A leading cause of cardiac arrest in patients 40 years and younger is due to drug poisoning. Adverse cardiovascular events (ACVE) such as myocardial injury (by biomarker or ECG), shock (hypotension or hypoperfusion requiring vasopressors), ventricular dysrhythmias (ventricular tachycardia/fibrillation, torsade de pointes), and cardiac arrest (loss of pulse requiring CPR) are responsible for the largest proportion of morbidity and mortality overdose emergencies. Clinical predictors of adverse cardiovascular events in drug overdose in recent studies include:
Bottom line:
Obtain ECG and perform continuous telemetry monitoring in overdose patients with above risk factors. Patients with two or more risk factors have extremely high risk of in-hospital adverse cardiovascular events and intensive care setting should be considered.
Benign headaches are common in bodybuilders. However, several less benign headaches are worth noting:
All except the first two are exclusively reported in patients on anabolic steroids, growth hormone, and/or “energy” supplements. Make sure to ask your patient about these risk factors.
Which septic patients should receive empiric antifungal therapy?
Patients with fungemia only make up about 5% of patients presenting with septic shock, but invasive fungal infections are associated with increased hospital mortality (40-50%), prolonged ICU and hospital length of stay, and increased costs of care.1
The EMPIRICUS trial showed no mortality benefit to empiric antifungals for all, even patients with candidal colonization and recent exposure to antibiotics.2
Bottom Line
Therapy should always be tailored to the specific patient, but providers should strongly consider admininistering empiric echinocandin (micafungin, caspofungin) over fluconazole in patients with severe sepsis/septic shock and:
*Especially consider addition of antifungal in patients who do not show improvements after initial management with IVF and broad spectrum antibiotics in the ED.*
The search for an objective reliable test for mild traumatic brain injury found an early promising result last week.
May be arriving in your hospital in the near future.
A handheld sideline version is sure to follow
The FDA approved the first blood test for concussion/mild TBI
Called the Banyan BTI (Brain Trauma Indicator)
This test measures 2 neural protein biomarkers released into the blood following mild TBI
The FDA approved this test within 6 months after reviewing data on just under 2,000 blood samples.
They concluded the Banyan BTI can predict the absence of cranial CT lesions with an accuracy greater than 99% and may reduce imaging in up to a 1/3rd
Be optimistic but consider the small sample size and remember that this test looks for biomarkers and may miss subtle cases where proteins didn’t leak. This test is NOT ready to be used for return to play decisions. It takes 3 to 4 hours to result and costs about $150. Other biomarkers are being investigated and may prove to be better
https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm596531.htm
Abnormal ocular movement (e.g. nystagmus) can often be observed in select CNS pathology.
Certain drugs/toxin overdose can also induce nystagmus.
In an "unknown" intoxication, physical exam findings such as nystagmus may help narrow the identity of the suspected ingestion/overdose.
-Nonischemic cardiomyopathy, classically seen in post-menopausal women preceded by an emotional or physical stressor
-Named for characteristic appearance on echocardiography and ventriculography with apical ballooning and contraction of the basilar segments of the LV – looks like a Japanese octopus trap or “takotsubo" (pot with narrow neck and round bottom)
-Clinical presentation usually similar to ACS with chest pain, dyspnea, syncope, and EKG changes not easily distinguished from ischemia (ST elevations – 43.7%, ST depressions, TW inversions, repol abnormalities) and elevation in cardiac biomarkers (though peak is typically much lower than in true ACS)
** Diagnosis of exclusion – only after normal (or near-normal) coronary angiography **
-Care is supportive and prognosis is excellent with full and early recovery in almost all patients (majority have normalization of LVEF within 1 week)
-Supportive care may include inotropes, vasopressors, IABP, and/or VA ECMO in profound cardiogenic shock
** LVOT Obstruction **
-occurs in 10-25% of patients with Takotsubo’s cardiomyopathy
-LV mid and apical hypokinesis with associated hypercontractility of basal segments of the LV predisposes to LV outflow tract obstruction
-Important to recognize as it is managed differently:
-may be worsened by hypovolemia, inotropes, and/or systemic vasodilatation
-mainstay of treatment is avoidance of the above triggers/exacerbating factors while increasing afterload
*phenylephrine is agent of choice +/- beta blockade
Take Home Points:
***Diagnosis of exclusion!!! Presentation very similar to ACS and ACS MUST be ruled out
* Treatment is supportive and similar to usual care for cardiogenic shock. Can be severe and require mechanical circulatory support!
