The pattern of prescription drug abuse continues to center around semisynthetic opioids like oxycodone and hydrocodone. Federal regulations have now raised hydrocodone to a schedule II drug like oxycodone. Despite efforts, the slope for natural and semisynthetic opioids remains steep. The ED measures of education, limit prescriptions for acute pain, minimize number of days/pills prescribed and utlize the prescription drug monitoring program are some basics that can assist you in better prescribing habits.
Tips for the inpatient management of community acquired pneumonia
Patient presents with dyspnea & hypoxemia (pulse oximeter is 80%). The "stat" CXR is delayed, but ultrasound is not. What's the diagnosis and what are some differential diagnoses?
Management of Felons
For good photos of the incision technique please visit the reference article listed.
A new population-based case-control study in older adults has linked the administration of trimethoprim-sulfamethoxazole (Bactrim, TMP-SMX) to increased risk of sudden death in patients also receiving angiotensin converting enzyme inhibitors (ACE-I) or angiotensin receptor blockers (ARB). [1]
Hyperkalemia is the suspected cause. [2] Compared to amoxicillin, TMP-SMX was associated with an increased risk of sudden death (adjusted odds ratio 1.38, 95% confidence interval 1.09 to 1.76) within 7 days of exposure to the antibiotic.
Practice Change
In older patients receiving ACE-Is or ARBs, TMP-SMX is associated with an increased risk of sudden death. When appropriate, alternative antibiotics should be considered.
Anisocoria, or unequal pupil sizes, is a common condition. Approximately 20% of the normal population have physiologic anisocoria. However, pathologic anisocoria indicates disease of the iris, parasympathetic pathway or sympathetic pathway. A systematic approach to the evaluation of anisocoria can help differentiate between etiologies that range from benign to life threatening.
The most important question in the evaluation of anisocoria is whether both pupils are normally reactive to light or is one (or both) poorly reactive. If both pupils are reactive, the smaller pupil is abnormal and the lesion is likely in the sympathetic pathway because pupillary constriction (parasympathetic pathway) is intact. If one pupil is poorly or non-reactive (and there is no relative afferent pupillary defect), the larger pupil is abnormal and the lesion is likely in the parasympathetic pathway.

DDx of anisocoria with normally reactive pupils:
DDx of anisocoria with poorly or non-reactive pupil:
Aminoglycosides in Critically Ill Patients
Parasternal long-axis of two different patients. What is the:
Coronary Subclavian Steal Syndrome
Coronary subclavian steal syndrome (CSSS) is defined as coronary ischemia resulting from the reversal of flow in an internal mammary arterial graft usually secondary to subclavian stenosis.
Angiographic subclavian stenosis is defined as greater than 50% narrowing or greater than 20mmHg pressure difference across a lesion.
CSSS occurs in up to 4.5% of patients with prior CABG & common in older individuals with existing peripheral vascular disease.
CSSS most commonly manifests as stable angina, but frequently presents as unstable angina, acute myocardial infarction, acute systolic heart failure or even cardiogenic shock.
Screening for subclavian stenosis prior to CABG w/bilateral noninvasive blood pressure assessment, and a 15 mmHg or greater discordance should elicit further imaging.
Percutaneous revascularization is the first-line therapy for CSSS and has excellent long-term outcomes.
Beware of spontaneous reduction masking the true injury!
Knee dislocations are rare due to supporting ligaments (MVCs, falls, sports)
but can be seen after minor trauma in obese patients.
Named by the direction of the displacement of the tibia relative to the femur
- Anterior and posterior are most common
Dislocations involve disruption of at least 2 of the major knee ligaments (ACL/PCL most common)
Usually associated with large hemarthrosis however capsular tearing may allow dissipation of the blood into adjacent soft tissue.
Consider a spontaneously reduced knee dislocation in those with a significant mechanism of injury in the setting of multidirectional instability,
Emergency Physician Bedside Ultrasound for Appendicitis
Why?
To reduce length of stay, improve patient care, and reduce radiation exposure in young patients.
How?
Start with pain medication so you get a better study. (Consider intranasal fentanyl for quicker pain relief and diagnostics in pediatrics.) Study results are also improved with a slim body habitus.
