Beta-lactam antimicrobials (penicillins, cephalosporins, and carbapenems) are frequently used for empiric and targeted therapy in critically ill patients. They display time-dependent killing, meaning the time the antibiotic concentration is above the minimin inhibitory concentration (MIC) is associated with improved efficacy.
Two new pharmacodynamic/pharmacokinetic studies suggest that current beta-lactam antimicrobial dosing regimens may be inadequate.
Antimicrobial dosing in critically ill patients is complex. Current dosing of beta-lactams may be inadequate and needs to be studied further with relation to clinical outcomes.
INFLUENZA
What is it?
Why do we care about influenza?
Bottom line
Cardioactive steroids are among the many treatments used for CHF, and for the control of ventricular response rate in atrial tachydysrhythmias. There are many sources of cardioactive steroids:
Pharmaceutial: Digoxin, Digitoxin
Plants: Oleander, Yellow Oleander, Foxglove, Lily of the Valley, Dogbane, Red Squill
Animal: Bufo marinus toad
It is a potent Na+-K+-ATPase inhibitor and can lead to hyperkalemia in acute ingestion with associated signs and symptoms of N/V, abdominal pain, bradycardia and possibly, hypotension.
Toxicity should be suspected with bidirectional ventricular tachycardia or atrial tachycardia with high-degree AV block
Therapeutic range of digoxin of 0.5 - 2.0 ng/mL is helpful but not a sole indicator of toxicity
Indication for antidote (Digoxin-specific Antibody Fragments) include:
1) Digoxin-related life-threatening dysrhythma
2) Serum K+ > 5.0 mEq/L in acute ingestion
3) Serum digoxin concentration >15ng/mL at any time, or >10 ng/mL 6 hours postingestion
4) Ingestion of 10 mg in adult; 4 mg in pediatric
5) Poisoning by non-digoxin cardioactive steroid
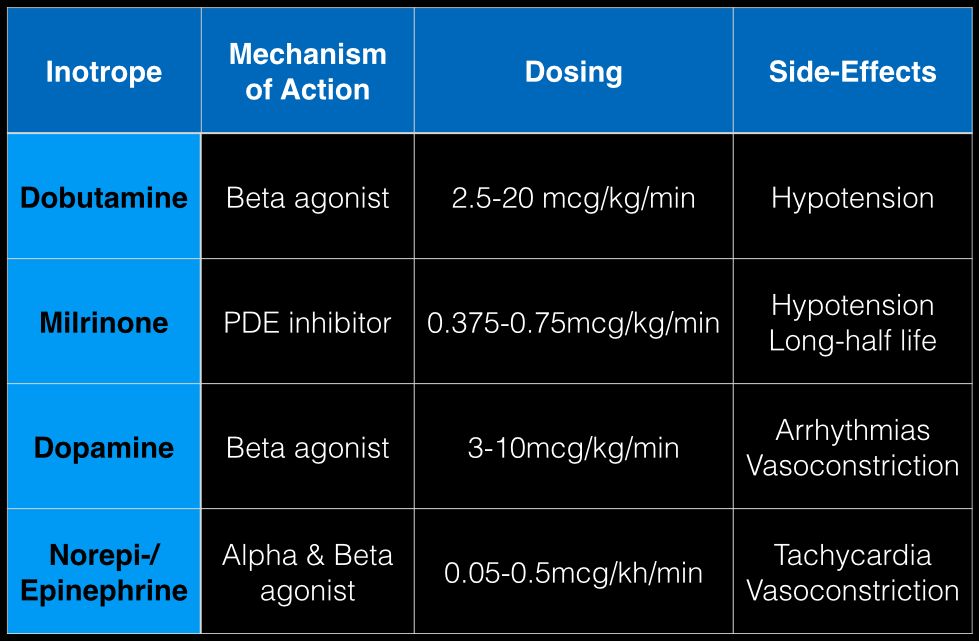
The last Back to the Basics post discussed the use of vasopressors to improve hemodynamics by increasing arterial (and venous) tone. This time we’ll discuss the use of agents to increase inotropy for patients with severe systolic dysfunction / failure.
Dobutamine: a direct b1 and b2-receptors agonist. It has no peripheral vasoconstrictor properties, so if blood pressure increases it occurs secondary to increased cardiac output. Unfortunately, blood pressure may be decreased in some patients due to its peripheral vasodilatory effects; in these cases it may need to be used with a vasopressor.