*10-25% have LVOT obstruction. Manage with phenylephrine +/- beta blockade
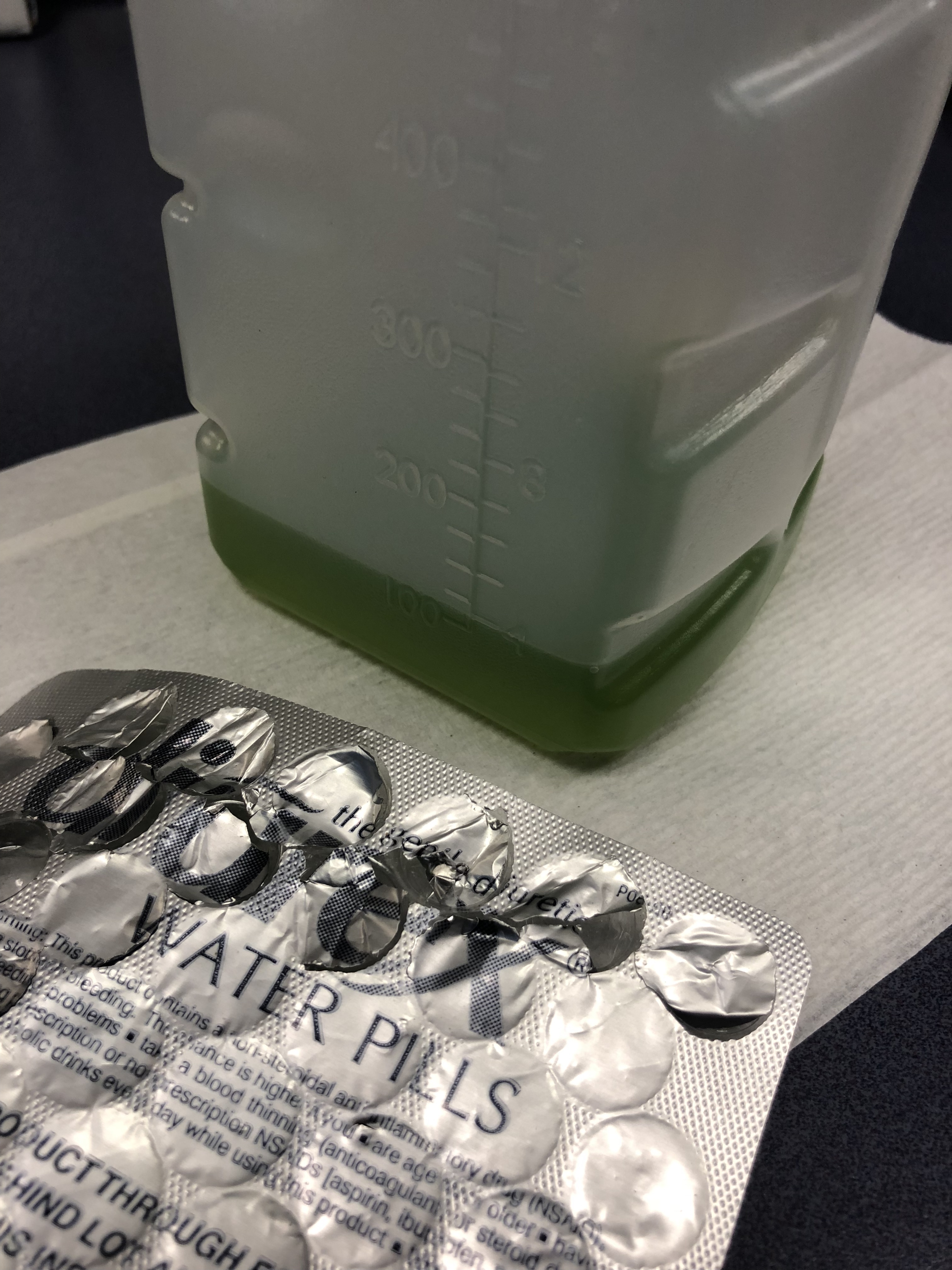
75 y/o M is brought in by EMS after he fell off the light rail and hit his head. In the ED he is A&Ox3, and