Elevation of AST or ALT >1000 after acute ingestion of acetaminophen indicate hepatic toxicity. N-acetylcysteine (NAC) is an effective treatment for acute acetaminophen poisoning. However, in a setting a significant transaminitis, (> 1000s) NAC infusion is continued beyond the routine 21-hour protocol.
Currently, there is no specific guideline or “level” of AST or ALT where discontinuing NAC is deemed safe and appropriate.
A recent retrospective study (n = 37 patients with 343 pairs of AST/ALT) evaluated AST/ALT ratio as a possible indicator for discontinuing NAC infusion after an acute acetaminophen induced hepatic toxicity.
This study found that post peak AST/ALT ratio of < 0.4 had sensitivity of 99% for identifying patients with resolving hepatic injury.
This finding requires validation prior to clinical application but this may be the first step to identifying a safe indicator to help guide clinician when NAC can be discontinued safely.
Whether in the U.S. or overseas, there are four main phases of emergency management:
The results of a multi-center trial from the UK, the ProMISe trial, were just released and it confirms what two prior studies (i.e., ProCESS and ARISE) have already shown; there does not appear to be any difference in mortality when septic patients are treated with a strategy of early-goal directed therapy as compared to usual care.
Patients were included in the ProMISe trial if they were in septic shock and were then randomized to either the EGDT group (630 patients) or the usual care group (630 patients); a total of 1,260.
The primary end-point was all cause mortality at 90 days and there was no difference shown in the primary outcome. There were no differences found in the measured secondary outcomes (e.g., serious adverse events)
This trial adds to the evidence that septic patients may not benefit from protocolized (i.e., EGDT) care versus usual care. One explaination why, is that our "usual care" in 2015 has significantly changed since the introduction of EGDT in 2001.
Imaging plays an important role in the evaluation of child abuse.
It aids in the identification, evaluation and in treatment.
Additionally, it is often the only objective evidence of abuse available to the courts.
It is often discovered through two means.
1) Injuries/fractures that are inconsistent with the alleged mechanism of injury.
2) Pathognomonic fracture patterns are found on routine radiographs
The ED physician should not attempt to precisely "date" the injury.
That said, soft tissue swelling resolves in 2-5 days. The periosteum becomes radiodense in 7 to 10 days. In subtle fractures this may be the only radiographic finding. If there is no evidence of bone healing (periosteal reaction), the fracture is less than 2 weeks old. Callus formation and resorption of the bone along the fracture line begins at 10 to 14 days. The callus is visible for up to 3 months. Bone remodeling continues for up to one year.
In the midst of an unprecedented opioid epidemic, there have been considerable efforts to expand access to naloxone (Doyon S, et al. J Med Toxicol 2014;10:431-4). If the situation arises when you need to write a prescription for it, here's how:
Option 1: Naloxone vial and needle traditional IM/SQ using 0.4 mg/mL injection vial and needles (least expensive $40, FDA approved)
Naloxone 0.4 mg/mL single dose vial and 3 cc, 23 g, 1 inch syringes, #2 each
SIG: Inject 1 mL intramuscularly upon signs of opioid overdose. May repeat X 1. Call 911.
Option 2: IMS/Amphastar 2 mg/2 mL prefilled syringe and mucosal atomization device ($95/kit, products FDA approved but intranasal administration is off-label)
Naloxone 2 mg/2 mL prefilled syringe and intranasal atomizer device, #2 each
SIG: Spray one-half of syringe (1 mL) into each nostril upon signs of opioid overdose. May repeat X 1. Call 911.
Option 3: Evzio Autoinjector ($200-700 per Rx though many insurances cover it and the company has vouchers available, FDA approved in 2014, evzio.com/hcp)
Evzio 0.4 mg, #1 two-pack
SIG: Use as directed upon signs of opioid overdose. May repeat X 1. Call 911.
Cauda Equina Syndrome is a true neurologic and surgical emergency. Unfortunately, no constellation of symptoms or exam findings is 100% sensitive. In fact, no single symptoms predicts the radiographic finding of cauda equina syndrome with an accuracy greater than 65%.
The most common symptoms are sciatica (96%), micturition dysfunction (89%), saddle anesthesia or hypoethesia (81%) and defecation dysfunction (47%).
Transfusion in Major Trauma: The PROPPR Trial
What should we be transfusing in major trauma?
The Trial
Results
Conclusions
How does this affect my practice?
A 1:1:1 transfusion practice is safe and can decrease mortality from hemorrhage in major trauma
Other points: control bleeding, permissive hypotension, avoid crystalloids, use TEG to guide therapy (TXA etc)
35 year-old female presents with acute leg pain and swelling. What's the diagnosis?

Afib Clinical Decision Aid: AFFORD
- Atrial fibrillation (AF) affects ~34 million people worldwide; the hospital admission rates vary with frequencies of 81%, 62%, and 24% in the US, Australia, and Canada respectively.
- Lack of a reproducible and accurate risk stratification/decision aid likely contributes to variability in ED disposition.
- AFFORD (Atrial fibrillation and flutter outcome risk determination) was the 1st clinical decision aid (contains 17 variables) to predict 30-day adverse events in a prospective ED patient cohort with acute symptomatic AF.
- Vanderbilt University Medical Center's ED (2010-2013) derived and internal validated an ED based clinical decision aid for prediction of MACE within 30 days utilizing the AFFORD decision aid in hemodynamically stable patients whose AF reverted to sinus rhythm, either spontaneously or after cardioversion (pharmacologic or electrical), and those who are adequately rate controlled and candidates for outpatient management.
- Incorporating AFFORD with a shared decision model into ED practice may help identify patients at low risk and potentially reduce rate of hospitalizations.
Emergency Departments are increasingly searching for alternatives to opioids for acute pain management.
An urban trauma center in California retrospectively evaluated their use of low-dose ketamine for acute pain over a two-year period. [1]
Application to Clinical Practice
There was no comparison group and there was no mention of what other pain medicines were given. Adverse events are often under-reported in retrospective studies. This study seems to demonstrate that low-dose ketamine administration for acute pain management in the ED is feasible with a low rate of adverse effects.
It's worth noting that a new review of 4 randomized controlled trials evaluating subdissociative-dose ketamine found no convincing evidence to support or refute its use in the ED. The 4 included trials had methodologic limitations. [2]
Background: While much of international health focuses on communicable diseases, it is clear that noncommunicable diseases (NCDs), such as cardiovascular diseases, cancer and diabetes, causes substantial morbidity and mortality.
Epidemiology:
Bottom line: As in developed countries, risk factors for NCDs deaths include physical in activity, tobacco use, unhealthy diabetes, harmful use of alcohol.
High-Flow Nasal Cannula for Apneic Oxygenation
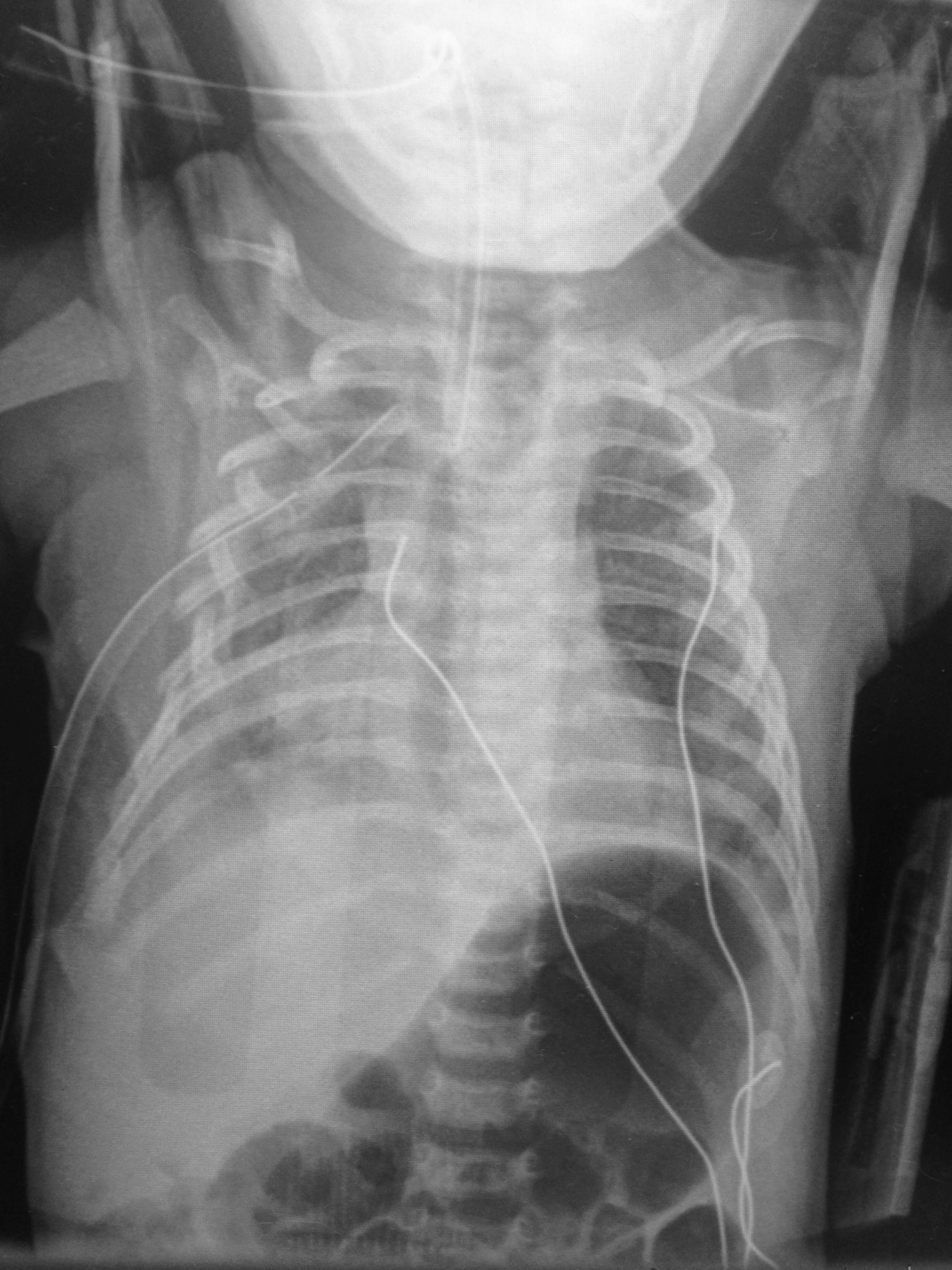
6 day-old child is brought in by parents with 1 day of reduced oral intake and 4 hours of rapid breathing. The child has no fever and no significant birth history. The child is tachycardic, hypotensive, and hypoxic. What’s the diagnosis?
Safety Risk? Digoxin in Atrial Fibrillation
- Digoxin is commonly utilize for atrial fibrillation/flutter with rapid ventricular response, though beta blockers and/or calcium channel blockers are a better 1st line therapy given digoxin’s narrow therapeutic index and lack of mortality benefit.
