Neurologic causes of cardiac arrest have not been well described. Two recent retrospective studies looked at the epidemiology and clinical features of these patients.
Hubner P. et al.
Arnaout M. et al.
Neurologic causes of cardiac arrest are uncommon presentations that may be difficult to distinguish from cardiac etiology of cardiac arrest. If history and clinical presentation suggests a neurologic cause, obtain a non-contrast head CT for evaluation.
The Role of the CVP in a Post- “7 Mares” Era
The role for using central venous pressure (CVP) as a measure of volume responsiveness has largely fallen out of favor over the years.1 There are certainly better indices for fluid responsiveness, but don’t be fooled – the CVP isn’t a one trick pony. In fact, a high or rapidly rising CVP should raise a significant concern for impending cardiovascular collapse.
Consider the following differential diagnosis in the patient with an abnormally high or rising CVP ( >10 cm H2O).
Bottom Line: In a time where the utility of the CVP has been largely dismissed, remember that an abnormal CVP offers great deal of information beyond a simple measure of volume status.
References
Follow me on Twitter: @JohnGreenwoodMD
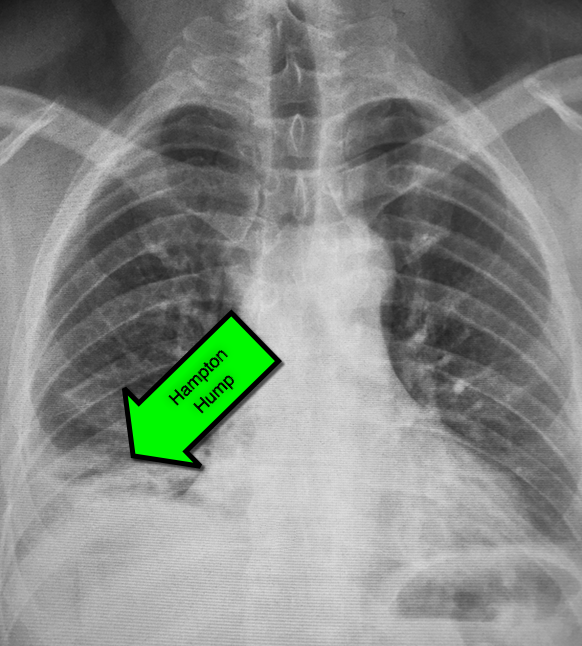
45 year-old male complains of pleuritic chest pain following a "long" flight. What's the diagnosis and what's this sign called?
This study is a case control study of the association of congenital heart disease (CHD) and stroke using a base population of 2.5 million Kaiser patients in California. 412 cases of stroke were identified and compared to 1236 controls. Of these stroke patients, 11/216 ischemic strokes and 4/196 hemorrhagic strokes were attributed to CHD (both cyanotic and acyanotic lesions). CHD was found in 7/1236 controls.
Children with CHD and history of cardiac surgery had the strongest risk of stroke (31 fold over the control group). Many of these children had strokes years after their surgery. Children with CHD who did not have cardiac surgery had a trend towards elevated stroke risk, but the confidence intervals included the null. More children without CHD history presented with headache.
Bottom line: Stroke risk (both hemorrhagic and ischemic) extend past the immediate postoperative period in patients with CHD.
The Centers for Disease Control continues to report increased numbers of measles patients in the US. From January 1 to February 13, 2015 there have been 141 cases. It has spread to 17 states and the District of Columbia, with 80% linked to the multistate outbreak from Disneyland.
Measles is not a benign disease!
Per the World Health Organization, there were 146,700 measles deaths globally in 2013. Most of these deaths occur in lower- and middle-income countries,
Even in the US, measles can cause serious complications and death. Complications from measles can be seen in any age group, but particularly in children <5 years of age and in adults >20 years of age.
Measles Complications:
Common:
Severe:
Long-term:
Bottom Line:
Per Dr. Anne Schuchat of the CDC: “This is not a problem with the measles vaccine not working. This is a problem of the measles vaccine not being used.”
As the cold and snow rips through the United States, hypothermia is a major concern because each year approximately 1,300 Americans die of hypothermia.
Classification of hypothermia:
The risk of cardiac arrest increases when the core temperature is less than 32 Celsius and significantly rises when the temperature is less than 28 Celsius. Rapid rewarming is required as part of resuscitation should cardiac arrest occur.
A rescue therapy to consider (when available) is extra corporeal membrane oxygenation (ECMO). ECMO not only provides circulatory support for patients in cardiac arrest, but allows re-warming of patients by 8-12 Celsius per hour.
