Magnetic resonance imaging (MRI) is the method of choice for imaging the spine for the suspicion of non-traumatic disorder, such as multiple sclerosis (MS), transverse myelitis, epidural abscess, spinal cord infarcts, and spondylotic myelopathy (changes in the spinal cord due to disk herniation or osteophytes in degenerative joint disease).
If the differential diagnosis includes infection, neoplasm, demyelination or inflammation, then IV contrast should be administered.
Recently Emergency Physicians have become far more aware of the importance of right ventricular (RV) function in our critically ill patient population. One of the methods that has been proposed to assess RV systolic function with bedside ultrasound (US) is the tricuspid annular plane systolic excursion (TAPSE). This simple bedside measurement utilizes M-mode to quantify the movement of the tricuspid annulus in systole. And while it has demonstrated reasonable accuracy at predicting RV dysfunction, adequate visualization of the lateral tricuspid annulus is not always obtainable in our critically ill patient population (1,2). In these circumstances an alternative measurement obtained in the subcostal window may be a viable option.
Similar to TAPSE, subcostal echocardiographic assessment of tricuspid annular kick (SEATAK) utilizes M-mode to assess the apical movement of the tricuspid annulus during systole. In a recent prospective observational study, Díaz-Gómez et al examined 45 ICU patients, 20 with known RV dysfunction and 25 with normal function. They compared the measurements obtained from TAPSE and SEATAK and found a strong correlation between the two measurement (Spearman’s ρ coefficient of .86, P=.03).
The small sample size and limited evaluation of RV function is far from ideal and more robust data sets are required before we cite SEATAK’s diagnostic accuracy with any confidence, but in the subset of patients where a TAPSE is unobtainable this may serve as an adequate surrogate until a more thorough echographic assessment can be obtained. 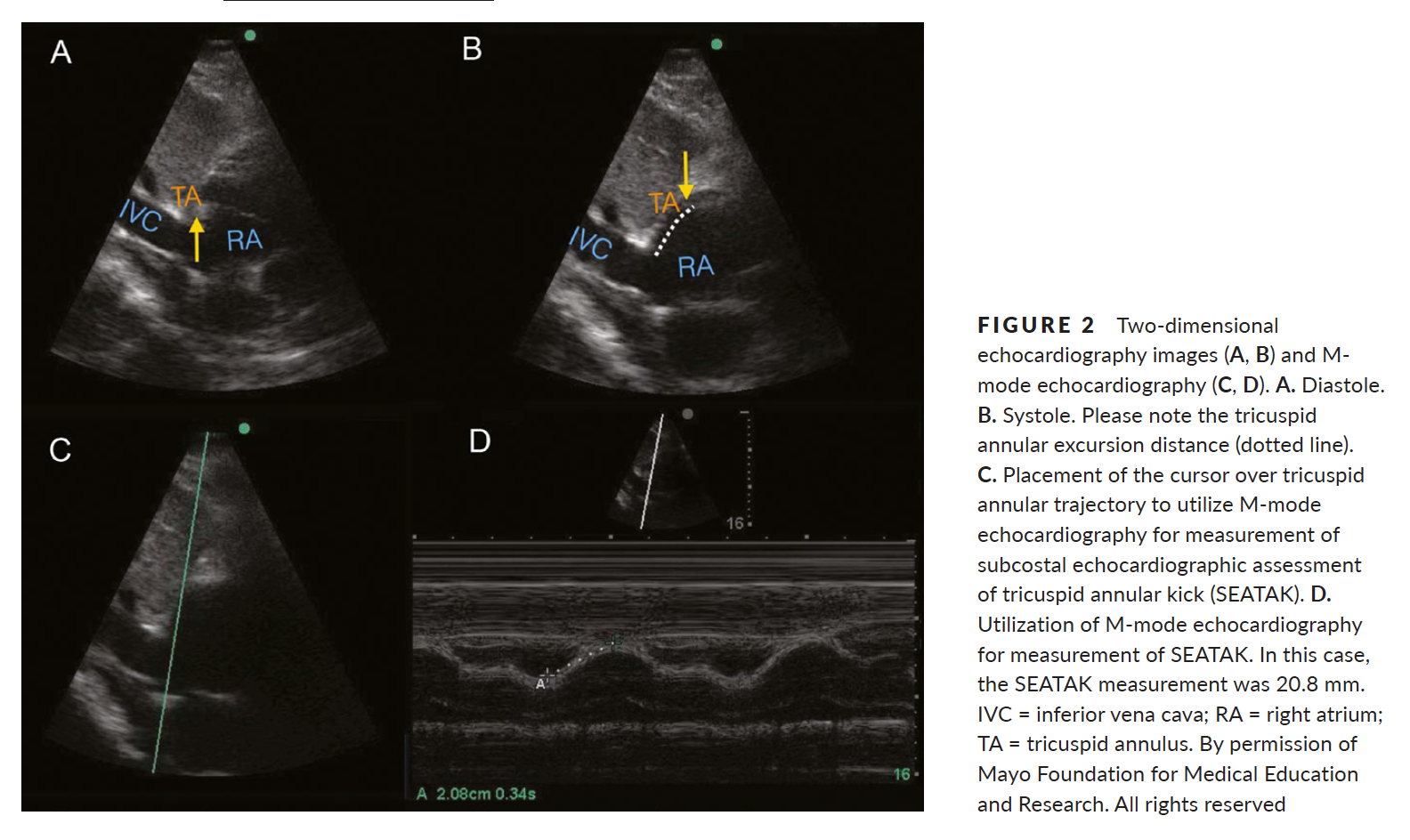