is asking for a urinal. Two minutes later the tech comes running to show you the following:
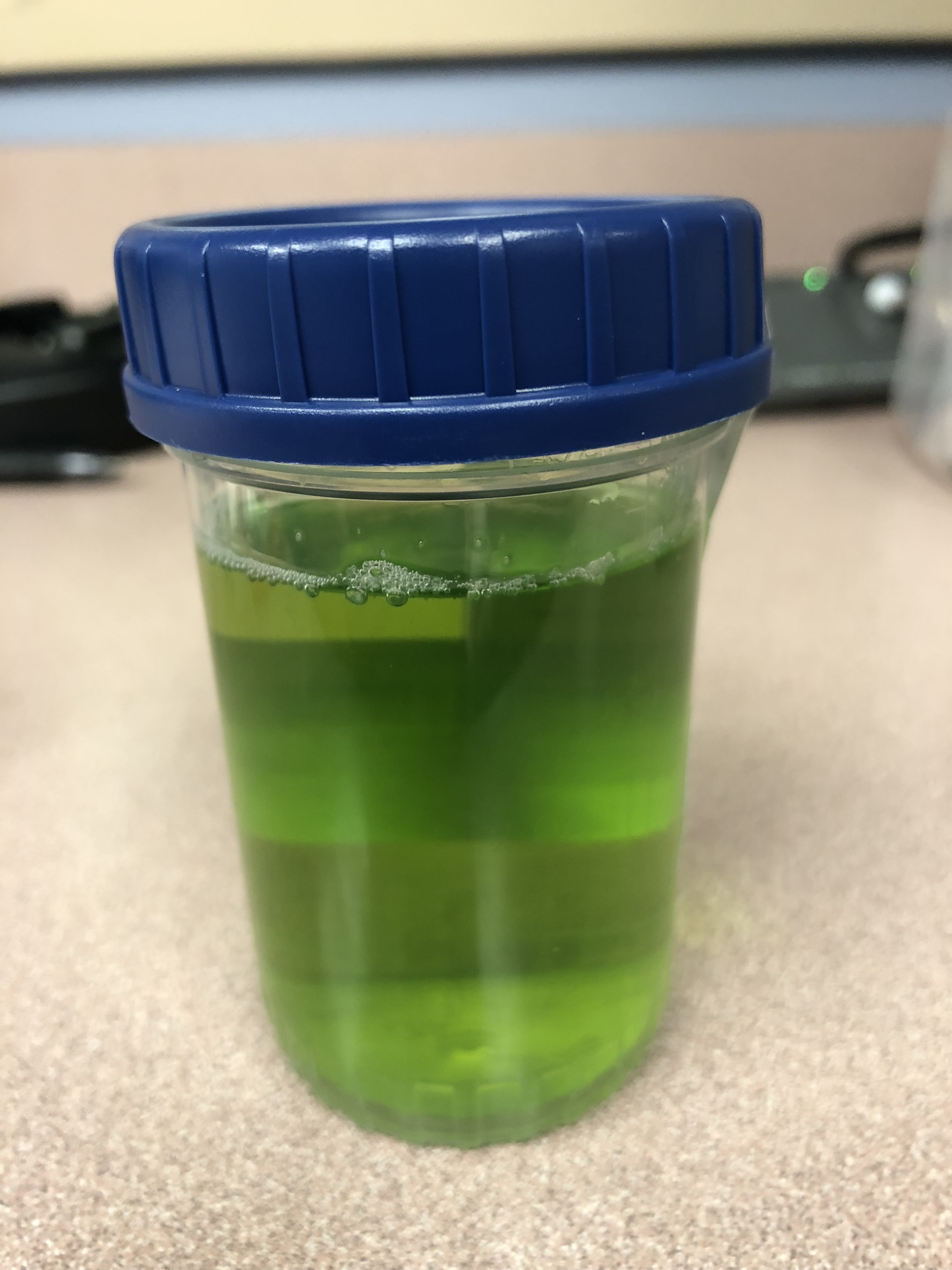
What is the cause of this patients Jolly Rancher Green Apple looking urine sample?
