Are We Using the Glasgow Coma Scale Reliably?
| Reported by Responders | |
| Patient population in which GCS is used | Traumatic brain injury (96%) Other neurological disorders (78%) |
| Intended purpose of GCS | Classification of severity of injury (51%) Serial evaluation of patient over time (33%) Clinical decision making (44%) Prognostication (17%) |
| Application of stimulus | Both arms and legs (62%) Only arms (37%) |
| Type of stimuli used | Nail bed pressure (57%) Lateral side of finger (22%) Supra-orbital nerve pressure (52%) Trapezius or pectoralis pinch (50%) Sternal rub (53%) Retromandibular stimulation (24%) Earlobe stimulation (16%) |
| Reporting of GCS | Description in words, e.g. no eye opening, no motor (19%) Numerical report, e.g. E1V1M1 (46%) Sum score, e.g. EVM=3 (35%) |
Bottom line: There are variations in the application, assessment, and reporting of the GCS. A standardized approach is needed for it to be a reliable assessment and communication tool.
There is little debate that ultrasound-guided central lines are safer, faster, and more reliable compared to a landmark technique; there is some debate, however, as to whether the short axis (SA) or long axis (LA) approach is the best (see clips below).
The referenced study compared the SA and the LA technique for both the internal jugular (IJ) and subclavian (SC) venous approach. The authors measured number of skin breaks, number of needle redirections, and time to cannulation for each method.
This study demonstrated that the LA technique for subclavian placement had fewer redirections, decreased cannulation time, and fewer posterior wall punctures as compared to the SA. With respect to the IJ approach, the LA was also associated with fewer redirections than the SA view.
Bottom line: Consider the long-axis technique the next time you place an ultrasound guided central line.
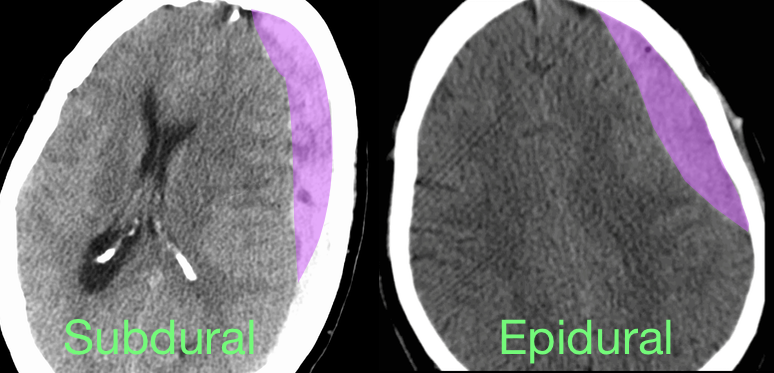
40 year-old male sustains a blunt force injury the left side of his lead. What's the diagnosis and what structure was injured?
Ischemic ECG Findings: Significance of the U-wave
The U-wave is a small deflection immediately following the T-wave, commonly with the same polarity as the T-wave and most prominently seen in precordial leads V2–V3.
Prominent U-waves are most often seen with bradycardia and hypokalemia, but can also be secondary to other electrolyte imbalances and medications.
Typically, T- and U-wave polarities are concordant; discordant U-waves have been identified several hours prior to other ECG changes in acute myocardial infarction.
Some studies note that exercise induced U-wave inversion is highly predictive of CAD; negative U -waves in the precordial leads during exercise had a higher specificity (88% vs. 70%) & positive predictive value (77% vs. 61%) for ischemia than ST-depression.
Reinig et al. 2005 showed that negative concordance of T- and U-waves have poor prognosis & is quite specific for ischemia.
