Sickle Cell Disease (SCD) is a hemoglobinopathy that is considered a relatively rare disease in the United States, affecting about 90,000-100,000 individuals.
Globally, SCD affects millions, primarily in West and Central Africa.
Acute presentations of SCD include:
The bottom line:
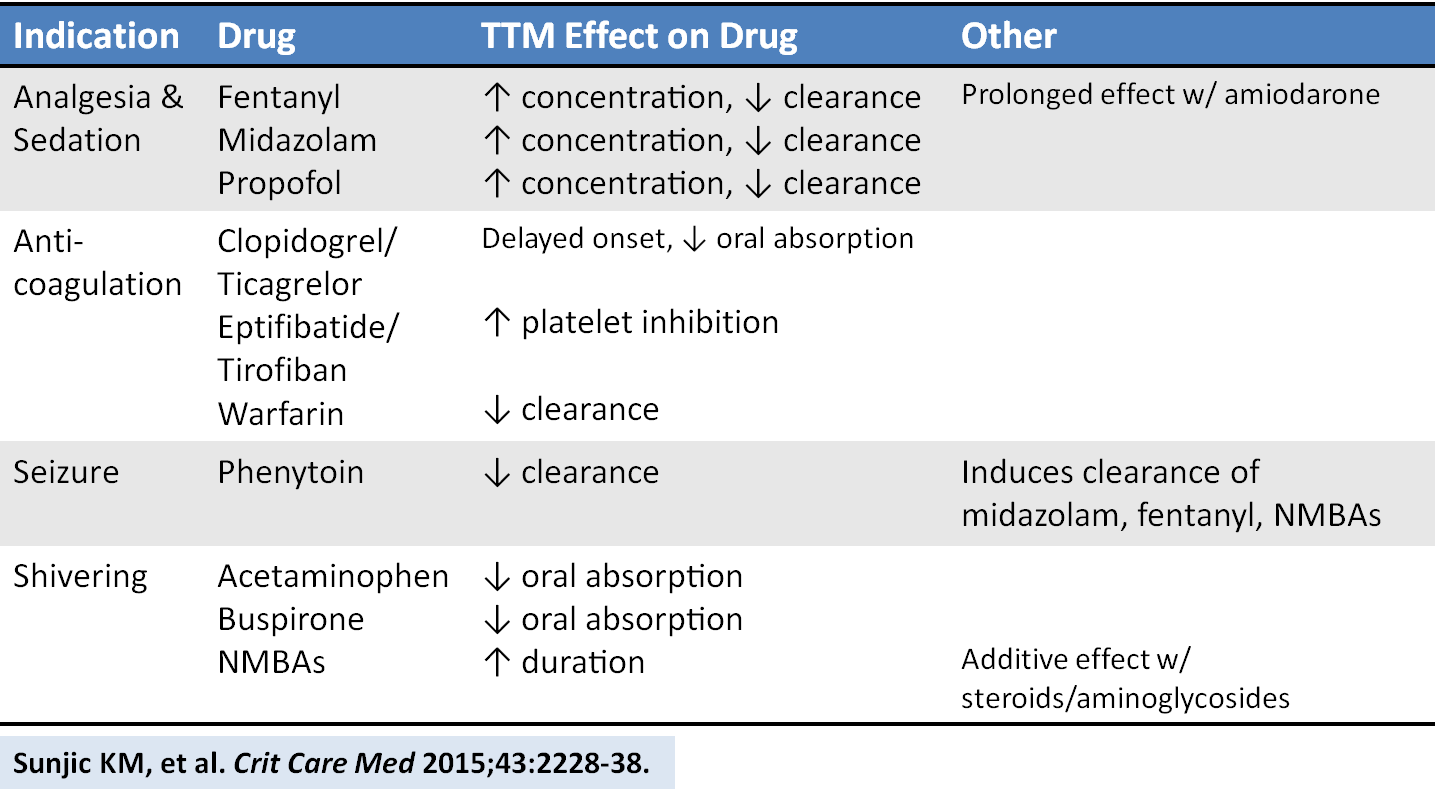
Pain Management in the Critically Ill Patient
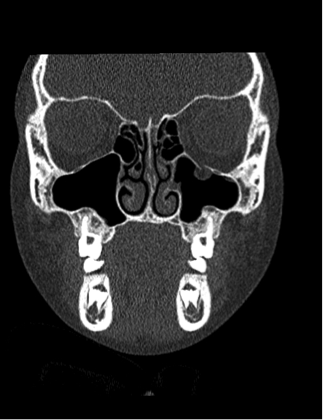
Patient complains of facial and neck swelling, what's the diagnosis?