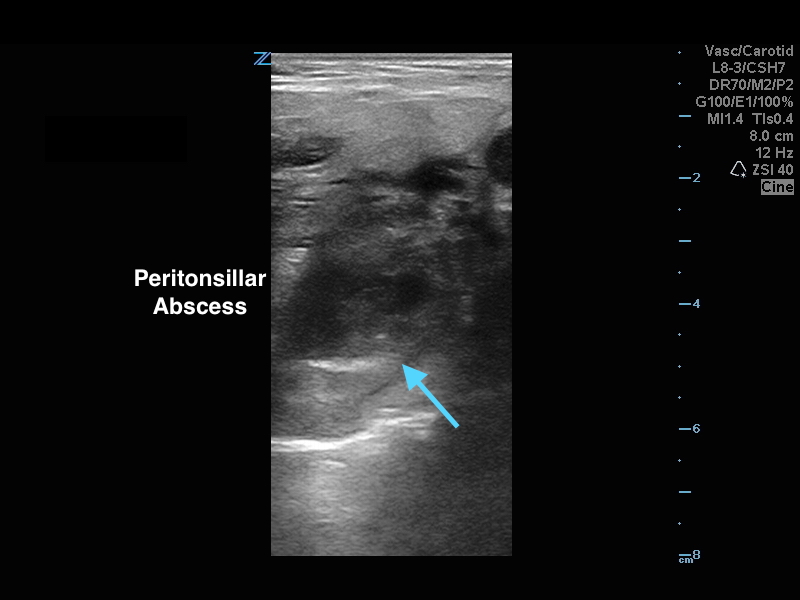
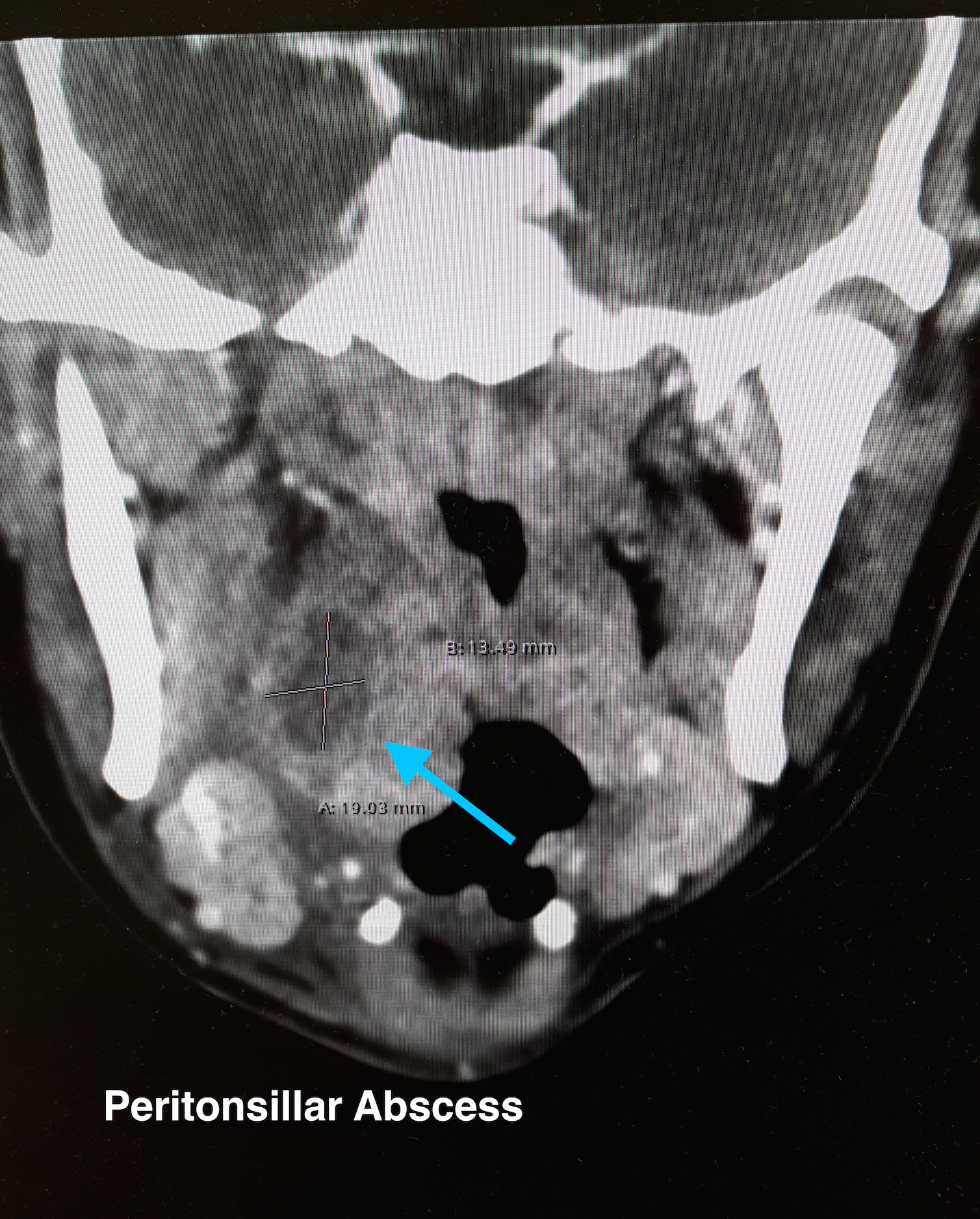
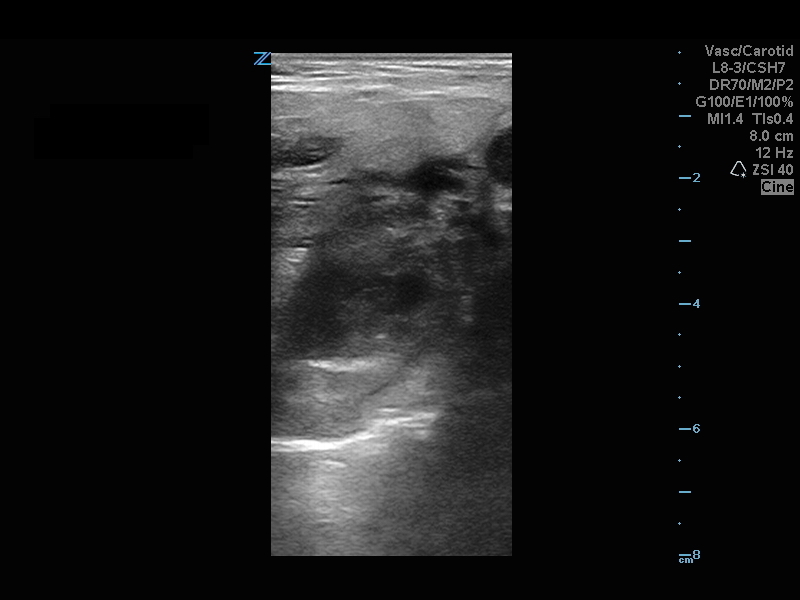
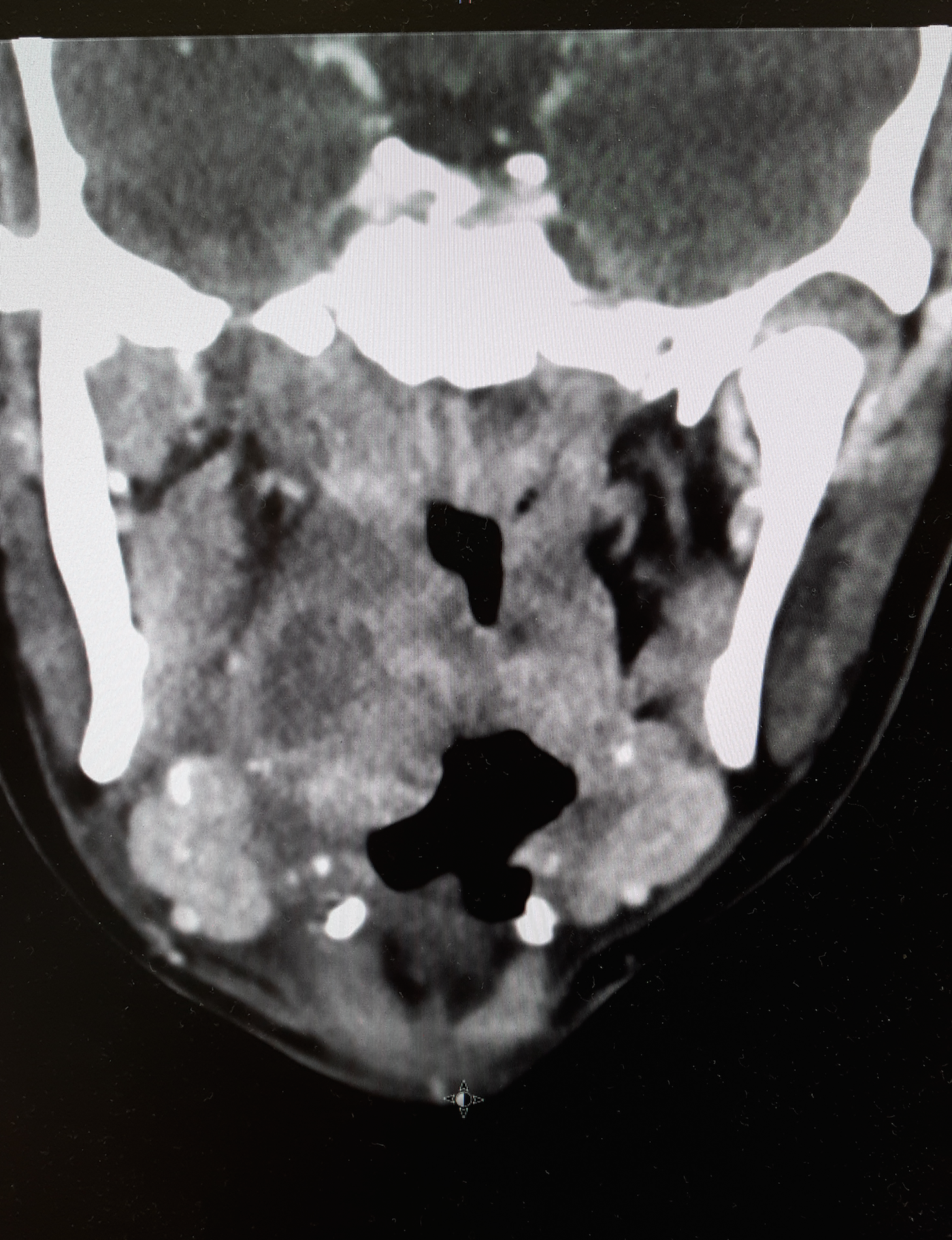
20 year-old female presents with sore throat, right throat fullness, difficulty speaking for 2-3 days. A bedside ultrasound and subsequent CT was obtained as seen below. What's the diagnosis?
Many of us use exercise as a coping strategy when emotionally stressed or to blow off steam when angry. This may place your heart at risk.
A recent observational study in Circulation surveyed 12,000 first MI patients about potential triggers. The associations didn't depend on age, smoking status, hypertension, or baseline physical activity.
