What is the ICH Score?
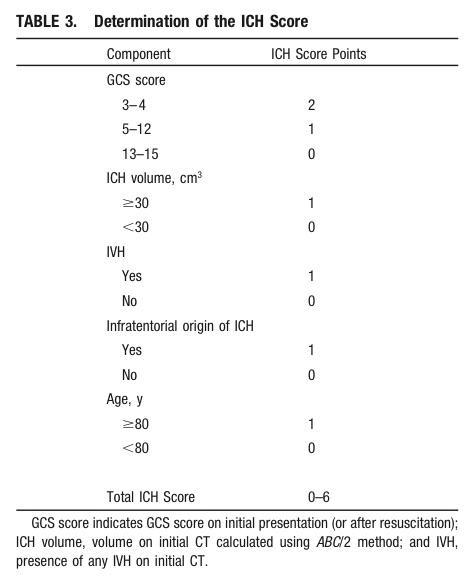
Take Home Point: Communicate the severity of your ICH patient by using either the composite ICH Score or by including details such as the patient's GCS, estimated volume of ICH, presence of IVH, and supra- vs. infratentorial origin.
Intraosseous (IO) placement is a rapid and reliable method for obtaining venous access in critically ill patients; previous studies demonstrated that everything from vasopressors to packed RBCs can be infused through it.
This prospective observational study compared the first-pass success rate and time to successful placement of IO versus landmark-based (i.e., not ultrasound guided) central-line placement (femoral or subclavian access) during medical emergencies (e.g., cardiac arrest) in an inpatient population.
The first pass success rate for IO was found to be significantly higher than the landmark technique (90% vs. 38%) and placement was significantly faster for IOs (1.2 vs. 10.7 minutes).
Despite the fact that this study did not directly compare IO to ultrasound guided line placement, this study demonstrates that IO is a rapid and effective means to obtain central access during patients with emergent medical conditions.
Bottom-line: Consider placing an IO line when rapid central access is necessary.
The following clip is one of three findings found in Beck’s triad. Name all three findings and how often are all 3 signs present for patients with pericardial tamponade?

Vancomycin guidelines recommend an initial dose of 15-20 mg/kg based on actual body weight (25-30 mg/kg in critically ill patients). [1] The MRSA guidelines further recommend a max dose of 2 gm. [2]
But, what dose do you give for an obese patient that would require more than 2 gm?
A new study provides some answers to this question. [3] Obese-specific, divided-load dosing achieved trough concentrations of 10 to 20 g/mL for 89% of obese patients within 12 hours of initial dosing and 97% of obese patients within 24 hours of initial dosing.
Application to Clinical Practice
Caveats
The study used some more specific dosing calculations based on renal function and percentage above IBW. If patient's renal function is abnormal, consultation with a pharmacist is recommended.
Electronic cigarettes are battery-powered devices that deliver nicotine, flavorings, (e.g. fruit, mint, and chocolate), and other chemicals via an inhaled aerosol. E-cigarettes are currently not regulated by the FDA. In many states, there are no restrictions on the sale of e-cigarettes to minors.
Electronic cigarette exposures involving young children are rapidly increasing. Such exposures tend to involve patients aged < 5 years and occur by ingestion of the nicotine-containing liquid. There is a potential for acute nicotine toxicity (nausea, vomiting, pallor, diaphoresis, tachycardia, hypertenstion initially). Respiratory muscle weakness with respiratory arrest is the most likely cause of death.
To date, the overwhelming majority of pediatric ingestions have not resulted in serious medical outcomes. The most commonly reported adverse events were nausea and vomiting.
However, in May of 2014, the first pediatric case of toxicity from ingestion of e-cigarette nicotine liquid was reported. A 10-month old ingested an unknown amount of e-liquid and developed vomiting, tachycardia, grunting respirations, and ataxia. The symptoms resolved by 6 hours after ingestion without specific treatment.
(1) The figure above shows the number of calls to poison centers for cigarette or e-cigarette exposures, by month, in the United States during September 2010 February 2014. E-cigarette exposure calls per month increased from one in September 2010 to 215 in February 2014.