Happy Halloween!!
I hope you have had a safe and fun Halloween. Thank you to all the people that are staffing the EDs on a Saturday Night Halloween.
Prostate-Selective Alpha Antagonists have been tied to Falls and increased risk of fractues in elderly men. These medications can lead to syncope and hypotension putting patients at increased risk of falls. A recent canadian study showed that at 90 days of use; individuals on alpha antagonists were at increased risk of hospital visits for falls (1.45% vs. 1.28%) or fractures (0.48% vs. 0.41%). There was also an increased risk of head trauma.
Please warn patients that are on these medications of the risks, so that injuries can be minimized. They should take specific care when changing postural positions, and report episodes of lightheadedness to their PCPs.
The article can be found at http://www.bmj.com/content/351/bmj.h5398
A traditional ED practice has been to combine promethazine as an anxiolytic adjunct to morphine for patients with musculoskeletal pain (eg back pain).
However, when compared to morphine alone, this combination does not lead to greater analgesia or decrease anxiety. It does however prolong ED length of stay.
This use of this "pain cocktail" is not recommended
Fever is the most common presenting symptoms to pediatric emergency departments 10-20%
There have been a variety of case reports that have been describing the effects of lipid emulsion therapy on severe hemodynamic overdoses. As time has gone on, we have realized that this therapy is not for all severe overdoses. The type of medication and its pharmacokinetic properties factor into the decision. There is minimal evidence and no ideal randomized control trials that will tell us what the right answer is but take beta-blockers for instance:
Atenolol - in overdose, consider hemodialysis, very effectively removed by HD [1]
Propranolol - very lipophilic and one of the few beta-blockers that can cause widened QRS, seizures as well as the prototypical hypotension and bradycardia.
Because of its lipophilicity, ability to cross the blood brain barrier and ability to cause lethal dysrrthmias, lipid emulsion therapy has been effective in reversing the clinically severe effects of a propranolol overdose. [2]
The World Health Organization (WHO) has just released a report on the current status of road traffic safety globally.
From a postive perspective, road traffic deaths are stabilzing even though the number of motor vehicles are rapidly increasing.
The bottom line- injuries are preventable. Continued policy efforts, laws with enforncement, can save lives. Specific life saving legislation includes:
There is more than the standard preparations of plasma, platelets, and PRBCs in the blood bank. Certain patients will require these specialized preparations when a transfusion is required. Here are three to know:
8 year-old female presents with nausea, vomiting, double-vision and inability to move her left eye upwards after being kicked in the face at school. What's the diagnosis?
Our suspicion of significant abdominal injury increases when there is bruising across the abdomen in adults after a motor vehicle collision, but what about in children? A PECRAN analysis may have provided us with the answer.
Of 3740 pediatric patients after motor vehicle collision, 16% had a seat belt sign. Seat belt sign was defined as a continuous area of erythema, ecchymosis or abrasion across the abdomen due to the seat belt. 1864 children had CT scans of the abdomen. Intra-abdominal injuries (IAI) were more common in those children with seat belt sign than those without (19% versus 12%). Those with seat belt sign had a greater risk of hallow viscous or mesenteric injuries. There was no increased risk of solid organ injury. 33% of patients with seat belt sign did not have complaints of abdominal pain or tenderness on initial exam (with a GCS of 14 or 15); 2% of these patients underwent operative intervention for their injuries.