Milrinone: augments contractility by increasing intracellular Ca levels via cellular phosphodiesterase inhibition. Because it does not work on beta-receptors, it might be preferred for patients taking beta-blockers requiring inotropic support. It may cause peripheral vasodilation and hypotension, but this may be a benefit if pulmonary artery pressure is elevated as reductions in pulmonary artery pressure lead to improvements in right ventricular function. It has a long-half life and should be avoided in patients with renal impairment.
Dopamine: chemical precursor to norepinephrine and technically a vasopressor. At moderate doses (3-10 mcg/kg/min) it works on beta-receptors to increase myocyte contractility. At higher doses works primarily as a vasopressor, which may reduce cardiac output due to higher afterload.
Norepinephrine/epinephrine: has alpha and beta properties that lead to increased peripheral vasoconstriction, but also increases inotropy and chronotropy (faster heart rate)
Person presents with painless vision loss after seeing flashes of light. Ultrasound is below. What's the diagnosis?
Ventricular Arrhythmias Originating from the Moderator Band
- Ventricular arrhythmias originating from the moderator band (MB) often have a distinct morphology
- Typically MB arrhythmias have a left bundle branch block pattern, QRS with a late precordial transition (>V4), a rapid down stroke of the QRS in the precordial leads, and a left superior frontal plane axis
- MB arrhythmias are often associated with PVC-induced ventricular fibrillation
- Catheter ablation is quite effective at termination of the arrhythmias and facilitated with intracardiac echocardiography (ICE)
Back pain with radiculopathy can be very distressing to a patient and they have heard from their medically savvy neighbor that a MRI is the way to go. Now, armed with this knowledge, they are in your ED with earplugs in hand...
A few minutes of reassurance and education can save in both cost and ED throughput.
In one study researchers performed MRIs on asymtomatic adult patients.
Almost two-thirds (64%) had abnormal discs
Just over half (52%) had bulging discs
Almost a third (31%) had disc protrusions
Further, finding a bulging disc already suggested by your history and physical examination does not change management. The majority of these patients improve with conservative treatment within four to to six weeks.
Restrict ED MRI use for the evaluation of suspected cauda equina, epidural abscess and spinal cord compression.
There are numerous different causes of pediatric hemorrhagic diarrhea. Consider a pediatric patient with bloody diarrhea as being at risk for developing hemolytic uremic syndrome. Most cases of hemolytic uremic syndrome are caused by O157:H7 strains of E Coli that release Shiga-like toxin from the gut. Systemic release of the toxin causes microvascular thromboses in the renal microvasculature. The characteristic microangiopathic hemolysis results with anemia, thrombocytopenia and peripheral schistocytes seen on laboratory studies, in addition to acute renal failure.
Antibiotics have been controversial in the treatment of pediatric hemorrhagic diarrhea due to concern that they worsen toxin release from children infected with E Coli O157:H7 and thus increase the risk of developing hemolytic uremic syndrome. Numerous previous studies have provided conflicting data regarding the true risk (1). A recent prospective study showed antibiotic treatment increases the risk (2). Most recommendations warn against using antibiotics to treat pediatric hemorrhagic diarrhea unless the patient is septic.
Bottom line: Avoid treating pediatric hemorrhagic diarrhea with antibiotics
When you prescribe certain medications, it may require some further instructions to avoid ethanol or a disulfiram like reaction (nausea, vomiting, flushing) may occur. Keep this short list in your brain:
1) Particular cephalosporins: cefotetan is a the one more likely
2) Nitrofurantoin
3) Sulfonylureas: chlorpropamide and tolbutamide
4) Metronidazole
5) Trimethoprim-sulfamethoxazole
Jolt accentuation, the exacerbation of a headache with horizontal rotation of the neck, or shaking of the stretcher in the less cooperative patient, has been promoted for the past few years as the "go-to" test to assess for meningeal irritation in patients with headache. Previous studies have quoted sensitivities as high as 97.1%. (1)
A new prospective study in AJEM challenges this belief by looking at a total of 230 patients with headaches and subsequent LPs. 197 of them had the jolt accentuation test done, which had a sensitivity of only 21% for pleocytosis (defined as greater than or equal to 5 cells/high power field in the 4th CSF tube). Kernig's and Brudzinski's signs both did even more poorly, with a sensitivity of 2% each. (2)
What is a massive transfusion?
When would I use this?
Indications:
-Systolic Blood pressure < 100
-Unable to obtain blood pressure
AND
-Penetrating torso trauma
-Positive FAST
-External blood loss
-Plans to go to the OR
How do I give it?
Does this apply for just traumatic bleeding?
Are there other agents I can use?
What am I trying to do with this protocol?
16 yo M with pleuritic right upper chest pain that started today. He is suffering from an asthma exacerbation currently in the setting of URI with cough. He is afebrile, tachycardic to 140-150s, respiratory rate 20, and sats 98% on room air. ECG was performed which incidentally diagnosed this patient WPW and he went for ablation as an outpatient. His chest x-ray showed:
Besides a bad day, what do we call this chest x-ray finding?
Tendon Lacerations:
A reasonable approach to all tendon lacerations is to loosly reapproximate the wound and splint the hand in the position of function until the patient can be seen by a hand surgeon in the next 1-3 days. These injuries do not require immediate surgical repair, and with the high rate of complications it is probably best to discuss with your hand surgeon before attempting a repair.
The NEXUS criteria is widely applied to adults who present with neck pain due to trauma. While this study did include about 2000 pediatric patients, there were not enough young children to draw definitive conclusions. For more information on the evaluation of the cervical spine, see Dr. Rice's pearl from 9/7/12. A 2003 study piloted an algorithm for cervical spine clearance in children < 8 years.
Patients were spine immobilized if: unconscious, abnormal neurological exam, history of transient neurological symptoms, significant mechanism of injury, neck pain, focal neck tenderness or inability to assess based on distracting injury (extremity or facial fractures, open wound, thoracic injuries, or abdominal injuries), physical exam findings of neck trauma, unreliable exam due to substance abuse, significant trauma to the head or face, or inconsolable children.
When the 2 pathways (see attached) were implemented, there was a decrease in time to cervical spine clearance. There were no missed injuries in the study period prior to implementation of the pathway or once it was implemented. There was no significant difference in the amount of xrays, CT scans or MRIs.
Food poisoning can occur with many different food groups/items, as well as how the food is prepared, handled or stored.
There are three specific “food poisonings” associated with fish consumption can cause serious toxicity/illness beyond GI symptoms: Ciguatera, Scrombroid, tetrodotoxin (puffer fish)
Ciguatera
Symptoms:
May progress to develop…
Treatment: supportive care and mannitol in presence of severe neurologic symptoms (limited evidence).
Scrombroid
Symptoms:
Tx: H1/H2 blockers and supportive care
Serious reactions: treat like allergic/anaphylactic reaction
Tetrodotoxin
Symptoms:
Treatment: supportive care and intubated if needed.
While sitting on an international flight, ever wonder what your risks are for a blood clot?
General Background:
It is estimated that the risk for a deep venous thrombosis (DVT) is 3-12% on a long-haul flight. However, the real incidence is difficult to evaluate, due in part to the lack of consensus about 1) diagnostic tests, and 2) the appropriate time frame to relate a venous thromboembolic event (VTE) to travel.
Risks Factors for VTEs on long-haul flights:
Bottom Line:
Infectious Risks Associated with TTM
Football player complains of sudden foot pain after begin tackled. What’s the diagnosis?

Optimal Revascularization in Complex Coronary Artery Disease
- A multicenter trial 4,566 patients with NSTEMI, unstable angina, and multi-vessel coronary artery disease were enrolled comparing outcomes of cardiac stenting versus coronary artery bypass.
- Cardiac stenting was associated with improved outcomes and lower mortality in the following subgroups: age >65 years, women, unstable angina, TIMI score >4, and 2 vessel disease.
- Despite high clinical risk patients who underwent cardiac stenting compared to surgical revascularization did better in this prospective registry.
Back pain accounts for more than 2.6 million visits
30% of ED patients receive X-rays as part of their evaluation
Imaging can be avoided in a majority of these patients by focusing on high risk (red flags) findings in the history and physical exam.
Patients who can identify a an acute inciting event without direct trauma likely have a MSK source of pain.
Imaging rarely alters management
Attempt to avoid imaging in patients with nonspecific lower back pain of less than 6 weeks duration, with a normal neurologic exam and without high risk findings (fever, cancer, IVDA, bowel or bladder incontinence, age greater than 70, saddle anesthesia, etc)
Patients with radiculopathy (sciatica) and are otherwise similar to the above also do not require emergent imaging