Introduction:
As noted in the previous pearl (May 20, 2015), globally diarrheal diseases are the second leading cause of death for children under five- killing approximately 760,000 annually. What can be done to prevent and treat diarrhea, especially among young children?
Prevention of diarrheal illness:
Treatment of diarrheal illness:
Bottom Line
Diarrheal diseases kill hundreds of thousands of children in developing countries each year. Appropriate prevention measures (clean water, improved sanitation) can markedly decrease the burden of disease. Appropriate treatment (ORS) can save lives for pennies.
High Flow Nasal Cannula (HFNC) in acute respiratory hypoxemia
The Trial:
Results:
Bottom line:
Consider using HFNC prior to or while deciding on intubation in patients with hypoxemic respiratory failure usually due to pneumonia
We all dread performing lumbar punctures on the obese patient. The traditional standard length spinal needle (9 cm) is becoming increasingly inadequate in reaching the subdural space in our overweight society.
Abe et al developed a formula for selecting the proper needle length to reach the middle of the spinal canal from the skin using retrospective CT data from 178 patients.
Length of needle (cm) = 1+ 17 x Weight (kg)/ Height (cm)
Given the average height of the American woman (163 cm or 5’4’’) our standard length spinal needle will FAIL to reach the mid-thecal space if a woman weighs more than 170 lb (75 kg)!!!
Paul Blart Mall Cop, and King of Queens star Kevin James (5’8’’, 285 lb) would require a 13.7 cm spinal needle. This means even our long spinal needles (12.7 cm) would FAIL by 1 cm.
Note that this formula resulted in selection of needles too small (6%) and too long (31%) of the time. Abe’s linear correlation had an R value of 0.81, (p<.001)
Bottom-Line: Consider use of a long spinal needle (12.7 cm) or IR guided LP in overweight /obese patients and the above formula to guide your depth of insertion
Stress-Induced Cardiomyopathy
Do you need to get stuff out of the thorax (like fluid or air) and don't want to place a HUGE chest tube? Consider a pigtail catheter; don't know how to place one? Well check out this video and learn how.
Reperfusion Ventricular Fibrillation
Ventricular fibrillation during reperfusion in STEMI is an infrequent, but serious complication.
Among ~4000 with STEMI between 2007-2012, 71 (1.9%) had reperfusion Vfib.
Increased risk for reperfusion Vfib is associated with: history of MI, aspirin and b-blocker use, Vfib before PCI, left main CAD, inferior MI, symptom-to-balloon time <360 minutes, maximal ST-segment elevation in a single lead >300 μV, and sum of ST-segment deviations in all leads >1,500 μV.
The sum of ST-segment deviations in all leads >1500 μV was an independent predictor of reperfusion Vfib.
Sx: pain to lateral arm, worse with overhead activity and sleeping/lying on arm
Anatomy: Pain generating structures include the rotator cuff, subacromial bursa, labrum and biceps tendon.
http://www.ortho-md.com/images/proceduresImg/SHOULDER2.jpg
Testing: Neer and Hawking tests
https://www.youtube.com/watch?v=U8-yLHQ_JaM
https://www.youtube.com/watch?v=OYK5qL2om-c
Done indepedently, Hawkings is more sensitive, however best to combine both tests.
Imaging: not indicated
Tx: rest, ice, physical therapy (modalities), subacromial steroid injection
Methemoglobin (MetHb) is produce when Fe+2 in heme is oxidized to Fe+3 under oxidative stress (caused by mediation and chemicals). MetHb does not bind to oxygen and thus decrease RBC’s O2 carrying capacity.
Among medication, overdose of local anesthesia - benzocaine, dapsone, and phenazopyridine are often implicated. (Table 1)
Think about methemoglobinemia in presence of low pulse oximetry (~85%) with lack of response to supplemental oxygen, cyanosis, dyspnea, etc. (see Table 2 – signs and symptoms of MetHb) in patients who are taking or overdosed on medication listed in Table 1.
Diagnosis: CO-oximetry detects toxin-induced hemoglobinopathies, including COHb and MetHb.
Treatment: Methylene blue (1 mg/kg over 5 min) in symptomatic patients or MetHb level > 25%. Resolution of methemoglobinemia should be noted in 30 – 60 min.
