Acute cocaine toxicity can manifest with several cardiovascular issues such as tachycardia, dysrhythmia, hypertension, and coronary vasospasm. A new systematic review collated all of the available evidence for potential treatment options. Here is what the review found (there is also an 'other agents' section for medications with less published reports):
Benzodiazepines and other GABA-active agents: Benzodiazepines may not always effectively mitigate tachycardia, hypertension, and vasospasm from cocaine toxicity.
Calcium channel blockers: Calcium channel blockers may decrease hypertension and coronary vasospasm, but not necessarily tachycardia.
Nitric oxide-mediated vasodilators: Nitroglycerin may lead to severe hypotension and reflex tachycardia.
Alpha-adrenoceptor blocking drugs: Alpha-1 blockers may improve hypertension and vasospasm, but not tachycardia, although evidence is limited.
Alpha-2-adrenoceptor agonists: There were two high-quality studies and one case report detailing the successful use of dexmedetomidine.
Beta-blockers and alpha/beta-blockers: No adverse events were reported for use of combined alpha/beta-blockers such as labetalol and carvedilol, which were effective in attenuating both hypertension and tachycardia.
Antipsychotics: Antipsychotics may improve agitation and psychosis, but with inconsistent reduction in tachycardia and hypertension and risk of extrapyramidal adverse effects.
Sodium bicarbonate: Twelve case reports documented treatment of dysrhythmia with IV sodium bicarbonate, with seven reporting successful termination.
The authors note that "publication bias is a concern, and it is possible that successful treatment and/or adverse events have not been reported in some of the publications, and in general."
Sunset Eye Sign
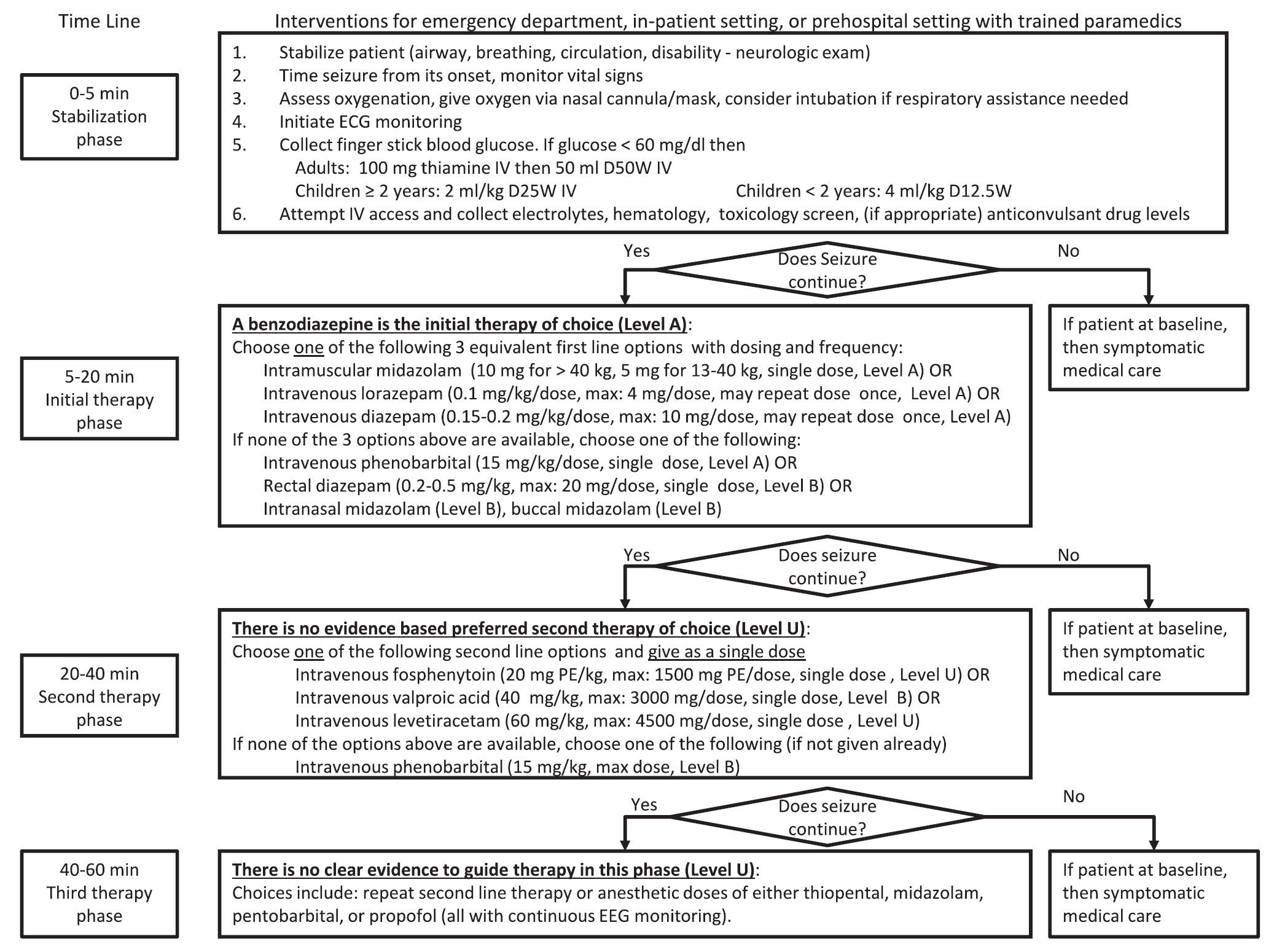
A new guideline for convulsive status epilepticus in adults AND children was recently published. [1] An insightful commentary was published alongside it (both are open access). [2] The proposed algorithm is below. Here are a few additional points to note:
Pure opioid agonists such as Morphine, Hydromorphone, and Fentanyl stimulate opioid receptors and are the most potent analgesics. Fentanyl and fentanyl analogues are up to 100 times more powerful than morphine and 30-50 times more powerful than heroin.
W-18 is a highly potent opioid agonist with a distinctive chemical structure which is not closely related to older established families of opioid drugs. While Fentanyl is approximately 100 times more powerful than Morphine, W-18 is about 100 times more powerful than Fentanyl.