Some studies quote survival rates of 50% with hypothermic cardiac arrest patients receiving ECMO versus 10% in similar patients who do not receive ECMO.
As winter lingers in the United States, consider speaking to your cardiac surgeons now to plan an Emergency Department protocol for hypothermic patients that may require ECMO.

The Unforgotten: ECG Utilization to Differentiate Athletic Heart vs. Brugada
- Highly trained athletes develop ECG changes as a physiologic consequence of increased vagal tone; The ECG manifestations of early repolarization (ER) can range from simple J–point elevation to anterior (V1 to V3) "domed" ST-segment elevation and negative T wave.
- The former raises problems of differential some forms of ER with the “ coved-type” pattern seen in Brugada Syndrome (BS).
- A recent study compared the ECG tracings of 61 athletes w/a “domed” ST-segment elevation & negative T wave and 92 age/sex-matched BS patients w/a “ coved-type” pattern to identify an ECG criteria for distinguishing benign athletic changes seen in ER from BS.
- ECG analysis focused on ST-segment elevation at J-point (STJ ) and at 80 milliseconds after J-point (ST80 ).
- Athletes had a lower maximum amplitude of STJ (p < 0.001) & lower STJ /ST80 (p < 0.001)
- All patients (100%) with BS showed a downsloping ST-segment configuration (STJ/ST80 > 1) versus only 2 (3%) athletes (p < 0.001)
- An upsloping ST-segment configuration (STJ /ST80 < 1) showed a sensitivity of 97%, a specificity of 100%, and a diagnostic accuracy of 98.7% for the diagnosis of ER.
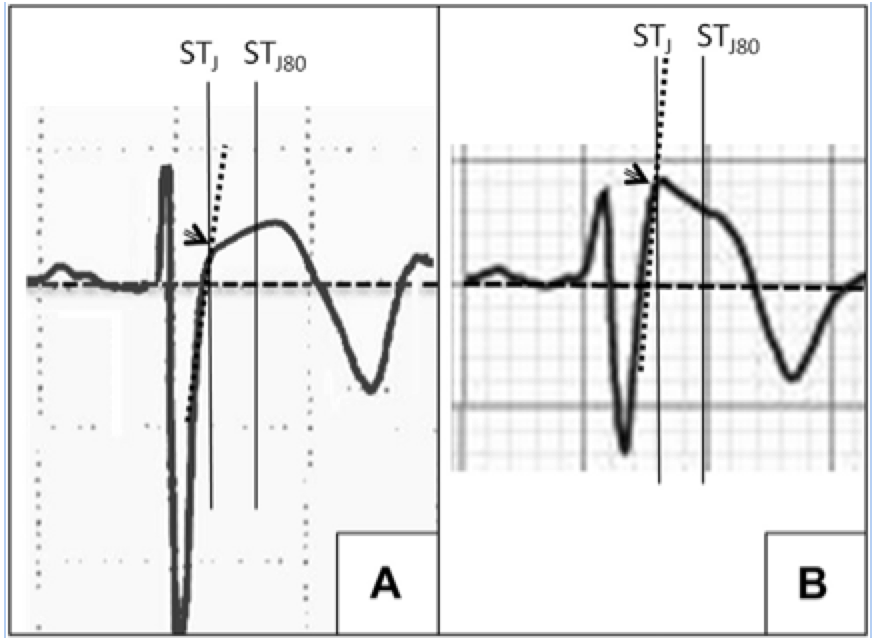
A: ER
B: Brugada
LATERAL ANKLE TENDINOPATHY
Hx: subacute onset (weeks) of the pain seen in athletes esp. runners (banked or uneven surfaces).
PE: Tenderness to palpation posterior to the lateral malleolus or over the course of the tendon. Pain worse with resisted ankle eversion from a dorsiflexed postion. Examine for subluxation of tendon.
The diagnosis is made from the above and does not require imaging.
Tx: Rest, conservative care, physical therapy (eccentric exercise focus), ankle taping or lace up brace. Severe cases may even require a walking boot.
http://www.epainassist.com/images/Article-Images/Peroneal_Tendonitis.jpg
Pediatric Caffeine Overdose
As the in-service draws closer and the hours to study wind down, I find myself becoming more and more of a caffeine enthusiast. While a No-Doz or Diet Mt. Dew may put a little more pep in my step, the caffeine found in energy drinks, caffeine pills, and diet supplements can quickly result in an dangerous overdose in a young child.