Patient: 11 month old with trouble breathing and color change after a family member sprayed air freshener. Symptoms have since resolved.
What are you concerned about in the attached xrays?
Bupropion (Wellbutrin, Zyban) is unique monocyclic antidepressant and smoking cessation agent that is structurally similar to amphetamines. Bupropion blocks dopamine and norepinephrine reuptake and antagonizes acetylcholine at nicotinic receptors.
Bottom line:
Bupropion is a common cause of drug induced seizures but in severe overdose can also cause prolonged QTc and wide complex ventricular dysrhythmia that may be responsive to sodium bicarbonate. All patients with an overdose of bupropion should have an ECG performed and cardiac monitoring to watch for conduction delays and life-threatening arrhythmias.
Femoral neck stress fractures
Adults>kids
Represents 5% of all stress fractures
Usually due to repetitive abductor muscle contraction
As with all stress fractures can occur in 2 types
1) Insufficiency type (normal physiologic stress on abnormal bone)
2) Fatigue type (abnormal/excessive physiologic stress on normal bone)
2 locations on interest:
1) Compression side (inferior femoral neck)
2) Tension side (superior femoral neck)
History: Insidious onset of groin or lateral hip pain associated with weight bearing
Exam: Antalgic gait, pain with hip log roll and with FABER (hip flexion, Abduction and external rotation test)
Treatment:
Compression side: reduced weight bearing and activity modification
Tension side: Non weight bearing (due to high risk of progression to displacement with limited weight bearing) AND surgical consultation for elective pinning to prevent displacement. If displaced, will require ORIF