G6PD deficiency: Prevalence in the U.S. is 4-7% with highest prevalence in African American population (11%). Methylene blue causes hemolytic anemia in patients with G6PD deficiency within 24 hours of administration. However, G6PD status is often unknown in ED patients. When caring for patients with known G6PD deficiency and methemoglobinemia, providers must carefully consider the risk and benefit of treating MetHb (including severity of poisoning/MetHb) with methylene blue.
Table 1. Causes of MetHb
| Medication
| Chemicals |
| Benzocaine, Lidocaine, Prilocaine | Aniline dye |
| Dapsone | Chlorobenzene |
| Phenazopyridine | Organic nitrites (e.g. isobutyl nitrite) |
| Nitroglycerin | Naphthalene |
| Nitroprusside | Nitrates (well water contamination) |
| Quinones (Primaquine & Chloroquine) | Nitrites (food preservatives) |
| Sulfonamides | Silver nitrate |
| Nitric oxide | Trinitrotoluene |
| Amyl nitrite |
|
Table 2. Signs and symptoms
| MetHb level (%) | Signs and symptoms |
| 1-3% (normal)
| · None |
| 3-15% | · Low pulse oximetry (<90%) · Gray cutaneous coloration |
| 15-20% | · Chocolate brown blood · Cyanosis |
| 20-50% | · Dizziness, syncope · Dyspnea · Weakness · Headache |
| 50-70% | · CNS depression, coma, seizure · Dysrhythmias · Tachypnea · Metabolic acidosis |
| >70% | · Death · Hypoxic injury |
Background:
While diarrhea in adults can be inconvenient and briefly debilitating, in children it can be fatal. Globally, diarrheal diseases are the second leading cause of death for children under five.
Clinical types of Diarrhea (with common infectious causes):
Clinical assessment:
*Best indicators of hydration status
Next week: Prevention and Treatment
Advances in Catheter-Directed Therapy for Acute PE - The PERFECT Registry
Earlier this month, initial results from the multicenter PERFECT registry (Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis) were released. In this study, 101 consecutive patients with massive or submassive PE were prospectively enrolled to receive early catheter-directed therapy.
Inclusion criteria:
Therapy provided:
Outcomes: Clinical success (stabilization of hemodynamics, improvement in pulmonary hypertension and/or right heart strain, and survival to discharge) was achieved in 86% of patients with massive PE and 97% of patients with submassive PE. There were no major procedure-related complications or major bleeding events.
Bottom Line: In patients with massive or submassive pulmonary embolism, there is growing evidence that early catheter-directed therapy may become first-line therapy for selected patients.
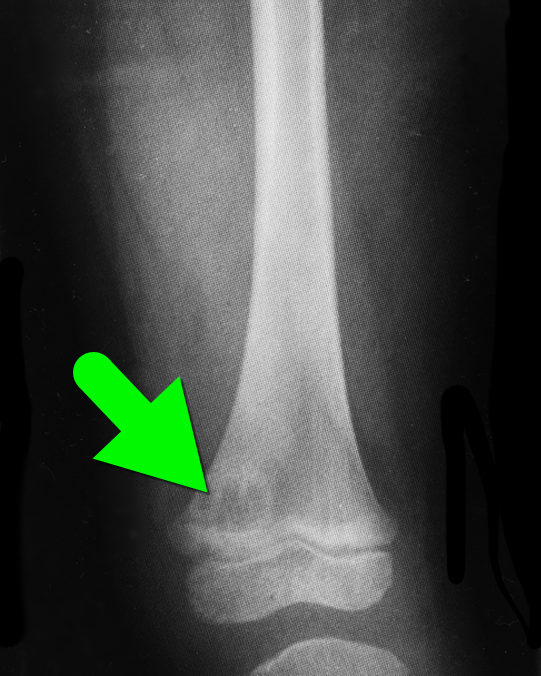
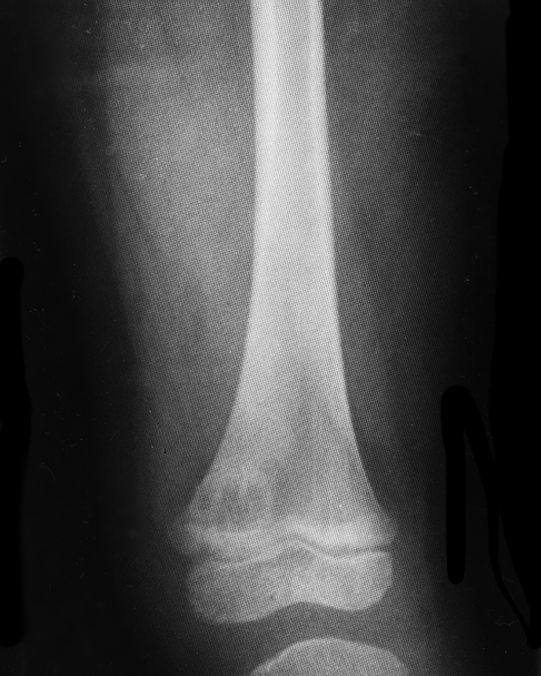
5 year-old with no past medical history, complains of a limp and mild left knee pain. No history of trauma. Physical exam is significant for a low-grade fever and is otherwise normal. What’s the diagnosis?
