Poison ivy, oak, and sumac (Toxicodendron sp) causes a highly puritic, allergic contact dermatitits (ACD) that affects between 10 and 50 million in the US every year. It is a significant occupational hazard as well a scourge for outdoor enthusiasts.
Toxicodendron species contain oleoresins, known as Urushiol compound, secreted by all parts of the plant. Contact with the oil usually occurs by brushing against or direct handling of the plant or contaminated items. This toxin triggers a type IV delayed hypersensitivity reaction in approximately 75% of the population. Within 12-24 hours an erythematous, often linear, vesicular rash develops but new lesions can occur up to 2 weeks later.
There is no ideal treatment for ACD induced by Toxicodendron species. Avoidance and barrier protection are the best strategies. Recommended medications include antihistamines, topical preparations, and systemic steroids. However, steroids require a 2-3 week course to prevent recrudescence of the rash and are not without undesirable side affects.
Zanfel, an OTC granular polyethlene paste, removes urushiol by binding with it to create an aggregate cluster that can be washed away with water. It is highly effective, providing rapid relief even as a sole agent but requires multiple initial applications and is expensive. Mean Green hand scrub has similar ingredients and is claimed to bond urushiol also. Excessive scrathing and abrasive scrubs can cause secondary cellulitis requiring antibiotics.
Introduction
Obtaining quality information about emergency care in low- and middle-income countries (LMIC) is challenging. Data is sparse and often of low quality and the number of peer reviewed publications is limited.
In order to address this, Obermeyer et. al. just published in the WHO Bulletin a systematic review of emergency care in 59 low- and middle-income countries. In this article, the authors systematically reviewed 195 reports related to 192 facilities. The search included English or French articles from 1990 found within PubMed, CINAHL and World Health Organization (WHO) databases.
Burden of Emergency Care
Most articles were from emeregncy departments (EDs) in academically-affiliated hospitals in urban areas. Median mortality in the EDs was 1.8% (interquartile range, IQR: 0.2–5.1%), though in sub-Saharan Africa it was 3.4% (IQR: 0.5–6.3%). The median number of patients seen per year was 30,000 (IQR: 10 296–60 000). The facilities were staffed primarily by physicians-in-training or by physicians whose level of training was unspecified. There were very few providers specialized in emergency care.
Bottom Line
Based upon available data, there are high patient loads and mortality in LMIC- particularly in sub-Saharan Africa. This report highlights the importance of emergency care and the opportunity for systematic improvement to reduce mortality in these countries.
Ever forget all the things that make up MUDPILES in your AG acidosis differential?
Instead, consider the less-complicated mnemonic "KILR"!
K Ketoacidosis (diabetic, alcoholic, starvation)
I Ingestion (salicylate, acetaminophen, methanol, ethylene glycol, CO, CN, iron, INH)
L Lactic acidosis (infection, hemorrhage, hypoperfusion, alcohol, metformin)
R Renal (uremia)
Once you rule out the KLR causes, begin to consider ingestion or a tox source as your source. Remember that many of the listed ingestions can also cause a lactic acidosis.
How much does the blood glucose concentration increase when dextrose 50% (D50) is administered?
A new study found a median increase of 4 mg/dL (0.2 mmol/L) per gram of D50 administered.
This retrospective study was conducted in critically ill patients who experienced hypoglycemia while receiving an insulin infusion. While it may not directly apply to all Emergency Department patients, an estimation of the expected blood glucose increase from rescue dextrose is helpful. If the blood glucose doesn't respond as anticipated, it can help us troubleshoot possible issues (eg, line access).
Oral hypoglycemic agents (e.g. sulfonylureas) can cause symptomatic hypoglycemia. Unlike metformin, sulfonylureas stimulate the release of insulin from beta-cells (in pancreas) in response to serum glucose level.
ED management of hypoglycemia involves:
However, for recurrent hypoglycemia (> 3 episodes of hypoglycemia), think about octreotide, rather than starting a dextrose (D5) infusion.
For example, D5 infusion at 150 mL/hour has only 7.5 gm of dextrose (calculation: D5% = 5gm/100 mL). One gram of dextrose contains about 4 calories (equivalent to one piece of Skittles) So, with a D5 infusion at 150 mL/hour, you are giving your patients 8 pieces of Skittles per hour. A bottle of Snapple lemon ice tea (non-diet) has more calories (150 calories in 16 oz. or 473 mL)!