· ECG’s were divided into 3 groups:
o Type 1 T-U discordance (negative T waves + positive U waves)
o Type 2 T-U discordance (positive T waves + negative U waves)
o Negative T-U concordance (both T & U waves negative)
* Significantly higher rate of CAD (88% vs. 58%) (P-value <. 0001) in the negative T-U concordance group
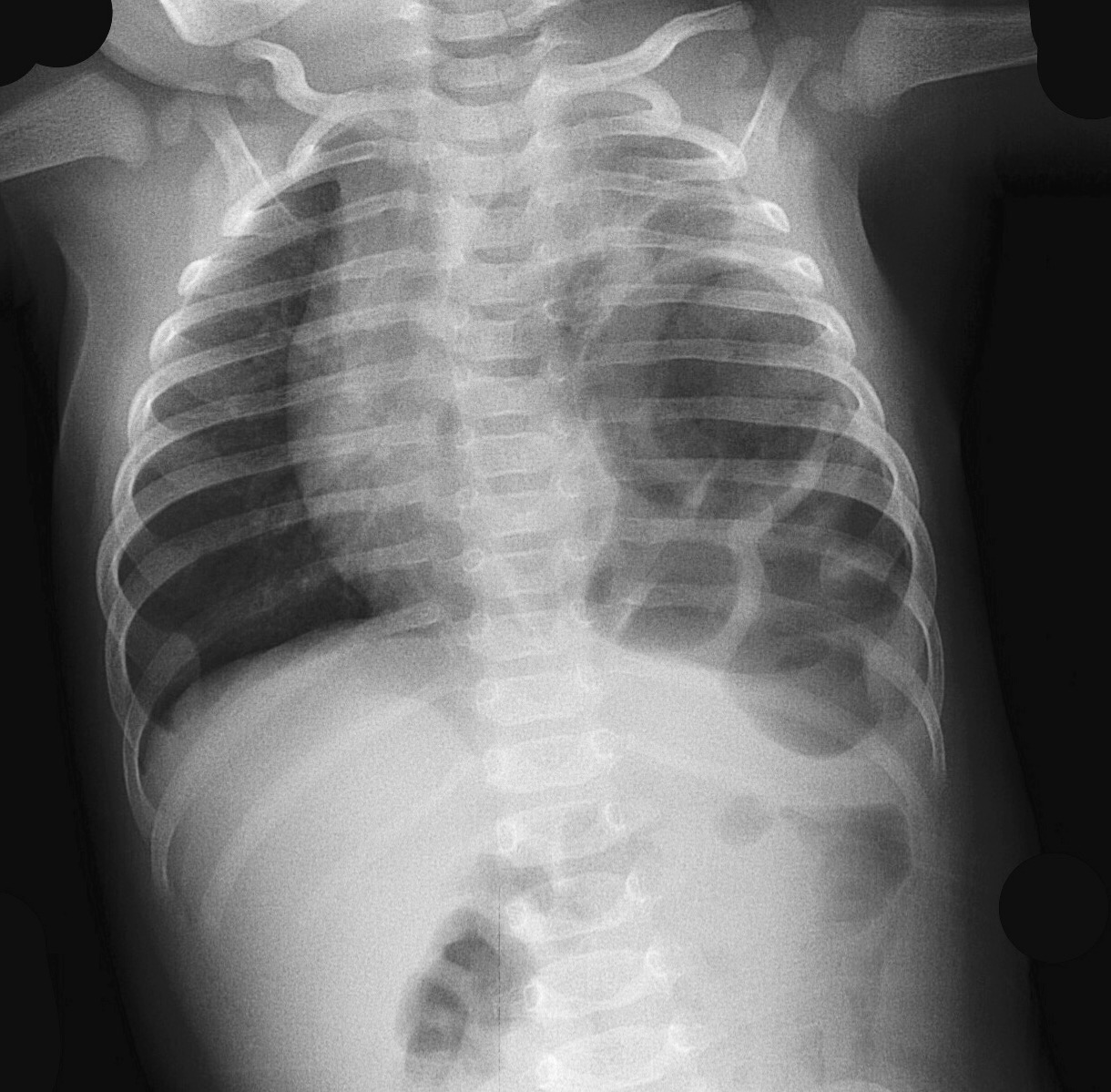
Posterior Shoulder Dislocations are uncommon (strong supporting structures vs. anterior)
But commonly missed by physicians
Mechanism: Direct blow anterior shoulder/FOOSH with shoulder internally rotated and ADDucted)
May also see with seizure/electric shock (tetanic contraction)
Clinical findings subtle
Shoulder held in ADDuction and internal rotation. Patient unable to externally rotate arm from this position. If habitus allows, anterior shoulder depression/posterior fullness.
Radiology: Decreased overlap between humeral head and glenoid fossa. Proximal humerus fixed in internal rotation looks like a light bulb on a stick.