- Digoxin in the acute setting is often favored given its ability to reduce the heart rate while maintaining or slightly augmenting blood pressure.
- 2014 AHA/ACC guidelines recommend digoxin, specifically for rate control in patients with heart failure and/or reduced ejection fraction.
- There have been 2 post hoc studies from the AFFIRM trial which showed conflicting results w/regards to digoxin and risk of mortality.
1. Increased risk of mortality associated w/digoxin (on-treatment analytic strategy)
2. No association w/mortality (intent-to-treat analytic strategy)
- A recent retrospective cohort examination of newly diagnosed afib patients without heart failure & no prior use of digoxin; digoxin was independently associated with a 71% higher risk of death & a 63% higher risk of hospitalization.
- Consistent and substantial increase in mortality and hospitalization risk was seen using both on-treatment and intent-to-treat analytic methods.
- Given other available rate control options, digoxin should be used with caution.
Sesamoid Injuries
The first MTP joint contains the 2 sesamoid bones. They play a significant part in the proper functioning of the great toe. 30% of individuals have a bipartite medial or lateral sesamoid.
http://www.coreconcepts.com.sg/mcr/wp-content/uploads/2008/05/sesamoid_foot.jpg
Injury can occur from trauma, stress fracture or sprain of the sesamoid articulation or of the sesamoid metatarsal articulation. Overuse injuries tend to occur in sports with a great deal of forefoot loading (basketball/tennis).
SXs: Pain with weight bearing, pain with movement of first MTP, ambulation on lateral part of foot.
PE: Tenderness and swelling over medial or lateral sesamoid. Resisted plantar flexion (flexor hallucis) reveals pain and weakness.
Imaging: plain film with sesamoid view to assess for a sesamoid fracture. Stress fractures may take 3-4 weeks to show on plain film.
http://www.agoodgroup.com/running/Fracture002.jpg
Treatment for fractures and suspected stress fractures involve 4 to 6 weeks of non weight bearing.
Orthopedic Causes of Chest Pain
The first thing that pops into everybody’s mind when they hear a patient state they have chest pain radiating to the left arm is Acute Coronary Syndrome and specifically a Myocardial Infarction. However, there are a lot of orthopedic causes of chest pain that can also radiate to the left arm. It is estimate that up to 20% of patients with pectoral symptoms have an underlying orthopedic problem.
Some of them are:
Some other less common causes are
So instead of just ordering some troponin and admitting to medicine, consider that the cause can be orthopedic in origin.
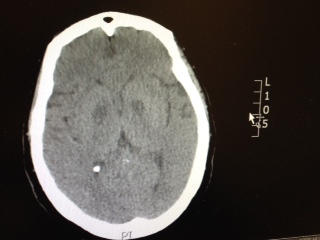
Patient has the following Head CT, what is your differential diagnosis? There are only a few characteristic toxins that can cause this type of finding on CT.