Octreotide 50 mcg SQ (q6 hour) injection will decrease the insulin release from the beta-cell by blocking the voltage-gated Ca channel on the beta-cell.
All patient who received octreotide in the ED requires admission to the hospital for observation. Patients can be safely discharge from the hospital when finger stick glucose level remains normal for 24 hours after the last dose of octreotide.
Bottom line: In sulfonylrea-induced recurrent hypoglycemia, administer octreotide, rather than continuous infusion of dextrose (D5) solution.
Every wonder what are the major global killers? Per the World Health Organization, the following were the top 20 causes.
Not unexpected, diseases primarily of the elderly, such ischemic heart disease, stroke and chronic obstructive pulmonary disease are on the top of the list. However, there are others, such as road traffic injuries and HIV/AIDS that could impact anyone.
| Top 20 Causes of Global Mortality, 2012 | ||||
| Rank | Cause | Deaths (000s) | % deaths | Deaths per 100,000 population |
| 0 | All Causes | 55859 | 100.0 | 789.5 |
| 1 | Ischaemic heart disease | 7356 | 13.2 | 104.0 |
| 2 | Stroke | 6671 | 11.9 | 94.3 |
| 3 | Chronic obstructive pulmonary disease | 3104 | 5.6 | 43.9 |
| 4 | Lower respiratory infections | 3052 | 5.5 | 43.1 |
| 5 | Trachea, bronchus, lung cancers | 1600 | 2.9 | 22.6 |
| 6 | HIV/AIDS | 1534 | 2.8 | 21.7 |
| 7 | Diarrhoeal diseases | 1498 | 2.7 | 21.2 |
| 8 | Diabetes mellitus | 1497 | 2.7 | 21.2 |
| 9 | Road injury | 1255 | 2.3 | 17.7 |
| 10 | Hypertensive heart disease | 1141 | 2.0 | 16.1 |
| 11 | Preterm birth complications | 1135 | 2.0 | 16.0 |
| 12 | Cirrhosis of the liver | 1021 | 1.8 | 14.4 |
| 13 | Tuberculosis | 935 | 1.7 | 13.2 |
| 14 | Kidney diseases | 864 | 1.6 | 12.2 |
| 15 | Self-harm | 804 | 1.4 | 11.4 |
| 16 | Birth asphyxia and birth trauma | 744 | 1.3 | 10.5 |
| 17 | Liver cancer | 740 | 1.3 | 10.5 |
| 18 | Stomach cancer | 733 | 1.3 | 10.4 |
| 19 | Colon and rectum cancers | 724 | 1.3 | 10.2 |
| 20 | Alzheimer's disease and other dementias | 701 | 1.3 | 9.9 |
It's July, that means new doctors are learning to do central-lines...here's a quick video with some quick pearls on how to do that. Enjoy!
Triquetral fractures are the 2nd most common carpal fractures (scaphoid).
Dorsal surface most commonly.
Usually occur from impingement from the ulnar styloid, shear injury or from ligamentous avulsion.
XR: best seen on the lateral projection
http://images.radiopaedia.org/images/902179/42b3487baf4fb66183c51cd982477d_big_gallery.jpg
Remember this injury/radiographic appearance the next time you see an avulsion fracture dorsal to the proximal row of carpal bones on the lateral film but are unsure of the donor site.
Post- streptococcal glomerulonephritis (PSGN) is an inflammatory reaction of the kidneys following infection with group A strep, and can occur sub clinically or have a severe presentation requiring admission, Nephrology consult, and careful management.
This diagnosis should be considered in any child between ages 2-12, or adults over 60, presenting with sudden unexplained hematuria or brown urine. Patients may also present with generalized edema secondary to urinary protein loss, hypertension, and acute kidney injury. Since kidney involvement usually trails the throat injection by 2-3 weeks or more, the patient and their family may not relate the two symptoms. A previous or current diagnosis of strep throat is not necessary to consider a patient for PSGN, since they may test negative by throat culture at the time of urinary and renal symptoms
When considering this diagnosis, the EM physician should order the following lab tests:
- Urinalysis (for casts and protein)
- Creatinine
- ASO Titer (or full streptozyme assay of 5 tests including ASO)
- Complement C3, C4, C50
Treatment is primarily supportive, and many cases will be mild enough to discharge home with pediatrician or Nephrology follow up. However, some cases may warrant admission for AKI, pulmonary edema, or cerebral edema. Edema can be managed with sodium restriction and loop diuretics. Hypertension can be managed with anti hypertension medications.