Y view will show subtle posterior displacement of humeral head (not as dramatic as is in anterior dislocations!)
http://cdn.lifeinthefastlane.com/wp-content/uploads/2009/06/posterior_shoulder_dislocation_005.jpg
http://eorif.com/Shoulderarm/Images/Shoulder-dislocationP1.jpg
In addition to the down regulation of GABA receptors in chronic ethanol users, there is an upregulation in NMDA receptor subtypes. Although the pathophysiology is much more complex, when ethanol abstinence occurs, there is a shortage of GABA-mediated CNS inhibition and a surplus of glutamate-mediated CNS excitation. If GABA agonists are the mainstay of treatment, why not also target the NMDA receptor? Enter ketamine.
Only one study exists and was published recently.
While the dexmedetomidine studies should not be using reduction in benzodiazepine requirements as an endpoint, it may be acceptable for ketamine since it actually works on the underlying pathophysiology. More studies are needed but it's good to see we’re starting to look at it.
Introduction:
There were approximately 56 million deaths worldwide in 2012. The causes of death vary significantly based upon the income level of the country.
High-income Countries:
Low-income Countries:
Bottom Line:
Acute care services in the US and high-income countries need to acknowledge the growing number of individuals with chronic diseases and the rapidly growing elderly population. In low-income countries, acute care services still need to primarily address maternal/child infections and problems as well as infectious diseases.
Safety of Thoracentesis
Results after 24 hours of followup post-procedure
Other interesting points:
Bottom line: Use your ultrasound to direct your tap and dont take out more than 1500 mL routinely
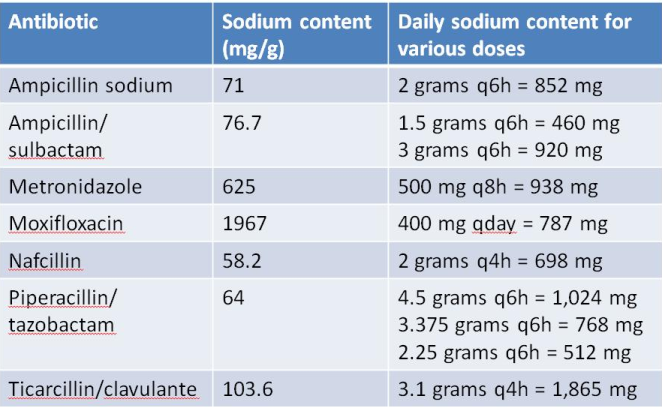
Aside from sodium chloride and sodium bicarbonate, several commonly used emergency department medications (namely IV antibiotics) contain a significant amount of sodium. In patients with heart failure or other conditions requiring sodium restriction, judicious use should be considered.
Notes:
There are some studies that have shown that NSTEMI patients have done worse when administered opioids. Most studies were not well controled and the exact mechanism was not clear. This study adds a biological mechanism to these fidnings.
Hobl et al. showed clopidogre concentrations delayt peak yhours, have overall decrease AUC and actually decrease active metabolites when morphine is administered IV. Morphine may not be the right choice in any ACS that receives clopidogrel.
A Lancet Commission on Global Surgery has just published a 56 page article about the need to improve access to surgery and anesthesia care. Its five key messages are:
The need for high quality acute care, both for urgencies and emergencies, is clearly an important component of providing “universal access to safe, affordable surgical and anaesthesia care”- the vision of the Commission.
SIRS and Severe Sepsis Screening
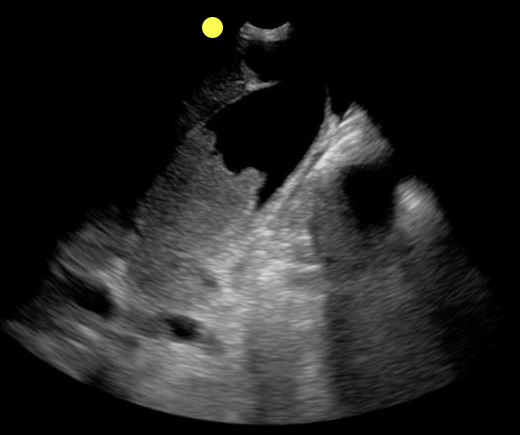
70 year-old female presents from a nursing home with fever and abdominal pain. A right upper quadrant ultrasound is shown, what's the diagnosis?
In cases of suspected spinal infection, the sensitivity of an elevated WBC count (35-61%), ESR (76-95%) and CRP (82-98%) may help guide further evaluation or consideration of other entities.
Incorporation of ESR/CRP into an ED decision guideline may help differentiate those patients in whom MRI may be performed on a nonemergent basis.