Toxicity due to body packing and body stuffing can be a significant concern due to unknown quantity and/or substance that was ingested.
A recent prospective observational case series compared the utility of CT abdomen/pelvis with and without PO contrast in identifying the ingested packets.
The gold standard comparison: surgical removal or expulsion of packets.
All patients received CT abd/pelvis with and without PO contrast.
A. Body stuffers (n = 24)
CT w/ PO contrast:
Positive: 7 (sensitivity 29.2%)
Negative: 17
CT w/o PO contrast:
Positive: 9 (sensitivity 36.5%)
Negative: 15
All 24 patients passed ingested packets
B. Body packers (n= 11)
CT w/ PO contrast
CT w/p PO contrast
10 patients expulsed packets; one patient did not have any packets.
Conclusion
Bottom line:
Last month we discussed symptoms of serotonin syndrome and its diagnosis by the Hunter Criteria. Let's move on to what causes serotonin syndrome.
Serotonin Syndrome - What Causes It?

** Stay tuned for the conclusion on management of serotonin syndrome **
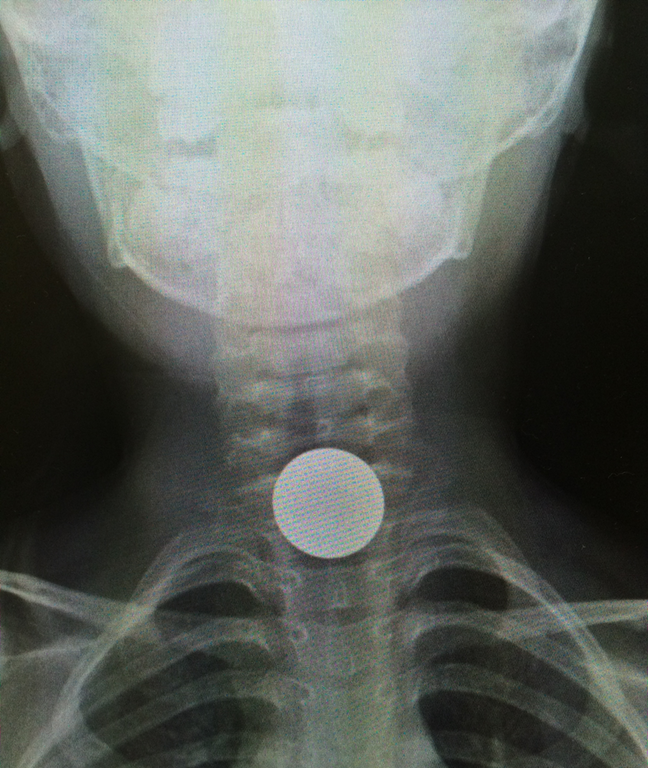
5 year-old boy who presents with sudden onset hoarse voice, and drooling without a fever.
In patients receiving renal replacement therapy as a treatment modality for dabigatran-related bleeding, watch for a rebound concentration increase after hemodialysis is stopped.
More than 50% of patients demonstrate a rebound effect with a median increase in dabigatran concentration of 33%.
It is unclear whether this rebound effect is clinically important, and whether it translates to prolonged clinically relevant bleeding. Extended hemodialysis sessions or consideration of CVVHD should offset this potential problem.
Bonus Pearl:
The North American Congress of Clinical Toxicology starts today and runs through October 12. Look for toxicology pearls and updates on Twitter under the official conference hashtag #NACCT15.