Anger or emotional upset in the hour before onset elevated odds of MI 2.44 fold
A similar 2.31 fold elevation was observed form heavy exertion
However, the combination of the two raised the odds to 3.05 fold (P<0.001 for interaction)
Plasma-Lyte A outperformed 0.9% NaCl for rehydration in children with acute gastroenteritis showing a more rapid improvement in serum bicarbonate levels and dehydration scores.
--Massive PE is defined as PE with obstructive shock (hypotension [SBP <90] or end-organ malperfusion)
--Consider venoarterial (VA) ECMO in massive PE for hemodynamic support, particularly prior to intubation
--VA ECMO may prevent intubation/mechanical ventilation, surgical intervention, systemic and local thrombolysis
Davos Shoulder Reduction Technique
Take Home Points
Interested, well find out more by watching this video by Larry Mellick https://www.youtube.com/watch?v=u2MsnjVNoPM or clicking the link below.
US, Canadian and European critical care and toxicology societies recently published a consensus recommendation is the management of CCB poisoning.
Bottom line:
1. First line therapy remains unchanged: IV calcium, atropin, high-dose insulin (HIE) therapy, vasopressor support (norepinephrine and/or epinephrine).
2. Refractory to first line therapy: increase HIE, lipid-emulsion, transvenous pacemaker
3. Refractory shock, periarrest or cardiac arrest: Above (#1 & #2) plus ECMO if available.
Updated Guidelines for Traumatic Brain Injury
The Brain Trauma Foundation (BTF) Guidelines for the Management of Severe Traumatic Brian Injury (TBI) was recently updated and published in September 2016.
Updated recommendations include:
For the executive summary and complete guidelines, go to https://braintrauma.org/guidelines/guidelines-for-the-management-of-severe-tbi-4th-ed#/
Oxygen-ICU Trial
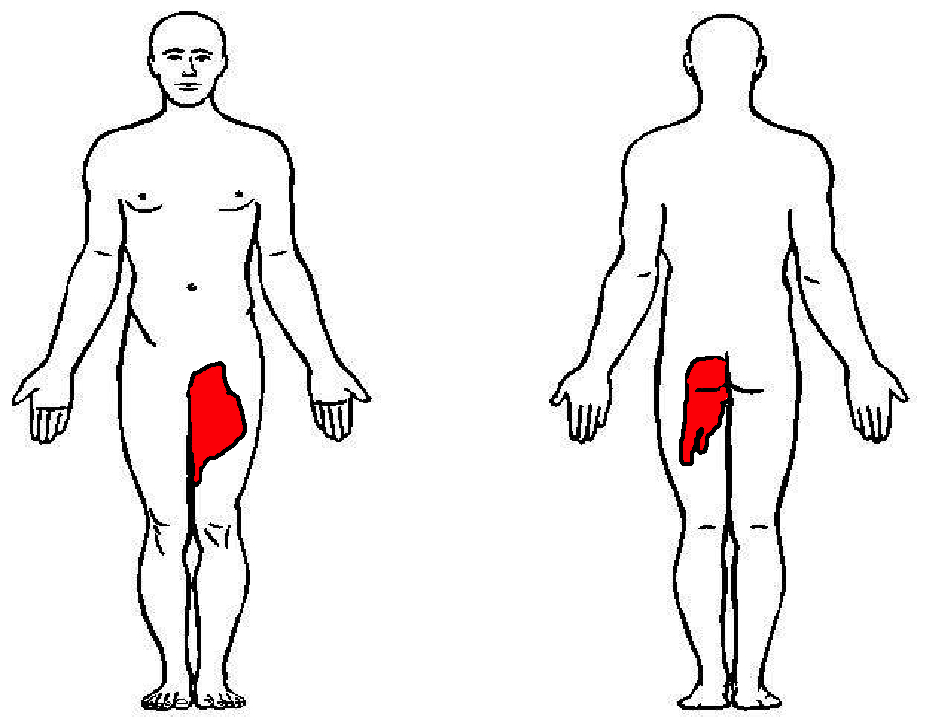
57 year-old female with history of bilateral lung transplants presents with fever, and 2 days of a painful, red, bumpy rash over the left labia and left buttock, but also notes a small tender area on the plantar surface of the left foot.
Below is a figure depicting the location of the rash, as well as a photo of her foot.