While the flu season this year has been mild, it is still important to recognize which patients are at high risk for flu-related complications:
During the influenza season, when admitting a patient who 1) has respiratory symptoms and 2) is at high risk for influenza complications, consider testing them for influenza.
19 year-old male complaining of left arm pain one week after injecting anabolic steroids into his shoulder. What's the diagnosis?
Achilles tendon rupture
More common in
men, ages 30 - 40yo, s/p steroid injections, fluoroquinolone use, and episodic athletes "weekend warriors
Mechanism: usually during an athletic endeavor, sudden forced planar flexion or violent dorsiflexion of a plantar flexed foot
Location: Usually occurs 4 to 6 cm ABOVE the Achilles calcaneal insertion (hypovascular region)
Patient will report a sudden pop, gunshot like sound
History: Will report heel and calf pain and weakness/inability to walk
Physical examination: Palpable gap, weakness with plantar flexion, + Thompsons test
https://www.netterimages.com/images/vpv/000/000/007/7714-0550x0475.jpg
Consult orthopedics and splint in resting equinus
http://img.medscape.com/fullsize/migrated/408/535/mos0216.01.fig5b.jpg
Perianal Group A Strep is an infectious dermatitis seen in the perianal region that is caused by Group A beta-hemolytic Strep. Children will have a characteristic rash with a sharply-demarcated area of redness, swelling, and irritation around the perianal region. There may be associated swelling and irritation of the vulva and vagina (in girls) and penis in boys. Patients can have bleeding or itching during bowel movements.
The age range is often <10 years of age. There is often an absence of fever or other systemic symptoms.The diagnosis can be confirmed by obtaining a Rapid Strep swab from the area of interest. You can also collect a bacterial culture of the area.
Treatment requires a 14 day course of penicillin. Amoxicillin (40 mg/kg/day divided TID) and clarithromycin are alternative treatments. The additional of topical bactroban (mupirocin) can be effective, but it should not be used as monotherapy. Re-occurrence is common, so close follow-up is key.
Sepsis-3
Colchicine is an alkaloid compound found in Colchicum autumnale that is often mistaken by foragers as wild garlic (Allium ursinum). Unintentional ingestion wild garlic or therapeutic misadventures among elderly population with history of gout often result in unintentional toxicity.
It is a potent inhibitor of microtubule formation and function involved in cell division and intracellular transport mechanism. Thus toxicity is related to diffuse cellular dysfunction of all major organs and results in significant morbidity and mortality.