Tensor Fascia Latae (Iliotibial Band) Pain Syndrome:
Some patients will complain of hip and back pain and can have multiple visits before somebody considers Tensor Fascia Latae Pain Syndrome AKA Iliotibial Band Syndrome.
The tensor fascia latae helps with thigh flexion at the hip, abduction, and medial rotation; and stabilizes the knee laterally
When this muscle/fascia gets tight and overcontracted it will lead to dysfunction of the gluteus and rectus femoralis muscles leading to increased hip pain due to abnormal movement of the joint.
Patients often complain of increased pain with running, especially downhill and exam is notable for local tenderness (approx. 2cm above lateral joint line) & occasional swelling over the distal lateral thigh.
Most patients respond to conservative treatment involving NSAIDs, stretching of the iliotibial band, physical therapy, strengthening of the gluteus medius, and altering their running regimens.
Lice are spread through direct contact as they crawl. Indirect contact (through brushes or hats) is less likely. One study showed that live lice were found in only 4% of infested volunteers pillowcases.
During an initial infestation, lice can reside on the head for up to 4 to 6 weeks before becoming symptomatic. Therefore, when lice are detected at school, there is no need to send the child home (or to the ED). Children also do not need to be kept out of school while receiving treatment.
Bonus: First line treatment is 1% Permethrin applied on day 0 and 9. The patient should wash their hair first with a non conditioned shampoo, apply Permethrin for 10 minutes and then rinse.
Dabigatran is an orally administered, potent, direct thrombin inhibitor approved for the prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, and for the treatment and secondary prevention of venous thromboembolism.
Several pharmacokinectic studies have suggested that dabigatran possesses a number of ideal properties for expedited removal via extracorporeal methods. Dabigatran has low oral bioavailability (3-7%) and is predominantly cleared (80%) by the kidneys. It is not significantly protein bound, low-to-moderate steady state volume of distribution, and has a low molecular weight. All of these attributes make it a candidate for extracorporeal removal. Low protein binding may suggest redistribution into the plasma post extracorporeal removal.
Dabigatran is a substrate for the multidrug efflux transporter P-glycoprotein. Administration of the drug with potent P-glycoprotein inhibitors (ketoconazole, verapamil, amiodarone, quinidine) may significantly increase risk of toxicity, i.e. bleeding.
Most of the current evidence is based on case reports/case series where HD was the primary mode of removal.
Caution: Redistribution effect in plasma dabigatran concentration was also observed in several cases within 20 min to 12 hours post cessation of renal replacement therapy. Other limitations include:
1) Hemodynamic instability such as hypotension that may make initiation of extracoporeal removal difficult
2) Availability of indicators demonstrating effectiveness of extracorporeal removal
3) Amount of time needed to prepare patient to receive extracorporeal therapy
4) Use of extracorporeal removal as a treatment modality has not been prospectively evaluated
Bottom line: Extracorporeal removal may be an option for patients in the setting of life-threatening bleeding but with consideration of several limitations and should not preclude or delay use of other supplemental hemostatic therapies.