Renal biopsy can confirm the diagnosis with the presence of epithelial crescents in the glomeruli, but this is only necessary in severe cases where it is important to determine the etiology of the nephritis.
Given the similarity in pathophysiology, pharmacologic treatments for ischemic stroke have been modeled after those for acute myocardial infarction, such as the use of antiplatelets and thrombolytic agents. Have you ever wondered, why don't we give glycoprotein IIb/IIIa inhibitors (GPIs) as well?
A Cochrane review answers this question; GPIs increase morbidity in acute ischemic stroke (in the form of intracranial hemorrhage), with no evidence of benefit (improvement in Rankin Scale).
The systematic review looked at randomized clinical trials of GPIs in patients with ischemic stroke of 6 hours or less, alone or in combination with thrombolytics.
Care of Drowning Patients in the ED
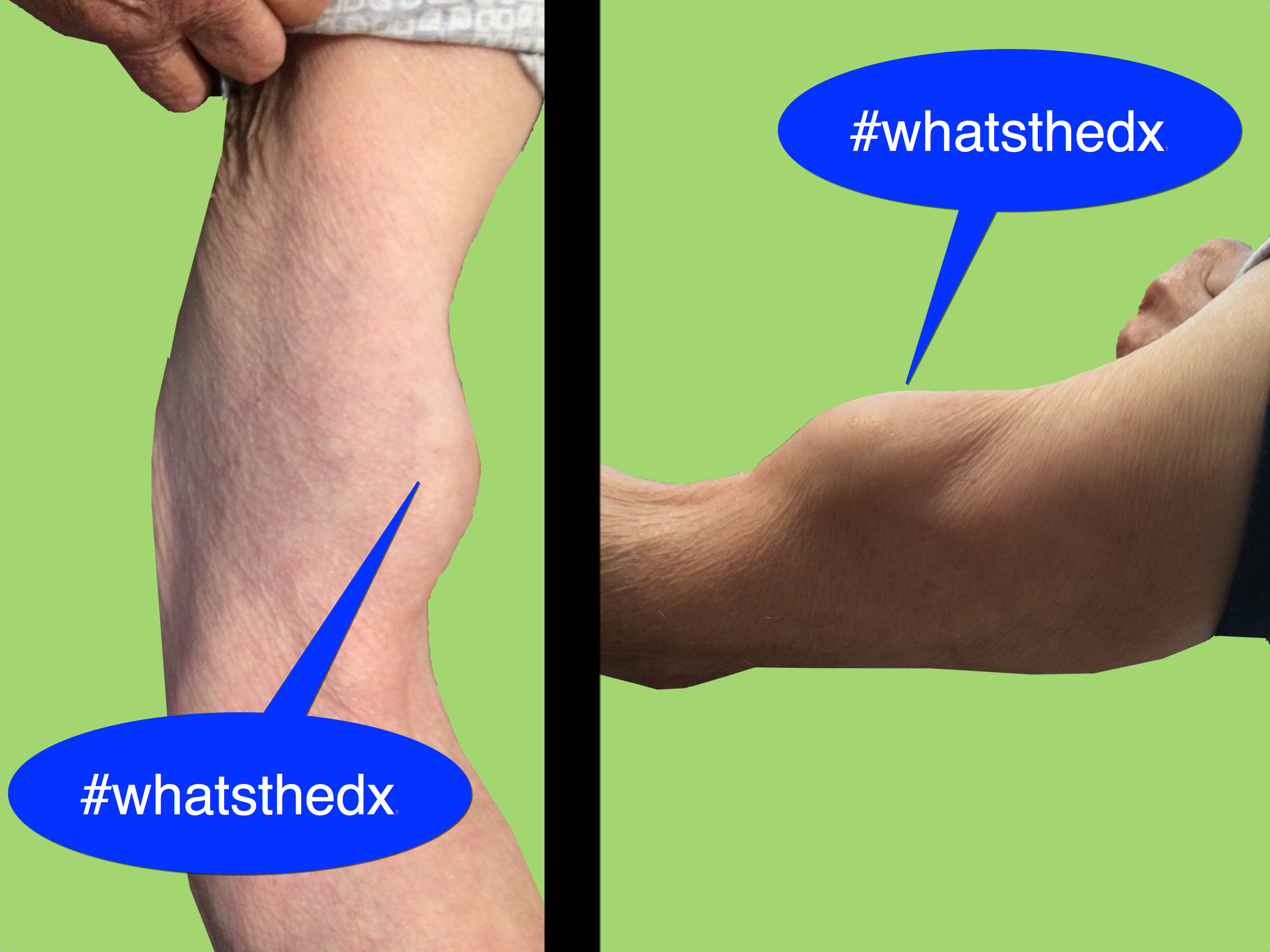
81 year-old man was mowing the lawn and then felt a sudden pop, then pain in his left arm. What's the diagnosis and what's this sign called?
