Preoxygenation in Critically Ill Patients
The Beers' Criteria lists 34 classes of medications that may be potentially inappropriate for geriatric patients due to a high risk of complications including increased risk for falls. When prescribing medications from the emergency department in geriatric patients, try to avoid these categories if other options are available.
http://www.americangeriatrics.org/files/documents/beers/BeersCriteriaPublicTranslation.pdf
The addition of diazepam to naproxen for patients with acute, nontraumatic, nonradicular lower back pain did not improve pain or functional outcomes at 1 week or 3 months after ED discharge compared to placebo.
Excited delirium syndrome (EDS) is a life-threatening condition caused by a variety of factors including drug intoxication. EDS is defined as altered mental status, hyperadrenergic state, and combativeness or aggressiveness. It is characterized by tolerance to significant pain, tachypnea, diaphoresis, severe agitation, hyperthermia, non-compliance or poor awareness to direction from police or medical personnel, lack of fatigue, superhuman strength, and inappropriate clothing for the current environment. These patients are at high risk for sudden death. Toxins associated with this syndrome include:
Ketamine at 4mg/kg dose can be given by intramuscular route and has been demonstrated to be safe and effective treatment for EDS.
Emergency department crowding is an almost universal problem. Whether it is called "access block" (Austalia) or "boarding" (United States), it is seen everywhere.
The American College of Emergency Physicians (ACEP) states that "a “boarded patient” is defined as a patient who remains in the emergency department after the patient has been admitted to the facility, but has not been transferred to an inpatient unit."
It should be clear that the primary cause of overcrowding is boarding: the practice of holding patients in the emergency department after they have been admitted to the hospital, because no inpatient beds are available. This practice has been shown to have an adverse impact on patients, with longer delays causing greater morbidity and mortality.
ACEP has created resources to help address this issue, including an emergency medicine practice paper on high impact solutions. See: file:///Users/jhirshon/Downloads/EMPC_Crowding%20IP_092016%20(1).pdf
A recently published study adds to the growing body of literature supporting the use of IV//IM ketamine as a first line agent for the control of the acutely agitated patient. In this observational cohort Riddell et al found patients given ketamine more frequently achieved adequate sedation at both 5 and 10 minutes compared to benzodiazepines, Haloperidol, given alone or in combination. This rapid sedation was achieved without an increase in the need for additional sedation or the rate of adverse events.
The Essex-Lopresti injury pattern is the lesser known of the triad of forearm injuries (Monteggia & Galeazzi).
It follows the “rule of the ring” aka the life saver candy rule: You can’t break a life saver in just one place.
These injury patterns are frequently missed because our eyes are drawn to the fracture and miss the associated dislocation.
The Essex-Lopresti fracture pattern involves a fracture of the radial head with concomitant dislocation of the distal radio-ulnar joint (DRUG)
-With associated interosseous membrane disruption
Think of it as the Maisonneuve fracture of the forearm.
Mechanism: fall from height/high energy forearm trauma.
PE: Suspect if patient has significant tenderness at the DRUG with a radial head fx.
Patients have worse outcomes if injury is missed on initial presentation due to radial migration and instability.
Take home point: Remember the rule of the ring. Remember to exam the elbow with wrist injuries and the wrist with all elbow injuries
Treatment of Low Back Pain
A recent recommendation from the American College of Physicians (Internal Medicine) now recommends nonpharmacologic therapies as the first line treatment of acute or subacute lower back pain lasting 12 weeks or less. This might bring more people to our Emergency Departments so it is important that we know their current recommendations.
Some nonpharmacologic therapies recommended are:
For acute back pain they recommend:
For chronic back pain:
A 12 year old with arm pain after doing push ups during gym class. What is the diagnosis?