Overall, suicide is the 15th leading global cause of death. However, it is the 2nd leading cause among 15-29 year olds
Suicides are preventable. Interventions to decrease suicides include:
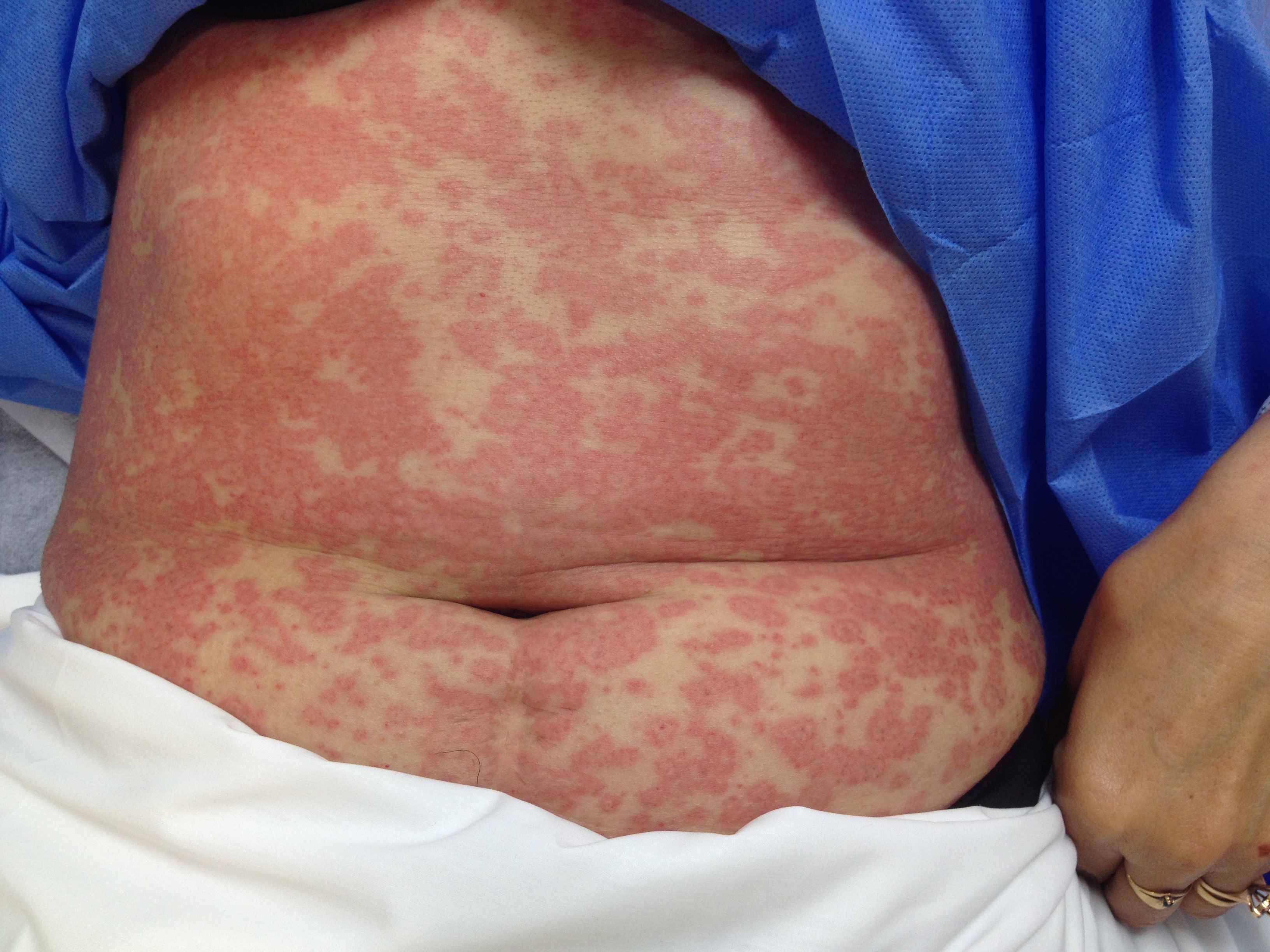
Patient presents after being started on an antibiotic for cellutlitis of lower extremity. What's the diagnosis and what are some other etiologic agents (name 3)
An excellent new review article provides a detailed look at how the drugs we give are affected by targeted temperature management. Here is a helpful chart of drug alterations that have data in reduced body temperature states: