A group from Colorado identified the high-stress of pediatric resuscitation as a high-risk setting for possible medication error. As such, they performed a prospective, block-randomized, crossover study with two mixed teams of docs (ABEM certified) and nurses, managing 2 simulated peds arrest scenarios using either:
1) conventional “draw-up and push” drug administration methods [control] or
2) prefilled medication syringes labeled with color-coded volumes correlating to the weight-based Broselow Tape dosing [intervention].
The objective was to compare the time of preparation and administration of a medication, as well as to assess dosing errors. Participants were blinded to the purpose during recruitment but unblinded just prior to running the scenarios.
The scenarios included advanced airway management and hemodynamic life support efforts to care for an 8-year-old or 8-month-old manikin. The intervention group received a standard 3-minute tutorial on the use of prefilled color-coded syringes just prior to their scenario. After completing the first scenario, the groups switched, utilizing the other sim with the other method of medication administration. After a 4-16 week “wash out” period, the groups reconvened to reverse the medication administration technique across the same 2 scenarios.
Each Broselow tape color zone corresponds to a narrow range of weights. The authors opted to designate medication dosing errors >10% above or below the correct range as critical dosing errors.
The results? Median time to delivery of all conventionally administered medication doses was 47 seconds versus the prefilled color-coded administration system-- 19 seconds. The conventional administration system saw 17% of doses with critical errors versus none for the prefilled color-coded syringe group.
These prefilled color-coded syringes are not currently manufactured. Should they go into commercial production, the hope is that such syringes would be longer and more narrow than conventional syringes to effectively elongate each color-coded section (the delineations for red and purple on a standard syringe differ by as little as 1/8-3/32 of an inch if you want to make your own!-- see picture).
If you are interested in learning about the current status of emergency medicine in a specific country, it can be difficult to find up-to-date information. One excellent resource for country specific details is the American College of Emergency Physicians’ (ACEP) International Ambassador Program.
This program has Emergency Medicine Ambassadors (U.S. emergency physicians), Liaisons (in-country emergency physicians) and Representatives (U.S. emergency physicians in training) for many countries around the world. Additionally, there are country specific reports that give annually updated information about emergency medicine in each country.
Included on the website are links to send emails to the Ambassadors, Liaisons and Representatives in order to request more detailed information.
To learn more, see: http://www.acep.org/IntlAmbassador/
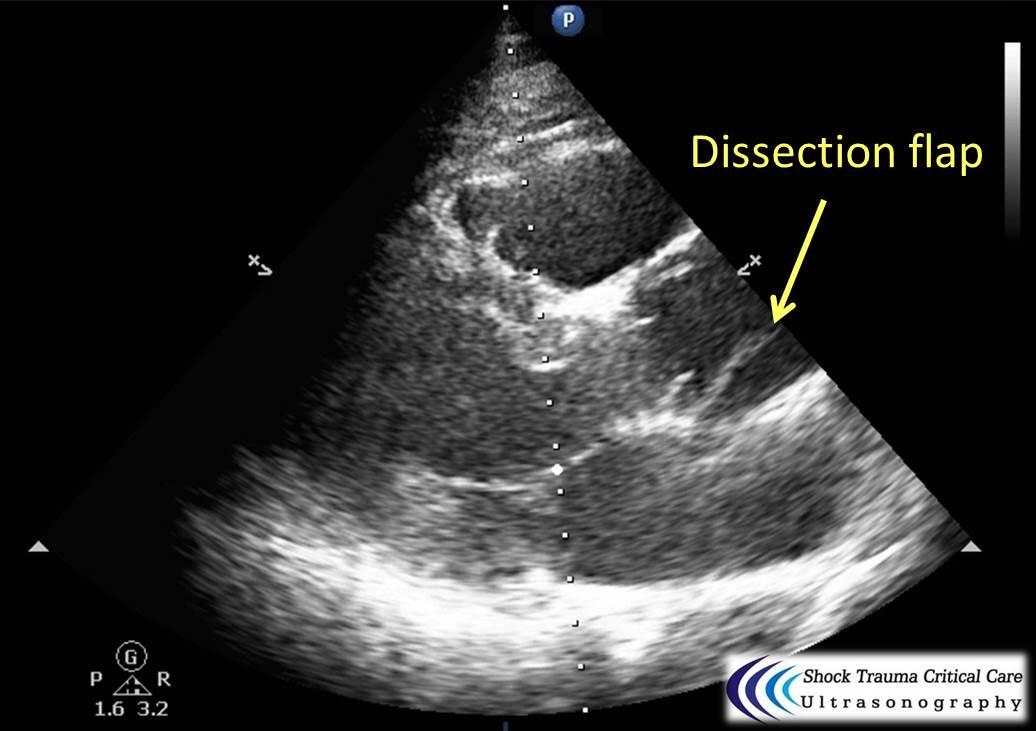
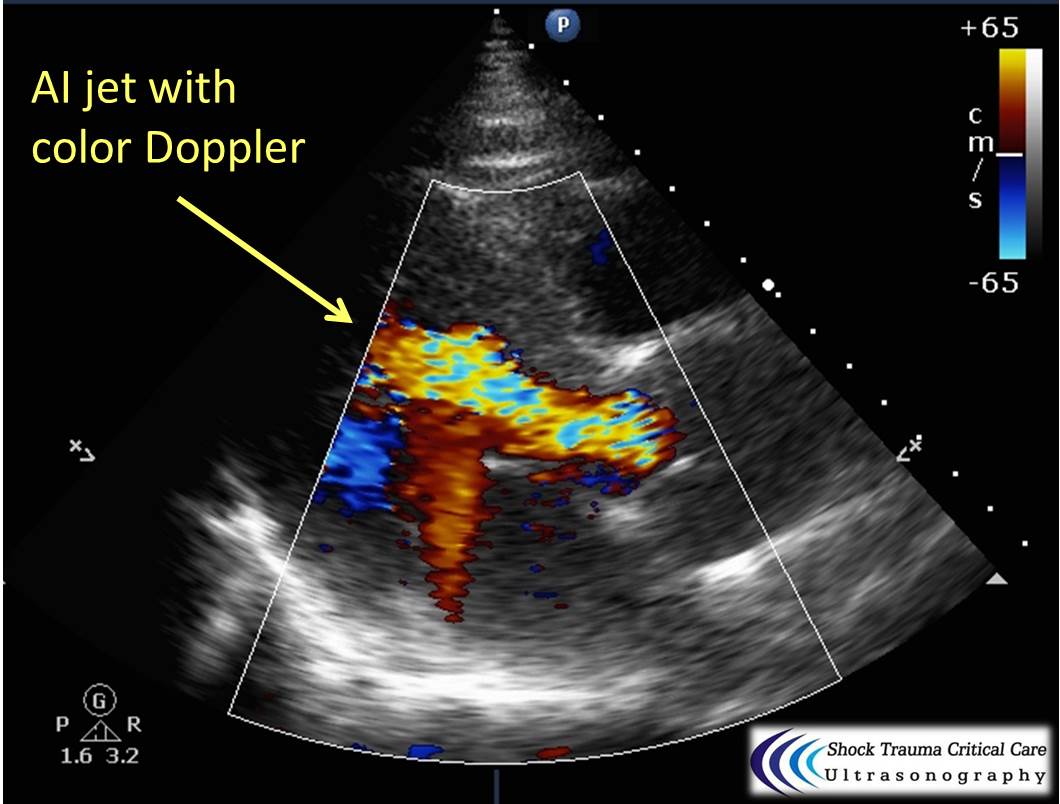
Classically, aortic dissection presents as tearing or ripping chest pain that radiates to the back in a HYPERtensive patient.
However, type A aortic dissections can quickly become HYPOtensive due to any the primary cardiac complications from retrograde dissection into:
Bedside echo can't rule out aortic dissection, but it can help rule in the diagnosis (figure 1) or complications (figure 2) at times.
26 year-old male presents with a swollen 4th digit and pain during extension, what’s the diagnosis?

Most common mass in popliteal fossa
Incidence 10 to 58%
Intra-articular pathology results in flow of synovial fluid from the joint into the bursa, forming a cyst
Association with concomitant intra-articular disorders 94%
Possible pathology - Meniscus, ligamentous, arthritis, other osteochondral defects
In children this is not a pathologic finding
Symptoms - Posterior knee bulging, posterior tightness/stiffness esp. with knee flexion
Ultrasound - 100% sensitive/specific
DDx: DVT
Tx: Refer for ultrasound guided aspiration, fenestration and steroid injection
http://www.caringmedical.com/wp-content/uploads/2013/11/Bakers-Cyst-treatment.jpg
A thunderclap headache is defined as a very severe headache that reaches its maximum intensity within 1 minute.
One of the most common causes (and the one associated with this buzzword on board questions!) is subarachnoid hemorrhage, but what else can cause a it?
- Reversible cerebral vasoconstriction syndrome (RCVS): suggested by recurrent thunderclap headaches (2-10) over 1 to 2 weeks. Normal CT and LP, with vasoconstriction on angiography. Can lead to SAH, ICH or ischemic stroke.
- Cervical artery dissection
- Cerebral venous sinus thrombosis
- Spontaneous intracranial hypotension: characterized by orthostatic HAs and auditory muffling.
- Intracerebral hemorrhage
- “Primary”: a diagnosis of exclusion
Bottom line? All patients with thunderclap HA should have a stat head CT with no contrast, then have SAH excluded with an LP, CTA or MRI/MRA. Just because you excluded SAH in a patient with thunderclap headache does not mean you’re done with the emergency workup.

30 year-old male with abdominal pain and diffuse tenderness on exam. Ultrasound is shown, what's the diagnosis?
Shoulder Dislocation Reduction
Do you have a chronic dislocated that frequents your ED? Are you interested in teaching them a way to relocate their shoulder without looking like Mel Gibson from Lethal Weapon, https://youtu.be/Igrdi_lhhW4, then the newly described GONAIS method might be what you are looking for.
This technique has the patient grab the top of a chair with the hand on the affected side, and then slowly equating, effectively bringing the hand and arm above their head. Once in the full squat position the patient can step backwards which should reduce the shoulder. If not they can use the opposite hand to apply pressure to push the humerus backward and reduce the location.
The full article can be found at http://bit.ly/1iZ8a9z
Is there a set of criteria similar to the Ottawa Ankle or Knee Rule that can be applied to the wrist in children?