Case: 5 year old presents to the ED with 2 weeks of fever. She has extensive cracked, bleeding lips and a rash on her hands and feet. She was recently diagnosed with “walking pneumonia” and hand, foot and mouth disease this week. Her pediatrician sent her in for further workup after she was found to have an elevated CRP on outpatient labs. A similar picture appears in the link below:
What's the diagnosis?
Hyperoxia and the Post-Arrest Patient
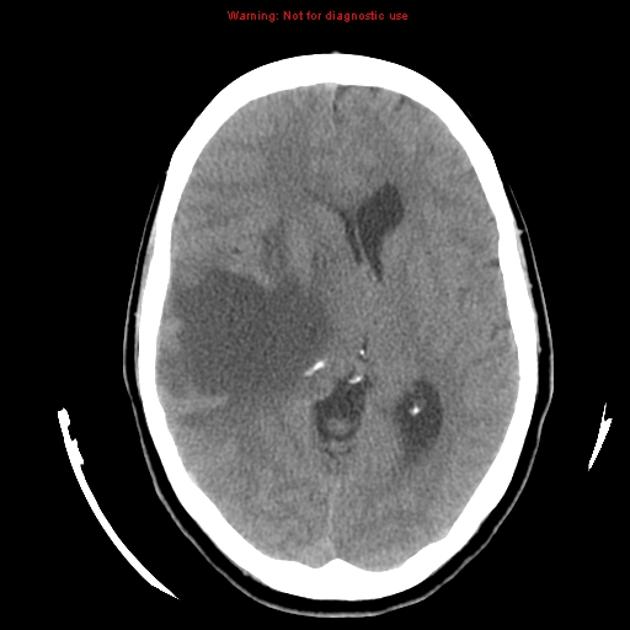
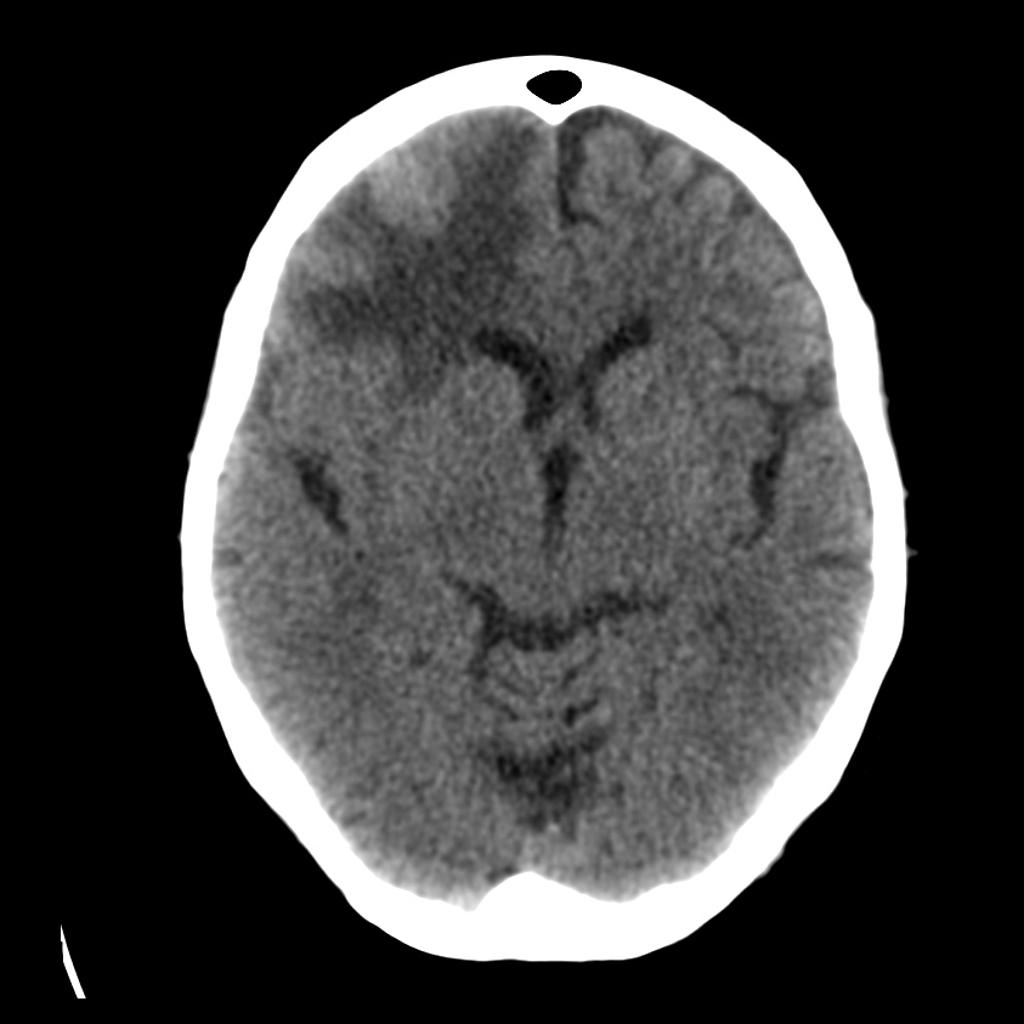
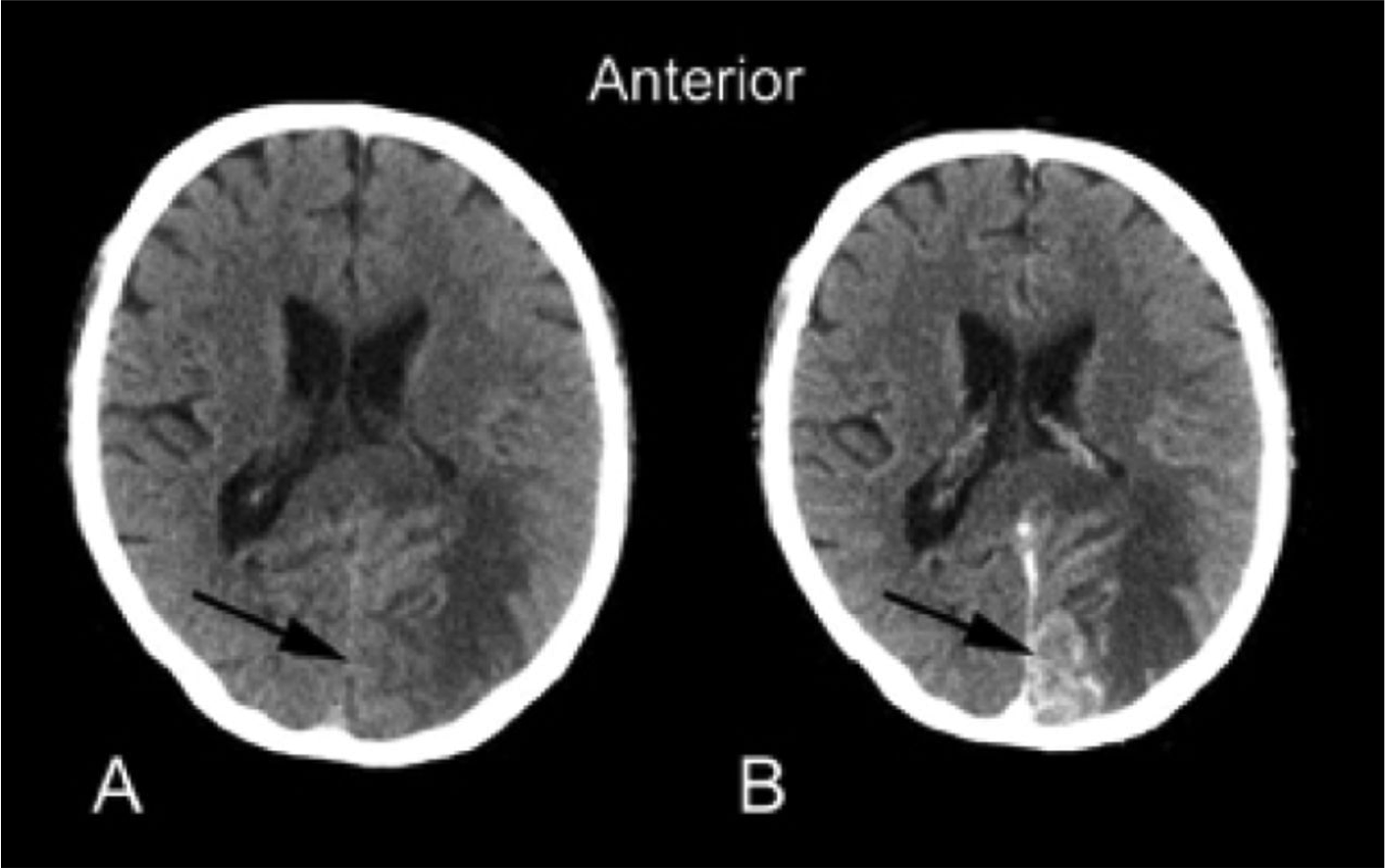
15% of older adults presenting to ED for dizziness have serious etiologies; 4-6% are stroke-related and sensitivity of CT for identifying stroke or intracranial lesion in dizziness is poor (16%), so if CNS etiology suspected, seek neuro consult or MRI (83% sensitivity)
Debating between cefepime or piperacillin/tazobactam for your septic patient? Use this table to help you decide.