Opiates Causing Cardiac Toxicity
- Opiates are well known in their ability to cause sedation, euphoria, and respiratory depression, however are classically considered devoid of cardiac properties.
- Methadone a synthetic central-acting μ-opioid receptor agonist has been associated with dose-dependent QTc interval prolongation and torsade de pointes (TdP).
- Utilization of other less known drugs of abuse, specifically loperamide (peripherally acting μ-opioid receptor agonist) has been increasing in popularity.
- A surge in recent case reports has shown a potential causal association of loperamide with prolongation of the QTc interval and subsequent TdP.
- Toxic ingestion of loperamide leading to TdP has been successfully managed with standard TdP therapies (magnesium, isoproterenol, and pacing).
Compartment Syndrome
Compartment syndrome is a diagnosis that needs to be made quickly in order to prevent long term muscle, nerve, and vascular compromise.
Two pieces of information are needed to determine if the patient has compartment syndrome.
Diastolic Pressure - Compartment pressure < 30 makes the diagnosis of compartment syndrome
So if a diastolic blood pressure is 80 and the compartment pressure is 40 the difference is 40 mmHg and the patient likely does not need a fasciotomy. The diagnosis can only be 100% onfirmed by a trip to the OR so these values should still be discussed with your local orthopaedist. When calling them just make sure you know both the DBP and the compartment pressure so that it can be interpreted correctly.
Physostigmine is a cholinergic agent (acetylcholine esterase inhibitor) that can be used to reverse anticholinergic toxicity. Its use has been declining since the publication of several case reports of physostigmine induced cardiac arrest in tricyclic antidepressant (TCA) overdose.
The first case report (and often cited) was by Pental P. et al. (Ann Emerg Med 1980), who presented 2 cases (32 and 25 year old) of asystole after administration of physostigmine (2 mg) in severe TCA overdose. These two cases both had widened QRS interval (120, 240 msec) due to TCA poisoning. Bradycardia preceded the asystole.
The second case report (Shannon M Pediatr Emerg Care 1998) reported a 15 year-old girl with QRS widening (120 msec) received 2 mg of physostigmine and developed severe bradycardia and then asystole.
Another case series (Knudson K et al. BMJ 1984) of 41 patients with overdose of maprotiline showed that physostigmine administration was associated with higher incidence of seizures. No asystole was noted.
Today physostigmine is contraindicated in TCA poisoning. But if we think about it, physostigmine administration probably wasn’t a good idea in the first place. Correcting anticholinergic toxicity of TCA has limited benefit; mortality from TCA overdose is usually associated with cardiac toxicity (Na-channel blockade) and should be treated with NaHCO3 administration
Physostigmine still has a role in treating isolated anticholinergic toxicity (e.g. diphenhydramine, benztropine, dimenhydrinate, scopolamine, jimson weed overdose). Prior to physostigmine administration:
Bottom line: If you suspect isolated anticholinergic toxicity, think about physostigmine. Like any medication, risk and benefit of administration should be considered prior to administration.
Tuberculosis (TB) remains a deadly scourge killing approximately 1.5 million each year (see Pearl from 7/2/2105). Recognition by astute clinicians in the emergency department is key, as there is no readily available rapid test.
Current testing options:
1) Tuberculin skin test (also known as the Mantoux tuberculin skin test). A small amount of fluid (tuberculin purified protein derivative) is placed intradermally, usually in the left forearm. A positive test means the person was infected with TB. (Alternatively, if they grew up outside the US, they could have been vaccinated with Bacillus Calmette–Guérin or BCG.) A positive test is determined by the size of the reaction, but this can vary depending on the patient’s immune status.
2) Two interferon-gamma release assays or IGRA blood tests are approved for TB. While not readily available in all institutions, this is the preferred method for someone vaccinated with BCG.