Caffeine Overdose Presentation- Sympathomimetic Toxidrome
Available Sources of Caffeine-
Toxic Doses
Management- treat the symptoms (metabolic, cardiovascular, and neurologic)
Good Luck on the In-Service!

A new review summarized published adverse effects when IV lipid emulsion is used along with venous-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiotoxic drug poisoning.
Not surprisingly, running fat through the ECMO circuit can cause some issues. Here's what's been published:
It's unclear how these findings should change management if using both treatment modalities, but at the very least, be aware that fat depostion in the VA-ECMO circuits and increased blood clot formation can occur.
Magnesium, another failed neuroprotectant?
Stroke is a leading cause of adult disability and the second leading cause of death worldwide. Currently available therapies for acute ischemic stroke are based on restoring perfusion to the ischemic penumbra. However, they are only moderately effective.
A series of pathological cascades leading to neuronal death are triggered in acute ischemia. Thus it may be logical to suggest that if one can interrupt the propagation of these cascades, perhaps part of the brain tissue can be protected and salvaged.
Magnesium has been shown in various animal models to have pluripotent neuroprotective properties. It is also widely available, simple to administer, and has a favorable risk profile. A prior study of magnesium in acute ischemic stroke (IMAGES) did not show a benefit when the agent was administered a median 7.4 hours after symptom onset. However, a subgroup of patients treated within 3 hours of symptom onset showed possible benefit.
The Field Administration of Stroke Therapy - Magnesium (FAST-MAG) trial, funded by the NIH, looked at magnesium administered within 2 hours after symptom onset on the degree of disability at 90 days after stroke as measured by the modified Rankin scale.
Magnesium was not found to have any benefit in functional outcome at 90 days.
This study was unique in several ways:
However, despite this study being very well executed, demonstrating the feasibility of conducting a phase 3 trial with targeted intervention within the hyperacute window, it is another neuroprotective agent that failed to translate from the laboratory bench to the clinical realm.
Potential explanations for the discrepancies between preclinical and clinical outcomes of neuroprotective agents thus far include discrepancies on outcome measures, functional assessments, pre-morbid conditions, therapeutic windows, and drug-dosing schedules between animal studies and clinical trials.
Take Home Point: Magnesium does not have any clear benefit in acute ischemic stroke at this time.
Updates in preventative strategies in the ICU
Preventing Ventilator Associated Pneumonia (VAP)
The trial
Bottom Line
Daily bathing with chlorhexidine does not reduce health care associated infections
The trial
Bottom Line
We know vancomycin should be dosed based on weight rather than the default 1 gm dose so many patients receive. A past Academic Life in EM post explores the nuances of proper vancomycin dosing. But do higher loading doses in the ED actually lead to more therapeutic trough levels?
New Data
A new randomized trial compared ED patients receiving 30 mg/kg initial doses vs. 15 mg/kg. [1] There was a significantly greater proportion of patients reaching target trough levels of 15 mg/L at 12 hours among the patients who received a 30 mg/kg loading dose as compared with a traditional 15 mg/kg dose (34% vs 3%, P < 0.01). This study did not use a max dose of 2 gm. They included patients up to 120 kg who received 3.6 gm loading doses! Patients with creatinine clearance < 50 mL/min were excluded. There was no difference in incidence of nephrotoxicity between the groups.
Application to Clinical Practice
| Performance Characteristics of Common Drug Abuse Screening Immunoassays | ||
| Drug/Class | Detection Interval (***) | Comments |
| Amphetamines | 1-2 days (2-4 days) | Decongestants, ephedrine,l-methamphetamine, selegilene & bupropion metabolites may give False (+) results; MDA & MDMA are variably detected |
| Barbiturates | 2-4 days | Phenobarbital may be detected for up to 4 weeks |
| Benzodiazepines | 1-30 days | Benzos vary in reactivityand potency; False (+) results may be seen with oxaprozin |
| Cannabinoids | 1-3 days (>1 month) | Screening assays detect inactive and active cannabinoids; Confirmatory assays detects inactive metabolite THCA (tetrahydrocannabinoic acid) |
| Cocaine | 2 days (1 week) | Screening & confirmatory assays detect inactive metabolite BE (benzoylecgonine); False (+) results are unlikely |
| Opiates | 1-2 days; 2-4 days (<1 week) | Semisynthetic opiates derived from morphine show variable cross-reactivity; Fully synthetic opioids (e.g., fentanyl, meperidine, methadone, propoxyphene, tramadol) have minimal cross reactivity; Quinolone may cross-react |
| Methadone | 1-4 days | Doxylamine may cross-react |
| Phencyclidine | 4-7 days (>1 month) | Dextromethorphan, diphenhydramine, ketamine, & venlafaxine may cross react |
| Propoxyphene | 3-10 days | Duration of positivity depends on cross reactivity of metabolite norpropoxyphene |
(***)Values are after typical use; values in parentheses are after heavy or prolonged use.
