populations at high risk of negative effects of PEEP (e.g. COPD/asthma, right heart failure, volume depleted with hemodynamic instability, bronchopleural fistula) until these groups are specifically studied.
Dianti J, Tisminetzky M, Ferreyro BL, Englesakis M, Del Sorbo L, Sud S, Talmor D, Ball L, Meade M, Hodgson C, Beitler JR, Sahetya S, Nichol A, Fan E, Rochwerg B, Brochard L, Slutsky AS, Ferguson ND, Serpa Neto A, Adhikari NK, Angriman F, Goligher EC. Association of PEEP and Lung Recruitment Selection Strategies with Mortality in Acute Respiratory Distress Syndrome: A Systematic Review and Network Meta-Analysis. Am J Respir Crit Care Med. 2022 Feb 18. doi: 10.1164/rccm.202108-1972OC. Epub ahead of print. PMID: 35180042. https://pubmed.ncbi.nlm.nih.gov/35180042/
Category: Orthopedics
Keywords: knee osteoarthritis, plain film (PubMed Search)
Posted: 2/26/2022 by Brian Corwell, MD
(Updated: 6/22/2026)
Click here to contact Brian Corwell, MD
The knee is one of the most commonly affected joints from osteoarthritis (OA).
Patients will complain of knee pain, swelling and stiffness.
This leads to disability as it interferes with walking, using stairs at home and getting in and out of chairs and the bath without assistance.
Increasing incidence due to aging of the general population and rising rates of obesity.
Patients frequently present to the ED for knee pain and imaging is often obtained.
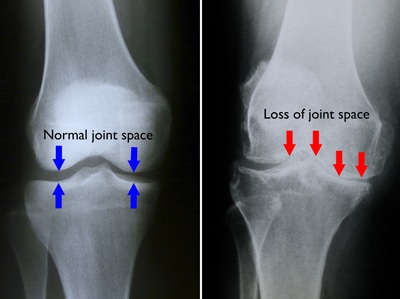
Diagnosis of knee OA can be made with an appropriate history and imaging that shows osteophytes and joint space narrowing.
The best views for knee OA include 1) PA weight-bearing & 2) 45 degree of knee flexion
https://d3i71xaburhd42.cloudfront.net/6f8ce215fb4bcd153a478187c9a6a2ae652a5fc4/250px/1-FigureI-1.png
Note: Weight-bearing radiographs will demonstrate greater joint space narrowing than non-weight-bearing radiographs
Of the 3 compartments of the knee, the medial tibiofemoral compartment is most commonly affected > patellofemoral compartment > lateral tibiofemoral compartment.
Examples of knee OA
https://roberthowells.com.au/wp-content/uploads/2016/04/A00212F02.jpg
https://orthoinfo.aaos.org/link/e7e6933819db4020bc2f3822c45c538f.aspx
Category: Critical Care
Posted: 2/22/2022 by Mike Winters, MBA, MD
(Updated: 6/22/2026)
Click here to contact Mike Winters, MBA, MD
Hyperglycemic Hyperosmolar State (HHS)
Long B, Willis GC, Lentz S, et al. Diangosis and management of the critically ill adult patient with hyperglycemic hyperosmolar state. J Emerg Med. 2021;61:365-75.
Category: Pediatrics
Keywords: pediatric trauma, complications (PubMed Search)
Posted: 2/18/2022 by Jenny Guyther, MD
Click here to contact Jenny Guyther, MD
Khalil M, Alawwa G, Pinto F, O'Neill PA. Pediatric Mortality at Pediatric versus Adult Trauma Centers. J Emerg Trauma Shock. 2021 Jul-Sep;14(3):128-135. doi: 10.4103/JETS.JETS_11_20. Epub 2021 Sep 30. PMID: 34759630; PMCID: PMC8527062.
Category: Visual Diagnosis
Posted: 2/12/2022 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
23 y/o otherwise healthy Male presents for approx. 3 month history of Right leg mass. It is painful with activity (deep and sharp) but not enlarging. Patient remembers a fall from a bicycle 6 months ago, with negative imaging for fracture.
What is the diagnosis?
https://plinthsandplatforms.files.wordpress.com/2016/06/screen-shot-2016-06-20-at-10-58-18-am.png
https://radsource.us/wp-content/uploads/2019/02/1E.jpg
Myositis Ossificans
{kind=link}
{kind=link}
{kind=link}
{kind=link}