The current opioid epidemic is considered the worst drug crisis in American history responsible for 50,000 deaths per year in the US from overdose of heroin and opioid prescription drugs. A 200% increase in the rate of overdose deaths involving opioids occurred between 2000 and 2014. The continued rise in opioid related deaths calls for an urgent need for treatment. Three types of medication-assisted therapies (MATs) are available for treating patients with opioid addiction:methadone, buprenorphine, and naltrexone. Suboxone a combination of buprenorphine and naloxone, is emerging as one of the best choices for the following reasons:
Congenital infection with the Zika virus is associated with 5 types of birth defects
· These are rarely or never seen with other infections during pregnancy
· These defects are:
1. Severe microcephaly (small head size) resulting in a partially collapsed skull
2. Decreased brain tissue with brain damage
3. Damage to the back of the eye with a specific pattern of scarring and increased pigment
4. Limited range of joint motion, such as clubfoot
5. Too much muscle tone restricting body movement soon after birth
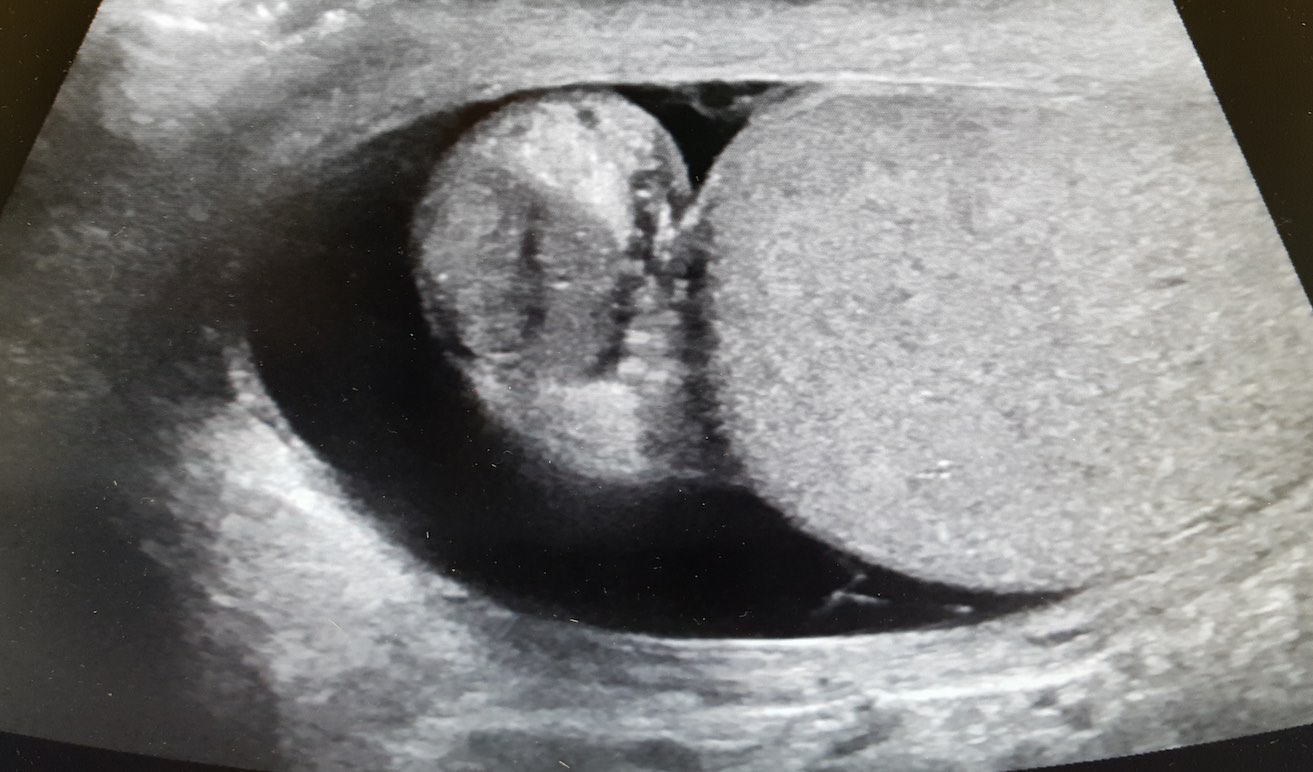
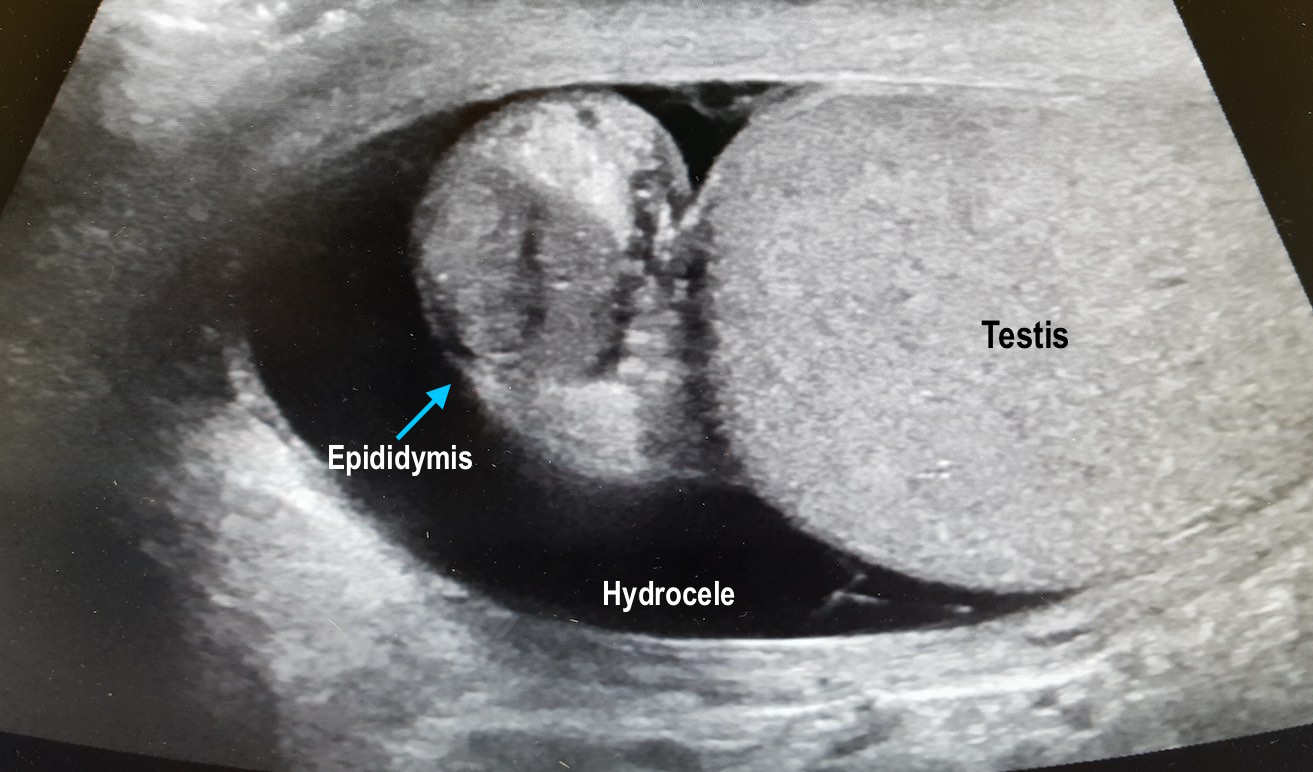
Sepsis Mimics
56 year-old male with history of hypertension presents with complaints of right scrotal swelling and pain. Denies any urinary symptoms, abdominal pain, nausea/vomiting or change in bowel habits or prior episodes. Temp was 99.0.
A scrotal ultrasound was done and an image of the right testis was seen (below). What's the diagnosis?
Is that a fracture or a growth plate?
Pediatric elbow x-rays are complicated to interpret due to the large number of ossification centers.