From January 1st to January 30th, 2015, 102 people from 14 states were reported to have measles. This one month total is greater than the annual number of U.S. cases from 2002 to 2012. Most of these cases are related to a large outbreak from a Californian amusement park. Measles can spread in communities without adequate vaccination (low herd immunity). The majority of the people in the US who get measles are unvaccinated. However, measles remains common in many parts of the world.
Bottom Line:
As noted in the recent ACEP Fact Sheet, “A very high index of suspicion for Rubeola is necessary especially among patients with an exposure history, travel to foreign or domestic areas where disease is present, and those without adequate immunization. Immediate isolation of these patients should be considered in the ED or other outpatient healthcare setting.”
Hypertensive Emergency Pearls
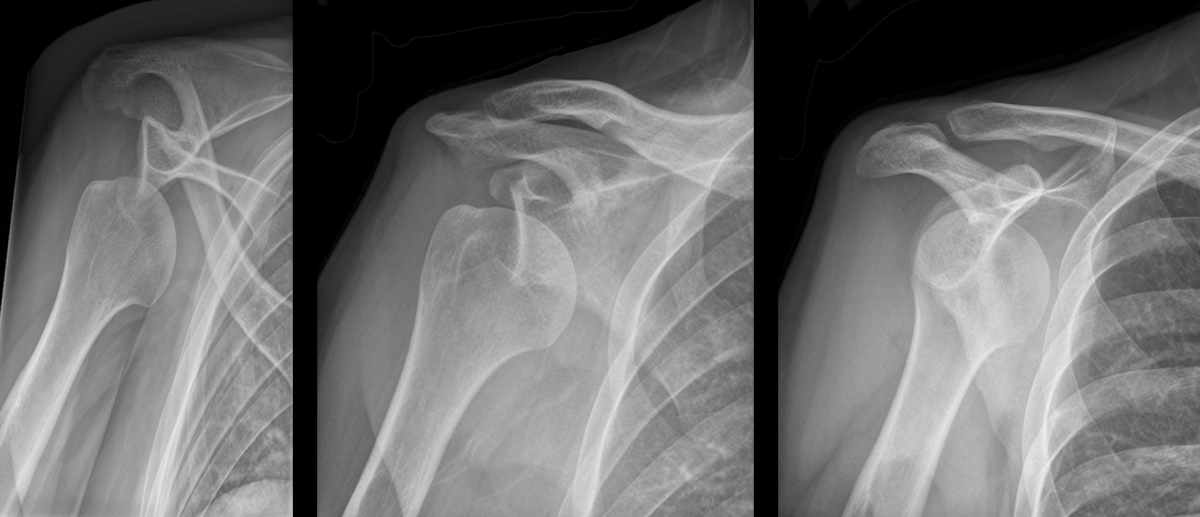
Patient presents with right shoulder pain following minor trauma. What's the diagnosis....and what's the Cunningham technique?
Tetrodotoxin is lethal poison that blocks sodium channels. A famous sushi called "Fugu" is cut from a puffer fish that contains this poison. The idea is to get just enough of the toxin to cause peri-oral paresthesia but not too much to get seizures, paralysis and cardiac dysrrhythmias. A recent outbreak in Minneapolis, Minnesota was just reported in the MMWR so it can really happen anywhere, its a great read - dried puffer was bought from a market in NYC.
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6351a2.htm
2-3 mg of the toxin is lethal to an adult human. No antidote exists though I would try hypertonic sodium bicarbonate for the cardiac dysrrhythmias and appropraite supportive. If the patient survives 24 hrs, the patient will do well without sequelae if appropriately supported.
Patients with myasthenia gravis (MG) may be seen in the emergency department for symptoms that are not related to their MG, such as an upper respiratory tract infection or chest pain, for example.
The emergency physician should be careful in prescribing new medications to patients with MG, as that can precipitate a myasthenic crisis (and therefore cause significant morbidity and mortality). Below is a list of medications that are commonly implicated; an extensive list can be found on www.myasthenia.org/docs/MGFA_medicationsandmg.pdf)