%20copy%201.JPG)
Recurrence depends on age and activity level
27% if >30yo and 72% if <23yo
Surgical Recommendations:
Large bony Bankart lesion, glenoid or humeral head defect >25%, recurrent instability, event near the end of season
Non surgical return to play:
If event occurs at beginning/early in season
Rehabilitation for 2 to 3 weeks (most return to play in this time frame)
Immobilization for 3 to 7 days in simple sling, gentle range of motion, cryotherapy
Physical therapy to strengthen dynamic stabilizers
Shoulder stabilization brace for non overhead throwing and contact sports
Fall clean up = Poison Ivy, oak, sumac (Toxicodendron species) which is ubiquitous in North America but it can also be found in British Columbia, Mexico and in parts of Asia. These plants are truly the scourge of outdoor enthusiasts and agricultural workers responsible for up to 40 million cases of miserable often temporarily incapacitating rashes annually.
Fast Facts:
Treatment Tips:
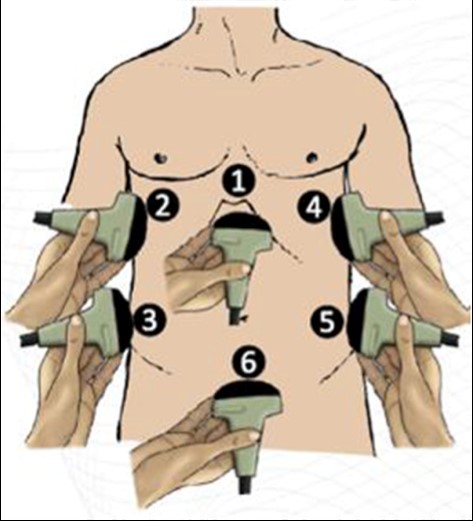
What is the FASH Exam?
Submitted by Dr. Laura Diegelmann
The delta gap is a measurement intended to assess for mixed acid-base disorders. A straightforward alternative, the strong ion difference (SID), allows for a quick and simple assessment of any non-gap acidosis or alkalosis that may be present.
The SID is simply the difference between the strong cations (Na+, K+, Mg+, Ca+) and the strong anions (Cl-) present in the serum. The abbreviated SID is the difference between the serum sodium and serum chloride levels (approximately 138-102). Values typically range from 36-40 mg/dl. Values less than 36 denote the presence of some degree of hyperchloremic, non-gap, acidosis. While values greater than 40 demonstrate the presence of hypochloremic, non-gap, alkalosis. And while on rare occasions, variations in albumin or elevated levels of cations other than sodium can lead you astray, the SID is as accurate as a delta gap at identifying mixed acid-based disorders without the added mathematical complexity.