Elbow trauma is common in pediatrics.
Ossification centers of the elbow appear in a reliable chronologic pattern which aids in distinguising fractures from growth plates.
Note the age ranges are an estimate with great variability. For example, girls can develop these up to 2 years earlier than boys.
The numbers 1/3/5/7/9/11 correspond to the average age of development of each ossification center
Years of fusion shown below in ()
Capitellum (12-14yo)
Radial head (14-16yo)
Medial epicondyle (16-18yo)
Trochlea (12-14yo)
Olecranon (15-17yo)
Lateral epicondyle (12-14yo)
Pneumonic: "Can't Resist My Team Of Lawyers"
Consider ordering films of both elbows to compare if in doubt.
How is this useful? If the trochlear center is present, but there is no medial epicondyle then you are most likely looking at a fx where the ossification center has been avulsed and displaced.
Identifying patients at risk of hypotension during intubation is not always straight forward. The prevalence of peri-intubation hypotension in the Emergency Department has been demonstrated to be approximately 20%.1 And while certain variables increase the likelihood of peri-intubation hypotension (ex. Shock index> 0.80), no single factor predicts it accurately enough to be used at the bedside.2 In the majority of patients undergoing intubation, clinicians should be prepared for peri-intubation hypotension with either vasopressor infusions or push dose pressors.
24-year-old male with a history of Wagner's Granulomatosis, currently on Cellcept (Mycophenolate Mofetil) and high dose prednisolone, presented with two days of sore throat, malaise and the lesions shown in the picture. What is the diagnosis?


{kind=link}