Place the patient supine
Use a high-frequency linear array transducer
Start at the point of maximal tenderness in the RLQ
Transverse and longitudinal planes "graded compression" to displace overlying bowel gas which usually has peristalsis (See Sivitz, et al article for images of "graded compression")
Appendix is usually anterior to the psoas muscle and iliac vein and artery as landmarks
Measure from outer wall to outer wall at the most inflamed portion of the appendix (usually distal end)
Example:
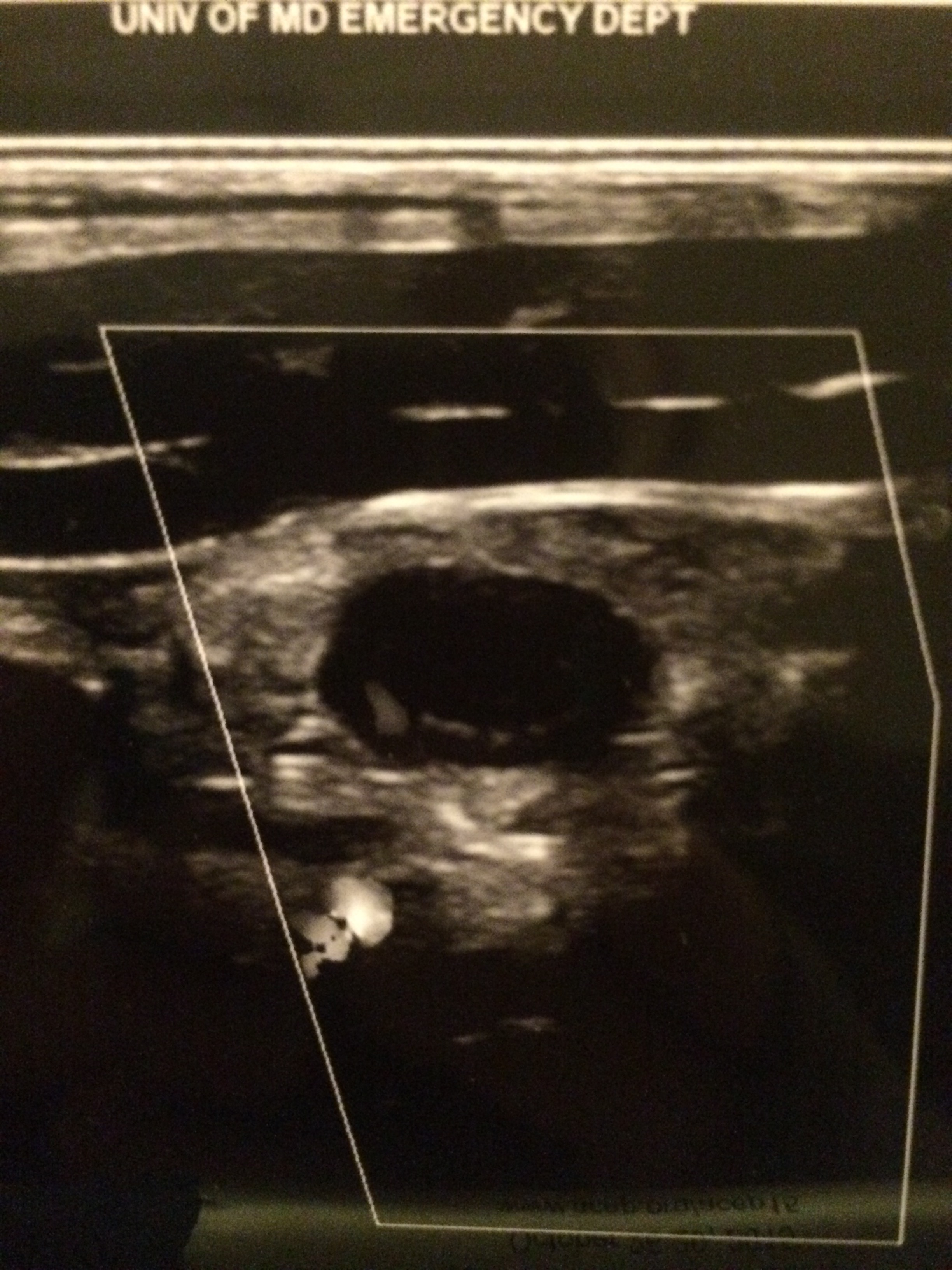
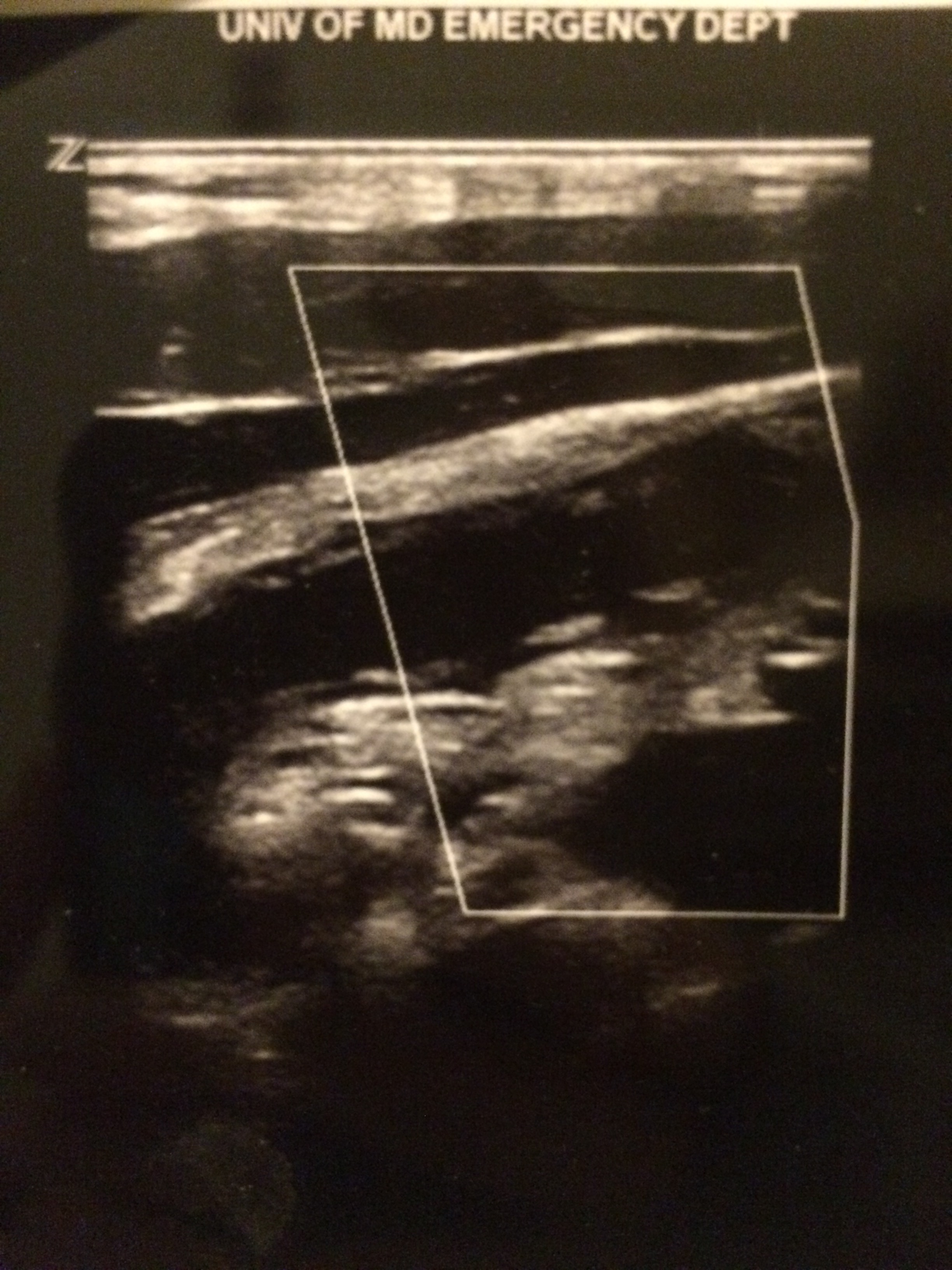
Positive study:
A non-compressible, blind-ending tubular structure in the longitudinal axis >6 mm without peristalsis (see second image above with 8.3 mm diameter measurement)
A target sign in the transverse view (see first image above)
Additional suggestive findings: appendiceal wall hyperemia with color Doppler, appendicoliths hyperechoic (white) foci with an anechoic (black) shadow, periappendiceal inflammation or free fluid
Negative study:
Non-visualization of the appendix with adequate graded compression exam in the absence of free fluid or inflammation.
Limitations for visualization and possible false negative result:
Retrocecal appendix and perforated appendix are difficult to visualize with US.
Pitfalls:
US has good specificity (93% in Sivitz et al article), but limited sensitivity (85% in Sivitz et al article), so trust your clinical judgement. You may need a MRI (pregnant/pediatrics) or CT as they have improved, but not perfect sensitivity.
Digoxin-specific antibodies are produced in immunized sheep and have high binding affinity for digoxin and, to a lesser extent, digitoxin and other cardiac glycosides. The Fab fragment binds free digoxin and once the digoxin-Fab complex is formed, the digoxin molecule is no longer pharmacologically active. The complex is renally eliminated and has a half-life of 14-20 hours (may increase 10-fold with renal impairment). Reversal of signs of digoxin/digitalis intoxication usually occurs within 30-60 minutes, with complete reversal varying up to 24 hours.
