Hyponatremic Encephalopathy
Febrile seizures occur in children 6 months through 5 year olds. A complex febrile seizure occurs when the seizure is focal, prolonged (> 15 min), or occurs more than once in 24 hours.
The prevalence of bacterial meningitis in children with fever and seizure after the H flu and Strep pneumomoniae vaccine was introduced is 0.6% to 0.8%. The prevalence of bacterial meningitis is 5x higher after a complex than simple seizure.
From the study referenced, those children with complex febrile seizures who had meningitis all had clinical exam findings suggestive of meningitis. More studies are needed to provide definitive guidelines about when lumbar punctures are needed in these patients.
In patients presenting to the ED with suicidal ideation, physicians should not use currently available risk-assessment tools in isolation to identify low-risk patients who are safe for discharge. The best approach to determine risk is an appropriate psychiatric assessment and good clinical judgment, taking patient, family, and community factors into account. (Level C Recommendation, based upon the quality of the research.)
Catastrophic Antiphospholipid Syndrome (CAPS):
A life-threatening “thrombotic storm” of multi-organ micro & macro thrombosis in patients with antiphospholipid syndrome (known or unknown).
Triggered circulating antibodies (usually by infection, but can be prompted by malignancy, pregnancy, and lupus itself) cause endothelial disruption and inflammation leading to prothrombotic state, commonly with SIRS response.
Mortality is high at an estimated 40%.
Confirm diagnosis with antiphospholipid antibody titers.
Treat ASAP with unfractionated heparin, corticosteroids, and Hematology consultation for plasma exchange and/or IVIG.
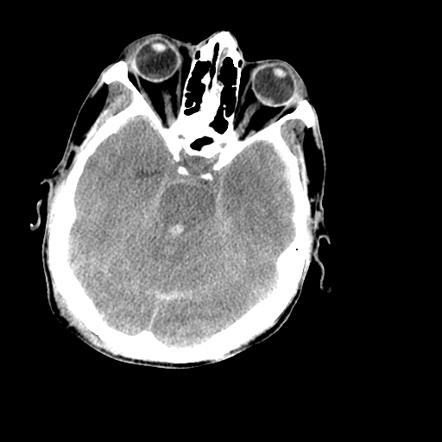
Bottomline: Keep pituitary apoplexy in your differential when considering SAH or meningitis, especially in the presence of risk factors, and have a low threshold to order an MRI.
Take Home Point: In patients with diabetic gastroparesis, haloperidol may be an effective adjunctive treatment to prevent hospitalizations and reduce opioid requirements.
Patients with psychiatric disorders are found globally, with a recent global burden of disease estimate that mental illness accounted for 32.4% of years lived with disability and 13.0% of disability-adjusted life-years.
The American College of Emergency Physicians just published a methodological rigorous clinical policy entitled “Critical Issues in the Diagnosis and Management of the Adult Psychiatric Patient in the Emergency Department.”
One question they sought to answer was “In the alert adult patient presenting to the ED with acute psychiatric symptoms, should routine laboratory tests be used to identify contributory medical conditions (nonpsychiatric disorders)?”
Their assessment was: “Do not routinely order laboratory testing on patients with acute psychiatric symptoms. Use medical history, previous psychiatric diagnoses, and physician examination to guide testing.” This was a Level C recommendation, based upon the quality of the research.
Bottom Line: Current literature does not support routinely ordering laboratory testing on patients with acute psychiatric symptoms. However, the quality of the evidence was not strong and local clinical context should be considered.
--RV systolic function is negatively affected by high RV afterload
--High mean airway pressures on the ventilator (particularly in modes such as APRV [airway pressure release ventilation]) can induce RV dysfunction
*****CLICK BELOW FOR A GREAT CASE!!!*****
The answer appears to be ... it depends.
Early Oseltamivir Treatment in Influenza in Children1-3 Years of Age: A Randomized Controlled Trial
A study in 2010 out of Finland by Heinonen, et al showed that if given in the first 12 hours of symptom onset to otherwise healthy pediatric patients between the age of 1-3 years:
- decrease incidence of acute otitis media by 85%
- no difference if given within 24 hours
Among children with influenza A, oseltamivir started within 24 hours of symptom onset
- shortened medium time to resolution of illness by 3.5 days (3.0 versus 6.5) in all children
- shortened median time to resolution of illness by 4.0 days in UNvaccinated children
- Reduced parental work absenteeism by 3 days
* no differences were seen in children with influenza B *
Limitations***
- Single Center study in Finland
- The authors received support from the drug manufacturer
- The sample size of children with confirmed influenza cases with small (influenza A: 79, influenza B: 19)
Takeaway:
If you have a patient between the age of 1-3 years with very early symptoms concerning for flu, a positive rapid influenza A test could allow you to cut her symptoms by 3 days, prevent complications, and allow parents to go back to work sooner.
Patients with severe salicylate poisoning may require endotracheal intubation due to fatigue from hyperventilation or mental status change.