|
|
| Cefepime | Piperacillin/Tazobactam |
| Gram Negative Spectrum | Pseudomonas aeruginosa | Yes | Yes |
| Aerobic gram negative organisms | E. coli Klebsiella sp. Proteus mirabilis M catarrhalis H. influenza | E. coli Klebsiella sp. Proteus mirabilis M. catarrhalis H. influenza | |
| Anerobic gram negative organisms | No | B. fragilis
| |
| Gram Positive Spectrum | MRSA | No | No |
| Aerobic gram positive organisms | MSSA CoNS Group A Strep S. pneumoniae
| MSSA CoNS Group A Strep S. pneumoniae E. faecalis | |
| Anaerobic gram positive organisms | P. acnes Peptostreptococci | P. acnes Peptostreptococci Clostridium sp. | |
| Infection Site Concerns | CNS Penetration | Yes | No1 |
| Urine Penetration | Yes | Yes | |
| Lung Penetration | Yes | Low2 | |
| Dosing Frequency (Normal Renal Function) | Q8h | Q6h | |
1. Tazobactam CNS penetration is limited, thus limiting antipseudomonal activity in the CNS
2. Low pulmonary penetration, may not achieve therapeutic levels in patients with critical illness
 Your patient is an18 months old female with intermittent abdominal pain for the last 4-5 days. She has history of constipation and soy allergy, seen at an outside hospital three days ago for the same. She had an xray and was discharged home with instructions for at home clean out with diagnosis of constipation.
Your patient is an18 months old female with intermittent abdominal pain for the last 4-5 days. She has history of constipation and soy allergy, seen at an outside hospital three days ago for the same. She had an xray and was discharged home with instructions for at home clean out with diagnosis of constipation.
Mother is bringing her to your ED because the pain is back. The laxatives helped somewhat, but her symptoms have returned. She reports that the patient cries spontaneously, lasting 1-2 minutes, then completely resolves. These episodes happen at multiple times during the day.
ROS: Decreased appetite and energy, but NO fevers, vomiting, diarrhea, bloody stool, abdominal distension, hematuria, or lethargy.
47 year old woman presents with cough, headache, weakness, and low grade fever. Her symptoms have been present for several days. Vital signs are temperature 99.9 F, HR 96, RR 16, BP 140/88, Pulse Ox 98%. Physical exam is nonfocal. She is Influenza negative. She is treated with Ibuprofen and oral fluids. Upon discharge she mentions she is having difficulty hearing and feels dizzy. Upon further questioning she admits to ringing in her ears. What tests should you order?
As hospital volumes increase and ED patient boarding becomes more commonplace, emergency physicians may find themselves managing critically ill patients beyond the initial resuscitation.
The benefit of glucocorticoids in critically ill patients with septic shock has remained a topic of controversy for decades due to conflicting studies, including the 2002 Annane trial and the 2008 CORTICUS trial, which had opposing results when it came to the mortality benefit of steroids.
The results of the eagerly-awaited ADRENAL trial, a multicenter randomized controlled trial investigating the benefit of steroids in septic shock, were released earlier this month:
Take Home Points:
1. Administration of standard daily dose hydrocortisone by infusion does not seem to affect mortality in septic shock.
2. Emergency providers should continue to consider stress-dose steroids in patients with shock and a high risk of adrenal insufficiency (e.g., chronic steroid therapy, genetic disorders, infectious adrenalitis, etc).
Dental Avulsion in the field/sporting event
- Only replace avulsed secondary teeth
- Handle the tooth by the crown only
- Rinse tooth with cold running water gently (the root should not be wiped)
- Immediate attempt to reimplant permanent tooth into socket by 1st capable person:
* Time is tooth: Each minute tooth is out of socket reduces tooth viability by 1%
* Best chance of success if reimplant done within 5–15 min*? Poor tooth viability if avulsed for >1 hr
- If unsuccessful, place tooth in a transport solution (from most to least desirable):
- Hanks balanced salt solution (HBSS)
* Balanced pH culture media available commercially in the Save-A-Tooth kit
* Effective hours after avulsion
- Cold milk:
* Best alternative storage medium
* Place tooth in a container of milk that is then packed in ice (prevents dilution)
- Saliva:
* Store in a container of parent or child's saliva
- Never use tap water or dry transport