Colchicine toxicity occurs in three phases:
| Phase | Time | Signs and symptoms | Therapy |
| I | 0 – 24 hr | · Nausea, vomiting, diarrhea · Salt and water depletion · Leukocytosis | · Antiemetic · GI decontamination · IV fluids · Observation for leukopenia |
| II | 1 – 7 days | · Sudden cardiac death (24 – 48 hr) · Pancytopenia · Acute kidney injury · Sepsis · Acute respiratory distress syndrome · Electrolyte imbalance · Rhabdomyolysis | · Resuscitation · G-CSF · Hemodialysis · Antibiotics · Mechanical ventilation · Electrolyte repletion |
| III | >7 days | · Alopecia (2-3 weeks later) · Myopathy, neuropathy, myoneuropathy. |
|
Management
There is not much data published on susceptabilities of urinary pathogens in infants. What resistance patterns are seen in infants < 2 months in gram negative uropathogens?
A retrospective study of previously healthy infants diagnosed with urinary tract infections in Jerusalem over a 6 year period examined this question. The standard treatment at this hospital included ampicillin and gentamycin for less than 1 month olds and ampicillin or cefuroxime for 1-2 month olds.
306 UTIs were diagnosed
74% were resistant to ampicillin
22% were resistant to cefazolin and augmentin
8% were resistant to cefuroxime
7% were resistant to gentamycin
Of the organisms cultured, 76% were E. coli and 14% were Klebsiella.
Bottom line: Know your local resistance patterns.
What are the criteria for dengue hemorrhagic fever?
Spondylolysis
Prevalence 3-6% in the general population (Higher in athletes)
Location: L4 (5-15% of cases) & L5 (85-95% of cases)
Population: More likely in the skeletally immature athlete due to the vulnerability of the immature pars interarticularis to repeated stress
Symptoms: Lumbar pain worse with extension
Higher risk sports: Gymnastics, diving, weightlifting, wrestling
Treatment: Bracing and activity modification, physical therapy
- Good results in 80% with conservative management allowing return to play.
- Those who fail benefit from iliac crest bone grafting and posterolateral fusion.
-Return to play is controversial in this group
Please review th images below for anaomy and imaging appearence
http://orthoinfo.aaos.org/figures/A00053F01.jpg
http://www.sonsa.org/images/spondylolysis.jpg
http://www.physio-pedia.com/images/2/22/Spondylolysis_x_ray_.docx.jpg
Borrella mayonii a new species
There is a new bacteria that is causing Lyme disease. Borrella burgdorferi is the typical bacteria associated with lyme disease, but now several cases of Borrelia mayonii have been isolated from patients and ticks that live in Minnesota, Wisconsin and North Dakota. What is unique about this new species is that it is associated with nausea, vomiting, diffuse macular rashes, and neuro symptoms [e.g.: confusion, visual disturbance, and somnolence) along with the typical lyme disease symptoms of arthralgias and headaches.
Current lyme tests should detect this new species and treatment is the same as Borrella burgdorferi. The take home pearl is that we may see patients with "atypical" lyme disease symptoms so this should be on our differential for patients presenting with rashes, nausea, vomiting and neurologic complaints.
In September 2013, an international group representing major societies in toxicology and nutrition support began collaborating on a comprehensive review of lipid use in poisoning. Six total papers will be published, with the most recent two made available online this week. Here are the available (and forthcoming) papers:
Gosselin S, et al. Methodology for AACT evidence-based recommendations on the use of intravenous lipid emulsion therapy in poisoning. Clin Toxicol 2015;53(6):557-64. [PMID 26059735]
Grunbaum AM, et al. Review of the effect of intravenous lipid emulsion on laboratory analyses. Clin Toxicol 2016:54(2):92-102. [PMID 26623668]
Levine M, et al. Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity. Clin Toxicol. 2016;54(3):194-221. [PMID 26852931]
Hoegberg LC, et al. Systematic review of the effect of intravenous lipid emulsion therapy for local anesthetic toxicity. Clin Toxicol. 2016;54(3):167-93. [PMID 26853119]
Hayes BD, et al. Systematic Review of Clinical Adverse Events Reported After Acute Intravenous Lipid Emulsion Administration. Clin Toxicol. 2016 Apr 1. [Epub ahead of print] [PMID 27035513]
The final paper, which is in process, is the consensus recommendations from the workgroup based on the 4 systematic reviews.
Bottom Line: CT venography is good for diagnosing CVT, but MRI/MRV is superior for detection of isolated cortical venous thromboses and assessing parenchymal damage.
{kind=link}