An elevated ESR (>20 mm/hour) also has a role in the diagnostic evaluation of occult malignancy (sensitivity 78%, specificity 67%).
Some medical issues arise in patients with brain tumors:
// Steroids are used to decrease vasogenic edema, especially preop or during radiation therapy. Patients are ideally gradually weaned off steroids. Dexamethasone is most commonly used. 1-2% of patients are at risk for adrenal suppression.
// Infections: Post-op wound infections can be delayed up to months, especially in patients on steroids.
// Antiepileptics: Although technically not recommended in patients with brain tumors who have not had seizures (American Academy of Neurology 2010), many surgeons continue to prescribe antiepileptics preoperatively and then discontinue them by 1 month postop if the patients remain seizure-free. Levetiracetam is emerging as the drug of choice due to favorable side effect profile.
// Thromboembolism: Brain tumors are considered very high risk for venous thromboembolism. Low-molecular-weight heparin is the treatment of choice, with warfarin being an acceptable substitute.
// Arterial thrombosis and ischemic stroke: Risk is increased with certain medications, and thrombolysis is contraindicated.
Updates in the Management of Large Hemispheric Infarction
Large hemispheric infarctions (LHI) are estimated to occur in 2-8% of all hospitalized ischemic strokes and 10 15% of all MCA territory infarcts. LHI carry high rates of morbidity and mortality, in fact, if left untreated associated cerebral edema can rapidly progress to transtentorial herniation and death in 40 80% of patients.
Recognized risk factors for progressive cerebral edema include:
Evidence based medical strategies for LHI include:
Prophylactic hemicraniectomy
Bottom Line: Early recognition of large hemispheric stroke is critical as it is associated with a high rate of morbidity and mortality. Aggressive medical management and early neurosurgical involvement may improve outcomes.
References
Follow me on Twitter @JohnGreenwoodMD
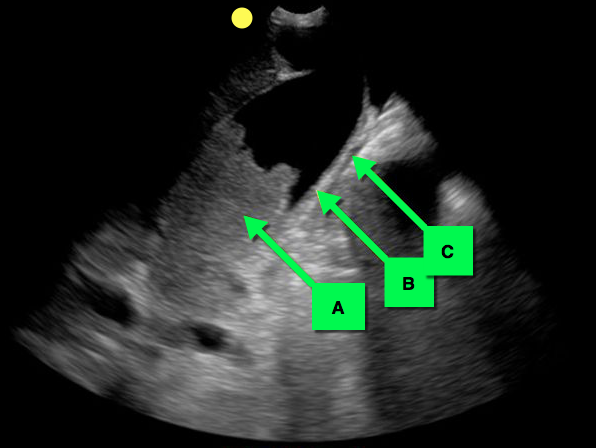
You see the following on a parasternal long-axis view; what's the diagnosis and what coronary distribution is involved?
Cardiac Sarcoidosis
- Cardiac Sarcoidosis (CS) is reported to involve ~2-5% of patients with systemic sarcoidosis. An increasing proportion of patients are presenting with isolated CS.
- Isolated CS is associated with a higher female predominance; severe LV involvement, heart failure, and poor prognosis.
- Manifestations range from symptomatic conduction disturbances, dysrhythmias, progressive heart failure, and silent myocardial granulomas - leading to sudden cardiac death.
- CS is a serious condition with a quoted 5-year survival ~60-75%.
- Corticosteroid therapy is considered cornerstone in management, but evidence is largely observational and no randomized trials have been performed to date.
Is acetaminophen good for pain control in patients with Osteoarthritic of the Knee or Hip or Low Back Pain? Most of my patients request narcotics, but conventional teaching is that we should try to start with Acetaminophen or NSAIDs.
This recent study, http://www.bmj.com/content/350/bmj.h1225, published in the BMJ analyzed 13 studies looking at over 5400 patients. In the end, they found that acetaminophen did not appear to improve pain, disability or the patient’s quality of life in patients with back pain. Also, there was a small improvement in pain and disability in those with hip and knee pain, but it was not deemed clinically significant.
Even worse, patients taking acetaminophen had a 4x greater chance of having abnormal liver function tests.
This meta-analysis really questions whether Acetaminophen should be first line therapy in patients with osteoarthritis of the knees or hips, or in those with low back pain. For now I will stick with a course of a NSAID. Especially with the risk of unintentional overdose if they are taking other over the counter medicaitons that might also contain acetaminophen.