Contraindication: None known. Caution is warranted in patients with known sensitivity ot ovine (sheep) products. Product may contain traces of papain and caution advised in patients with allergies to papain, papaya extracts, chymopapain.
Adverse effects:
1) Monitor for potential hypersensitivity reactions and serum sickness
2) In patients with renal insufficiency and impaired renal clearance of dig-Fab complex, a delayed rebound of free serum digoxin levels may occur
3) Removal of the effect of digoxin/digitalis may exacerbate preexisting heart failure
4) Removal of digoxin/digitalis effect may cause hypokalemia
Laboratory interaction: Digoxin-Fab complex cross-reacts with the antibody commonly utilized in quantitative immunoassay techniques. This results in falsely high serum concentrations of digoxin due to measurement of the inactive Fab complex. Therefore, measure free digoxin levels, which may be useful for patients with renal impairment.
Dosing: Each vial of Fab product binds 0.5 mg of digoxin.
Digoxin-specific Fab (round up vial calculation)
# of vials = Digoxin concentration (ng/mL) x Pt Wt (kg)
100
Background: The Centers for Disease Control and Prevention (CDC) classifies potential bioterrorism agents into three categories, with Category A the most deadly.
Category A: These are the highest priority agents/diseases because they:
Specific Category A Agents/Diseases:
Bottom Line: With the exception of smallpox, these disease still occur in various parts of the globe including the United States. As can be seen by the current Ebola epidemic in West Africa, the U.S. public health system and healthcare providers must be prepared to recognize and treat these agents.
A patient presents post-motor vehicle crash with chest pain and dyspnea. The lung ultrasound is shown below. What's the diagnosis?
Back 2 Basics Series: Your Simple RSI Checklist - SOAP ME
The use of a checklist during high stress medical procedures is often recommended. Rapid sequence intubation (RSI) is a classic situation where having a checklist can ensure adequate preparation however, if you don’t have a checklist – this simple mnemonic will make sure you are well prepared for a successful intubation.
| Mnemonic – “SOAP ME” | |
|---|---|
| Suction |
|
| Oxygen |
|
| Airways |
|
| Positioning |
|
| Monitors & Meds |
|
| EtCO2 & other Equipment |
|
The SOAP ME mnemonic is a quick and useful technique to remember only the basics of airway management and preparation. Always remember to also assign roles to team members and communicate clearly to maximize your chances of success.
Heart Failure & Pulmonary Hypertension (Part II)
- HFpEF-PH management guidelines recommend the treatment of symptoms of congestion and volume overload, targeting LV relaxation and co-morbidities; including the management of pulmonary congestion, ischemia, sleep apnea, atrial fibrillation, and diabetes.
- Both atrial/ventricular dysrhythmias contribute to the mortality associated with HF & control of particularly atrial fibrillation, is an essential part of the early pulmonary vascular remodeling process.
- Both endothelin receptor antagonists (ERA) and prostanoids have been effective for PAH & clinical trials utilizing these agents have also been attempted in treatment of PH due to left heart disease, but have proven to be either neutral or even detrimental.
- Selective dilation of the pulmonary vessels in patients with postcapillary PH, without simultaneously ensuring the unloading of the LV, can cause profound pulmonary venous congestion resulting in sudden pulmonary edema, which greatly increases the morbidity in patients with this form of PH.
- Currently, the most compelling published data for pharmacological treatment targeting PH in HFpEF involves phosphodiesterase (PDE) inhibitor sildenafil.
The cross-reactivity between cephalosporins and penicillins is significantly lower than the 10% figure many of us learned. In fact, the beta-lactam ring is rarely involved. So, when the warning pops up next time you order ceftriaxone in a penicillin-allergic patient, what should you do?