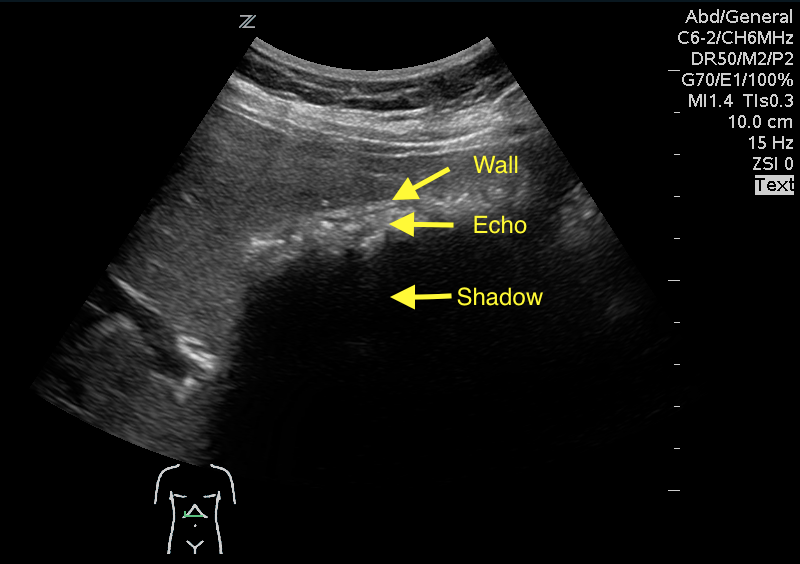
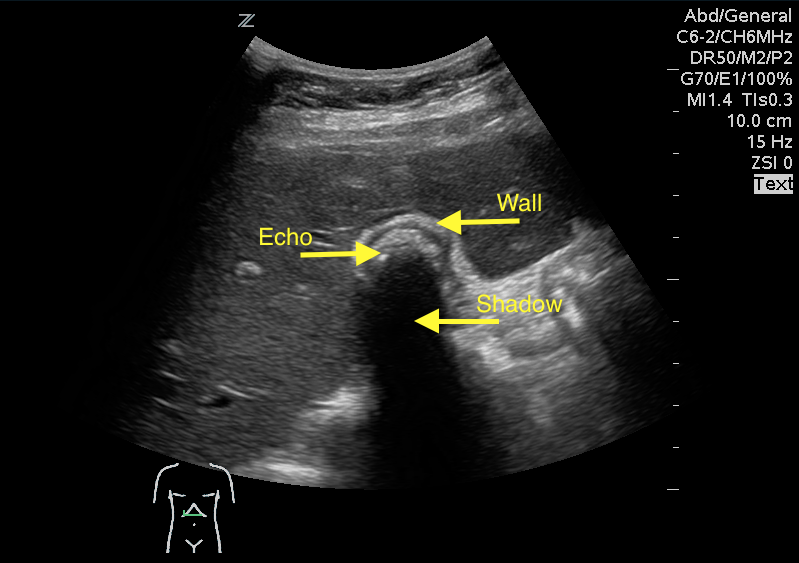
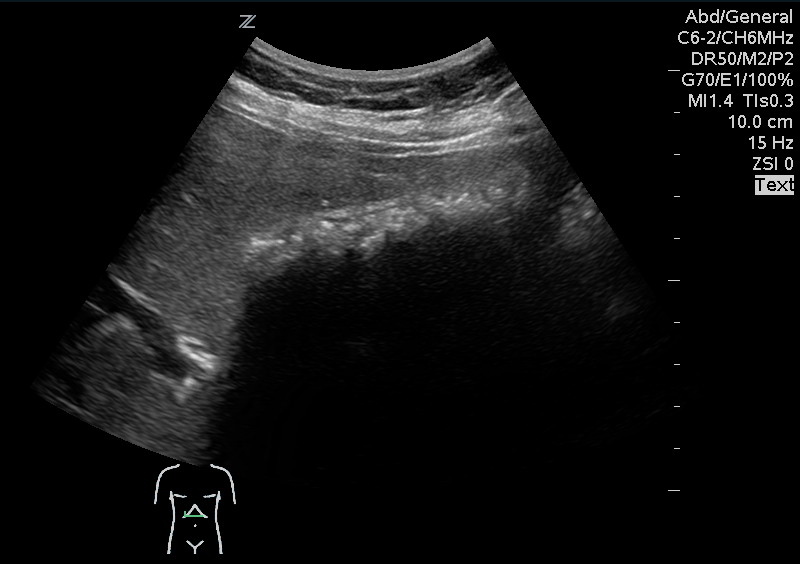
A 41 year old female presenting with intermittent RUQ abdominal pain for 1 week. An ultrasound of the right upper quadrant was performed. What is the diagnosis ?

What they did:
What they found:
Application to clinical practice:
A 12 year old male who recently started middle school presents to the ED with a rash in the periumbilical region that has been developing over the last few weeks. The rash is scaly, somewhat itchy, but otherwise benign appearing. The patient has no known medical conditions other than eczema, and is otherwise well. What is the diagnosis?
Picture courtesy of Mara Haseltine, MD

You have a patient in whom you suspect meningitis, but he is on warfarin for a history of pulmonary embolism. You started empirical antibiotics. His INR is 2.6, and you want to do a lumbar puncture (LP) to confirm your diagnosis. Can you use Prothrombin Complex Concentrate to lower his INR and safely perform the LP?
Take Home Point:
Using PCC to lower INR to enable LP is relatively safe and effective in patients on vitamin K antagonists. The dose used was individually determined by the physician according to initial INR.
Limitation:
This is a retrospective study, with no control group. One patient (2.7%) had a myocardial infarction that was “possibly related” to the PCC administration.
TAKE HOME POINTS:
-- High chloride load is associated with adverse outcomes in large-volume resuscitation (>60mL/kg in 24h), including increased risk of death [1]
-- Avoid supraphysiologic chloride solutions (i.e. normal saline) when resuscitation volumes are likely to exceed 60mL/kg (e.g. sepsis, DKA)