Diagnosis of TB disease is based upon:
Treatment:
TB treatment depends on the susceptibility of the organism and the immune status of the patient. For a susceptible organism in a non-HIV patient, the first-line anti-TB agents regimens include
Typical treatment has an initial phase of 2 months, followed by a choice of several options for the continuation phase of either 4 or 7 months. Further information can be found at the CDC website on tuberculosis
Bottom Line
As stated previously, in the emergency department, maintain a strong clinical awareness for tuberculosis for someone with night sweats, cough, chest pain, and intermittent fever lasting for 3 weeks or longer. In particular, consider this diagnosis for someone from a low- or middle-income country or if he or she is HIV positive.
Blood Pressure Management in Severe Preeclampsia
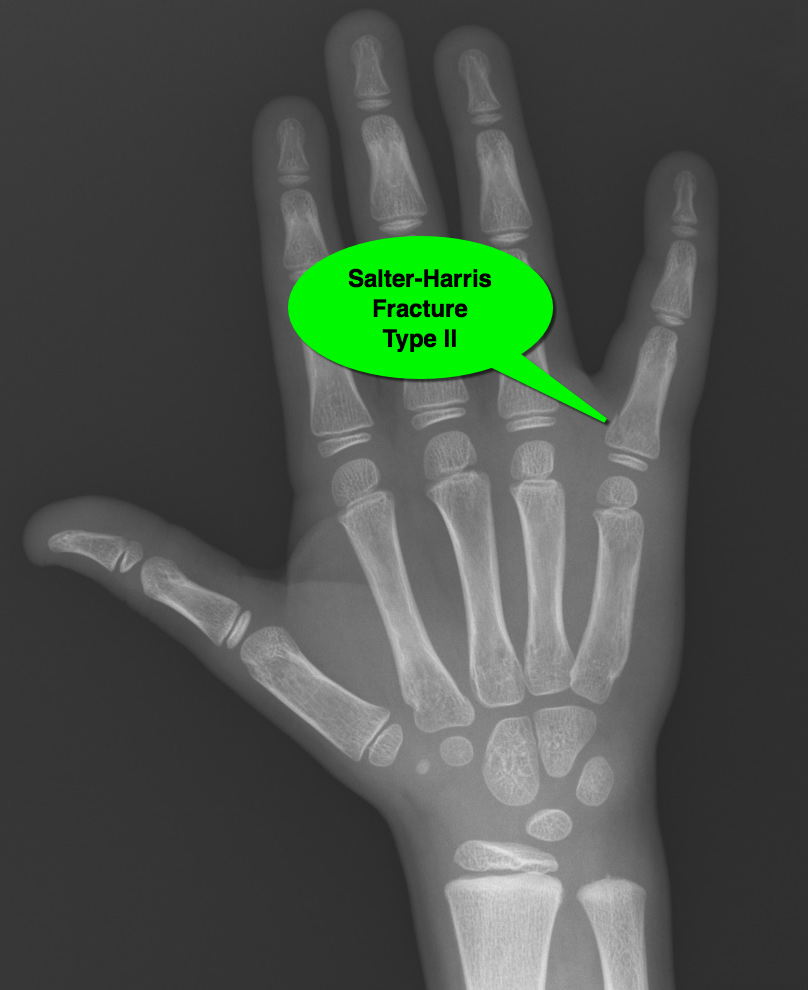
7 year-old male "jammed" 5th finger while playing basketball with pain and swelling over finger. What's the diagnosis?

A sports hernia is a painful musculotendinous injury to the medial inguinal floor.
It is the result of repetitive eccentric overload to the abdominal wall stabilizers of the pelvis.
It is common in sports that require sudden changes of direction or intense twisting movements.
Despite the term "hernia" in the title, it is not a true hernia as there is no "herniation" of abdominal contents
http://www.ssorkc.com/wp-content/uploads/2014/09/publagia.gif
Figure description: The upward and oblique pull of the abdominal muscles on the pubis fights against the downward and lateral pull of the adductors on the inferior pubis. This imbalance of forces can lead to injury.
PE: Evaluation of other GU/GYN/other intra-abdominal pathology comes first.
Clinician may note tenderness of the pubic ramus and medial inguinal floor.
Pain is more severe with resisted hip adduction and with resisted sit-up.
Combining these maneuvers (resisted situp while adducting hips) recreates the pathophysiology described above and is a good exam maneuver.
{kind=link}