In a patient with a documented penicillin allergy, here is a simple chart to help determine when a cephalosporin is ok to use:
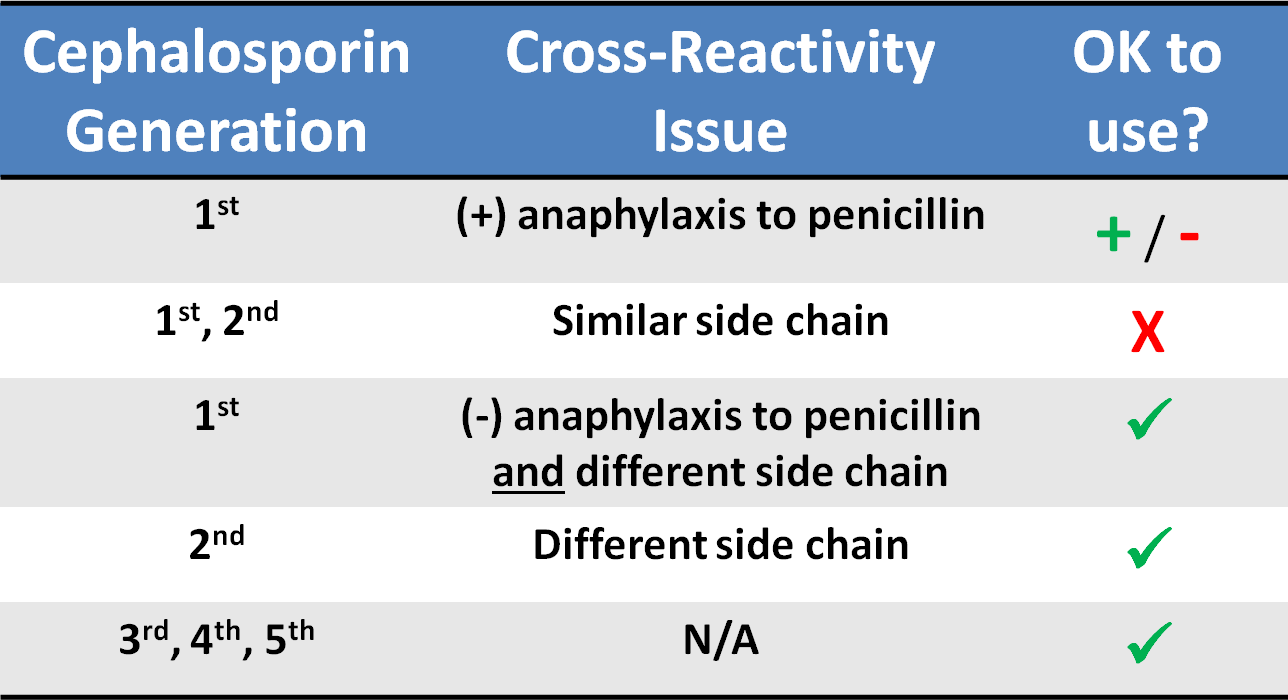
Common penicillins and cephalosporins with similar side chains include ampicillin/amoxicillin and cephalexin, cefaclor, cephadroxil, and cefprozil.
Background:
ED Algorithm For Patients with Possible Ebola
If yes to both identification questions, then:
Bottom line:
Whether the patient has Ebola or not, a well-developed response is necessary for patient management and public health preparedness. The fear of the disease is much more widespread and impactful than the disease itself.
See the full algorithm, with more details at: http://www.cdc.gov/vhf/ebola/pdf/ed-algorithm-management-patients-possible-ebola.pdf
Heart Failure & Pulmonary Hypertension (Part I)
~50% of patients with heart failure & preserved ejection fraction (HFpEF) develop pulmonary hypertension (PH)
HFpEF with PH portends reduced survival and increased hospitalization rates compared to those without PH
HFpEF-PH is often confused with idiopathic pulmonary hypertension (IPAH) given the similar hemodynamics; differentiating them is challenging and requires careful consideration of clinical, radiologic, and hemodynamic data
|
| PAH | HFpEF |
| Clinical parameters: | ||
| Age | Typically 3rd–5th decade | Typically 6th–8th decade |
| Comorbidities (HTN, HLD, DM, CAD) | Rare | Common |
| Atrial arrhythmias | Rare | Common |
| Obstructive sleep apnea | Rare | Common |
| Echocardiographic parameters: | ||
| LA size/volume | Normal | Increased |
| LV diastolic function | Normal to mildly abnormal | Moderate to severely abnormal |
| Hemodynamic parameters: | ||
| Resting PAWP | Always <15 mmHg | May be < or >15 mmHg |
| Response to volume | PAWP <15 mmHg (increase ≤5 mmHg) | PAWP >15 mmHg (increase >5 mmHg) |
| Response to exercise | PAWP <15 mmHg (increase ≤5 mmHg) | PAWP >15 mmHg (increase >5 mmHg) |
(Table reproduced from article)
Iliocostal syndrome aka iliocostal friction syndrome
Consider this entity in an elderly patient with osteoporosis with unexplained abdomen/flank or back pain.
Osteoporosis and/or vertebral compression fractures can result in a narrowing of the distance between .
the lowest anterior rib and the top of the iliac crest producing pain where this rib contacts the pelvis.
This can be perceived as side or back pain. This pain can restrict walking leading to a possible misdiagnosis of spinal stenosis. Treatment is with physical therapy and therapeutic injection.
http://www.caringmedical.com/wp-content/uploads/2013/09/iliocostalis.syndrome.jpg