The Amsterdam Pediatric Wrist Rules are as follows:
-Swelling of distal radius
-Visible deformity
-Painful palpation of the distal radius
-Painful palpation at the anatomical snuff box
-Painful supination
A positive answer to any of these would indicate the need for an xray.
The study referenced attempted to validate these criteria. This criteria is inclusive of the distal radius in addition to the wrist. The sensitivity and specificity were 95.9% and 37.3%, respectively in children 3 years through 18 years. This model would have resulted in a 22% absolute reduction in xrays. In a validation study, 7/170 fractures (4.1%, 95% CI: 1.7- 8.3%) would have been missed using the decision model. The fractures that were missed were all in boys ages 10-15 and were all buckle fractures and one non displaced radial fracture.
Bottom line: This rule can serve as a guide for when to obtain an xray in the setting of trauma, but it is not perfect.
Monosodium glutamate
Metabisulfites (Na sulfite, Na/K bisfulfite, Na/K metabisulfite, etc.)
Tyramine reaction
Niacin
Trichloroethylene
Scrombroids
Hydroxocobalamin
Which infectious disease listed as Class A agents occur naturally, though sporadically within the U.S?
Small pox no longer occurs naturally and other viral hemorrhagic fevers occur in tropical settings.
SIMV (Synchronized intermittent mandatory ventilation)
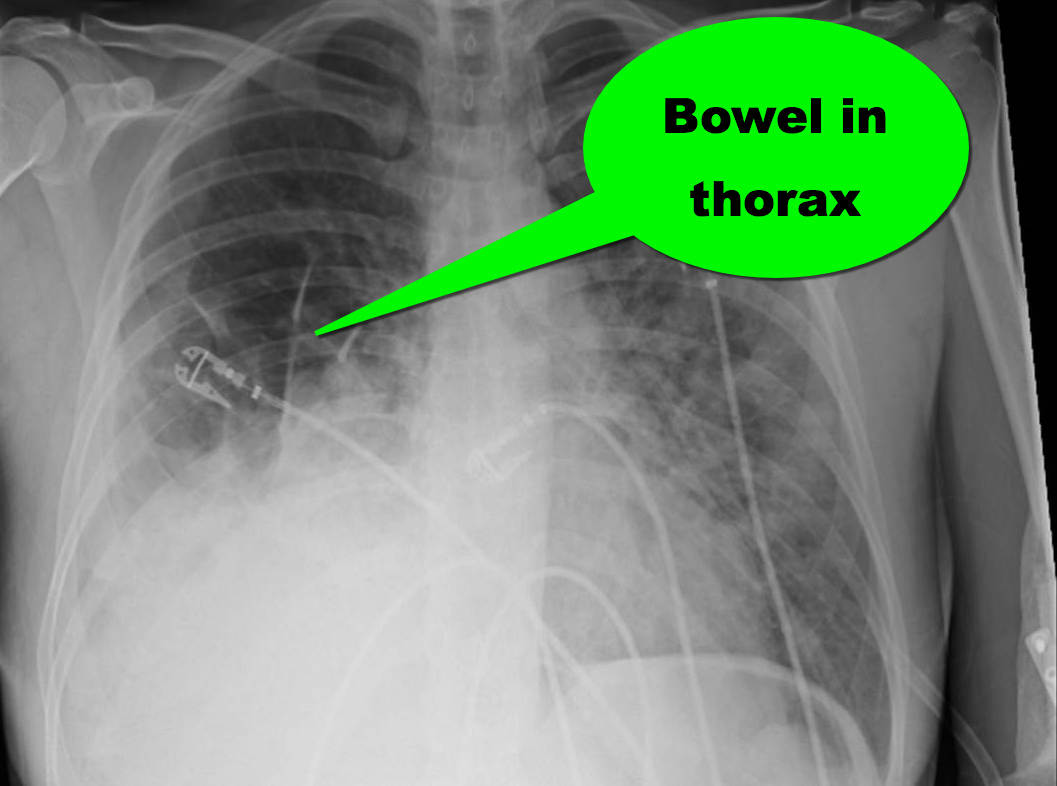
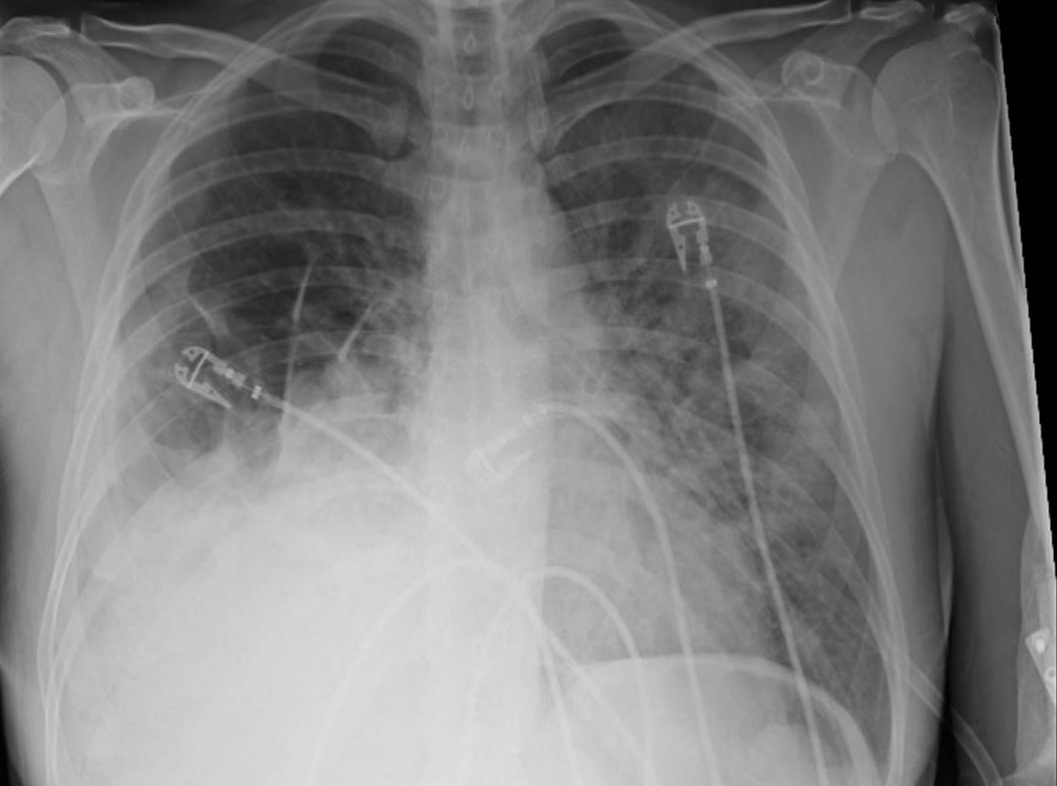
35 year-old female presents to the Emergency Room with cough and chest tightness. She was discharged from the hospital yesterday for an asthma exacerbation that was secondary to pneumonia. What's the diagnosis?