A previously published study (Stolbach et al. 2008) showed that mechanical ventilation increases the risk of acidemia and clinical deterioration.
A small retrospective study investigated the impact of hemodialysis (HD) in intubated patients with salicylate poisoning.
Findings:
53 cases with overall survival rate of 73.2%
In patients with salicylate level > 50 mg/dL
If salicylate level > 80 mg/dL
Bottom Line:
There is moratality benefit of HD in intubated salicylate-poisoned patient.
Improving Resuscitation Performance
PCL injuries can sometimes have involvement of the posterolateral corner (PLC)
The dial test can be used to diagnose posterior lateral instability and help differentiate it from isolated PCL injuries
The dial test involves comparing the amount of external rotation of the lower leg at the knee while the knees are in 30° and in 90° of knee flexion.
https://www.youtube.com/watch?v=rnk62Y-nDSQ
An isolated injury to the posterolateral corner will result in more than 10° of external rotation in the injured knee that is present at 30° but not at 90° of knee flexion.
http://www.kneejointsurgery.com/wp-content/uploads/2015/06/DIAL-TEST.jpg
http://www.kneejointsurgery.com/wp-content/uploads/2015/06/DIAL-TEST-90.jpg
Ventricular shunt (VP) malfunction can be severe and life-threatening and evaluation has typically included a dry CT brain and a shunt series which includes multiple x-rays of the skull, neck, chest and abdomen. The goal of this study was to decrease the amount of radiation used in the evaluation of these patients since these patients will likely present many times over their lifetime. Several institutions have more towards a rapid cranial MRI, however, this modality may not be readily available.
This multidisciplinary team decreased the CT scan radiation dose from 250mA (the reference mA in the pediatric protocol at this institution) to 150 mA which allows for a balance between reducing radiation exposure and adequate visualization of the ventricular system. They also added single view chest and abdominal x-rays.
The authors found that after implementing this new protocol, there was a reduction in CT radiation doses and number of x-rays ordered with no change in the return rate.
Vaginal douching is a common and potentially dangerous practice. Women engage in this practice predominately for personal hygiene reasons but also with the false belief it will prevent or treat infections and for contraception. Numerous public health agencies and medical societies discourage douching as it has been associated with many adverse outcomes including pelvic inflammatory disease, bacterial vaginosis, cervical cancer, low birth weight, preterm birth, human immunodeficiency virus transmission, sexually transmitted diseases, ectopic pregnancy, recurrent vulvovaginal candidiasis, and infertility.
An increasing fad is the use of intravaginal detox products. Claiming to enhance female health by removing toxins, these mesh cloth-covered balls containing herbs such as mothersworth, osthol, angelica, borneol, and rhizoma, not FDA-approved, are inserted into the vagina for 3 days. Clinical experience demonstrates these products decompose into numerous pieces which become scattered retained intravaginal foreign bodies, cause mucosal irritation, and thereotically could serve as a nidus for serious infections.
When surveyed, half of general medicine patients interviewed stated that they would prefer to have a loved one present if they were to develop cardiac arrest and require CPR. So far, studies have demonstrated that…
Allowing family presence during CPR is associated with the following benefits to family members:
And is NOT associated with a difference in:
Take Home Points:
Hydrogen peroxide (H2O2) is a common household liquid that is used for wound irrigation/antiseptic and cosmetic purposes. The concentration of household product is 3% to 5% and is considered to be relatively safe except in large volume ingestion.
High-concentration H2O2 (>10%) is commercially available as “food grade” (35%) that is diluted for household use or for alternative medicine therapy (i.e. hyperoxygenation).
Ingestion of high-concentration of H2O2 can result in caustic injury as well as ischemic injury from gas embolism.
Ingestion of 1 mL of 3% H2O2 produces 10 mL of O2 gas while 1 mL of 35% H2O2 produces 115 mL of O2 gas.
Common symptoms/findings of H2O2 ingestions includes:
A retrospective review of >10% H2O2 ingestion from National Poison Data System showed:
Management
50 YOF with acute onset of worst headache of life associated with nausea and vomiting. Patient is somnolent, will rouse to noxious stimuli and complains of a headache as well as decreased vision.
Idiopathic osteonecrosis of the femoral head
Children as young as 2 or as old as 12 but generally 4 to 8 (worse in older children)
Fare better than adults with osteonecrosis of femoral head
1 in 10,000
4-5x more common in males, much less common ini African Americans
Unilateral femoral head involvement 90% of the time (Bilateral 10% of the time)
Long term consequences are deformity and arthritis
Typical presentation: Subacute limping for weeks (Painless)
As activity worsens limp, it is maximal at the end of the day (Intermittent)
As in adults with hip pathology, IF pain is reported, it is located at the upper anterior thigh and groin
On examination, look for restriction in range of motion of the hip (compare with contralateral side)
May only present with mild to moderate decreased range of motion of the hip
30 versus 60 degrees for example
ABduct both legs with pelvis in neutral OR Place one hand on contralateral pelvis and ABduct affected leg with other hand.

{kind=link}
{kind=link}