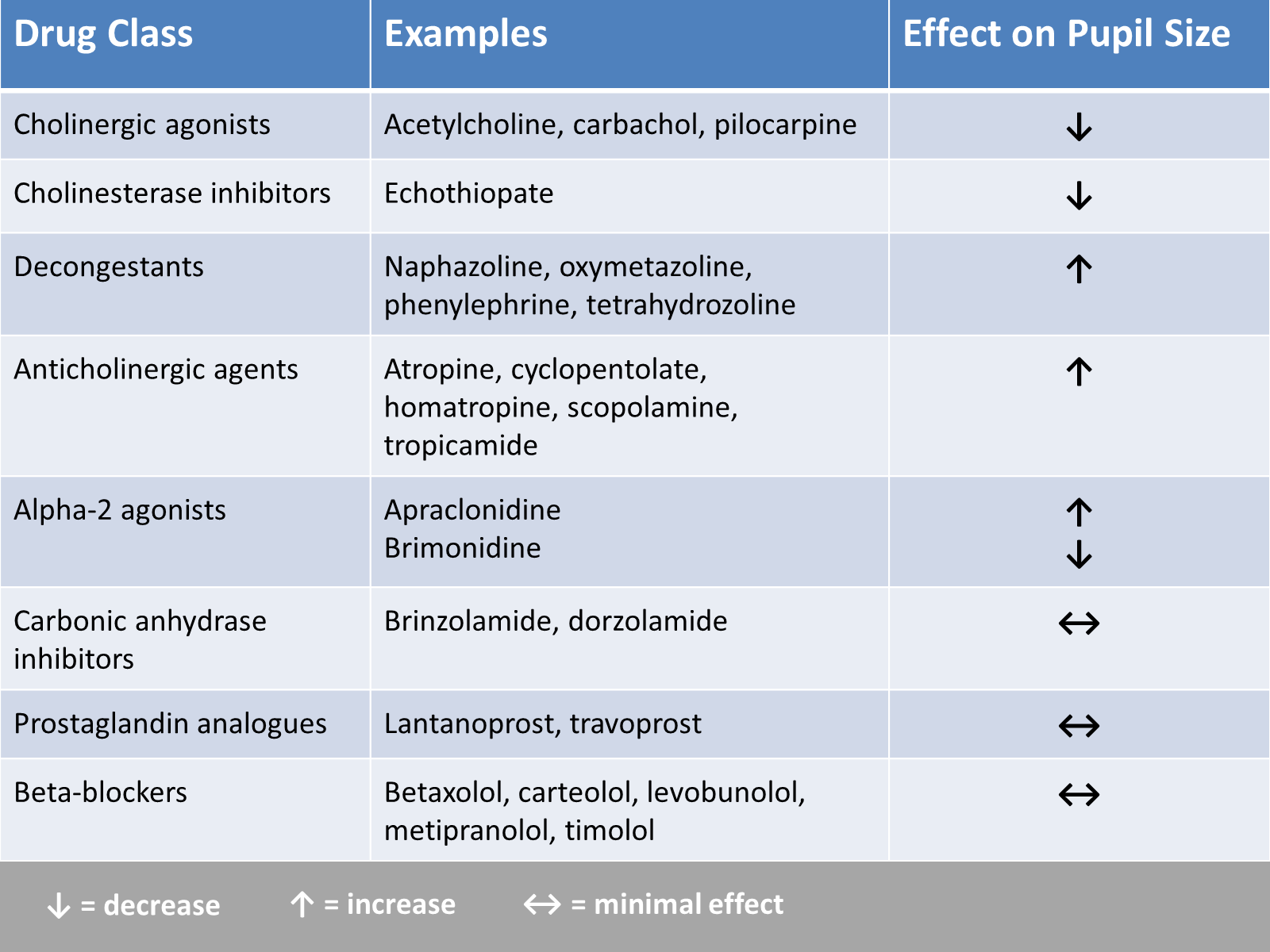
In the evaluation of ED patients, it may be important to understand the effect on pupil size from the ophthalmic medications they use. Here is a summary chart of common eye drops and their effect on pupil size.
Serotonin Syndrome - What is It?
** Stay tuned for part 2 on what causes serotonin syndrome **
Hyperoxia in the Critically Ill
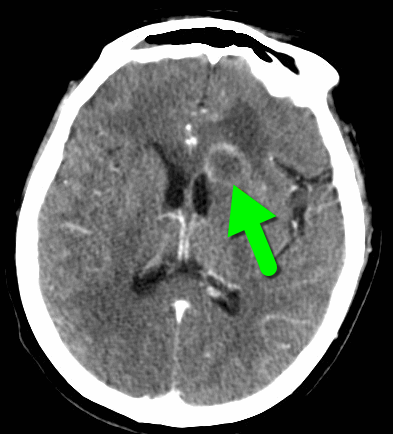
68 year-old man presents with a new-onset seizure. What's the diagnosis and what's in your differential diagnosis?
A new prospective, randomized, double-blind trial compared subdissociative ketamine to morphine for acute pain in the ED.
What they did
What they found