An interesting new study was published looking at in-hospital mortality in TBI patients who received succinylcholine or rocuronium for RSI in the ED.
What They Did
What They Found
Application to Clinical Practice
Throughout medical history one of the basic tenets of poisoning therapy is to remove the poison from the patient. For hundreds of years, gastric decontamination has been the cornerstone treatment for acute poisonings by ingestion. This commonsense approach endeavors to remove as much of the the ingested toxin as possible before systemic absorption and organ toxicity occurs. Multiple GI decontamination methods have been utilized including gastric emptying by lavage and ipecac, toxin binding by activated charcoal, and increasing GI transit time with cathartics and bowel irrigation. Numerous studies have been conducted to assess the effectiveness of GI decontamination including measurement of amount of toxin removed by gastric retrieval, reduction of bioavailability by measuring blood levels, and finally comparison of clinical outcomes of patients treated with and without GI decontamination. Controlled studies have failed to show conclusive evidence of benefit and have even demonstrated resultant harm especially with use of gastric lavage. Activated charcoal has a tremendous surface area capable of binding many substances. Although viewed as relatively safe it does have risks in certain subsets of patients, pulmonary aspiration the most common, and is no longer routinely recommended.
Considerations for use of Activated charcoal (AC) use in acutely poisoned patients:
The decision to use activated charcoal is no longer standard of care but should be individualized to each clinical situation weighing the risk versus clinical benefits.
On February 1st, the World Health Organization declared that Zika was an international public health emergency. As noted in the Pearl from January 20th, 2016, Zika is a mosquito-borne RNA flavivirus that is usually asymptomatic. However, congenital malformations have been seen in pregnant women infected with Zika.
While it is clear that the decision to declare an international public health is a judgement call, what are the criteria for considering this declaration?
Per the WHO, the term Public Health Emergency of International Concern is defined in the IHR (2005) as “an extraordinary event which is determined, as provided in these Regulations:
· to constitute a public health risk to other States through the international spread of disease; and
· to potentially require a coordinated international response”. This definition implies a situation that: is serious, unusual or unexpected; carries implications for public health beyond the affected State’s national border; and may require immediate international action.
The responsibility of determining whether an event is within this category lies with the WHO Director-General and requires the convening of a committee of experts – the IHR Emergency Committee.
For Zika, the sequalae of concern are the clusters of microcephaly and Guillain-Barré syndrome suspected to have resulted from Zika infection.
Diverticulitis
It seems like the standard treatment course for patients with suspected diverticulitis in the ED is to obtain a CT of the Abdomen and pelvis and then to start antibiotics. A CT scan is really only needed if you suspect that they have an abscess, micro perforation, are not responding to conventional treatment, or you suspect an alternative diagnosis.
However, what should the conventional treatment be? Several recent studies from Sweden, Iceland and the Netherlands have shown that patients treated with antibiotics did not fair any better then patients who were just observed. There was no difference in time to resolution of symptoms, complications, recurrence rate, or duration of hospitalization.
Several national societies (Dutch, Danish, German, and Italian) now recommend withholding antibiotics in patients free of risk factors who have uncomplicated disease, but these patients will need close follow up.
TAKE HOME POINT: Patients with diverticulitis can be treated supportively and probably do not require antibiotics unless you suspect they have complicated disease or are immunosuppressed.
Airway management is an integral part of caring of critically ill patients, but is there anything that should be done differently in the neurologically injured patient?
Shock Index
Recommended follow-up for common orthopedic injuries
Lead is a ubiquitous metal in the environment partly due to decades of using leaded gasoline (organic lead) and lead-based paint (inorganic lead). Outside of occupational exposure, children are disproportionately affected from environmental lead exposure.
Common route of exposure are:
Majority of the absorbed lead are stored in bone (years) > soft tissue (months) > blood (30-40 days) (half-life). Thus blood lead level does not accurately reflect the true body lead burden.
Incidence of elevated blood lead level (EBLL > 5 microgram/dL) in children increased from 2.9 to 4.9% in Flint, MI before and after water source change. In the area with the highest water lead level, the incidence increased by 6.6%.
Clinical manifestation in children
| Clinical severity | Typical blood lead level (microgm/dL) |
| Severe
| > 70 – 100 |
| Mild to moderate
| 50 – 70 |
| Asymptomatic
| > 10 |
Evaluation for lead poisoning
Management of children with EBLL
Zika virus is a mosquito-borne flavivirus.
While outbreaks have been previously reported in Africa, Asia and the islands of the Pacific, it was first reported in the Western Hemisphere in May 2015.
Clinical Disease:
Diagnosis and Treatment
Prevention
What classifies "submassive PE"?
Submassive PE has early benefit from systemic thrombolysis at the cost of increased bleeding [1].
Ultrasound-accelerated, catheter-directed thrombolysis (USAT) [the EKOS catheters] has been shown to be safe, with low mortality and bleeding risk, as well as immediately improved RV dilation and clot burden [2-4]. USAT may improve pulmonary hypertension [4].
USAT is superior to heparin/anti-coagulation alone for submassive PE at reversing RV dilation at 24 hours without increased bleeding risk [5].
Long-term studies evaluating chronic thromboembolic pulmonary hypertension (CTEPH) need to be done, comparing USAT with systemic thrombolysis and surgical thombectomy.
Take-home: In patients with submassive PE, USAT should be considered over systemic thombolysis or anti-coagulation alone.
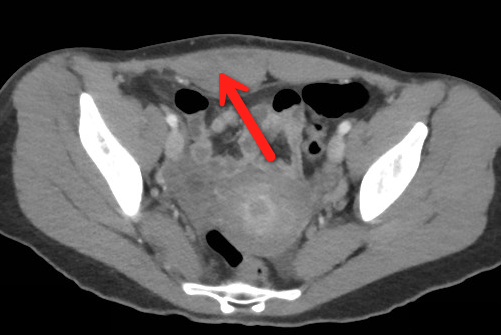
23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" exercise. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)

The Salter Harris Classification System is used in pediatric epiphyseal fractures. The higher the type of fracture the greater the risk of complications and growth disturbance.
Some common exam facts about Salter Harris Fractures are:
The Classification system as listed by Type:
For Maite, a helpful mnemonic is SALTR , Slipped (Type I), Above (Type II), Lower (Type III), Through (Type IV), and Ruined or Rammed (Type V)
A image of the fractures can be found on FP Notebook at http://www.fpnotebook.com/ortho/fracture/ephyslfrctr.htm
ED study of 60 pediatric patients for procedural sedation
Bottom line: Etomidate can achieve effective sedation in children for a short procedure. Although respiratory effects were noted, none of them required assisted ventilation.
The three-bag IV acetylcysteine regimen for acetaminophen overdose is complicated and can result in medication/administration errors. [1] Two recent studies have attempted simplifying the regimen using a two-bag approach and evaluated its effect on adverse effects. [2, 3]
Study 1 [2]
Prospective comparison of cases using a 20 h, two-bag regimen (200 mg/kg over 4 h followed by 100 mg/kg over 16 h) to an historical cohort treated with the 21 h three-bag IV regimen (150 mg/kg over 1 h, 50 mg/kg over 4 h and 100 mg/kg over 16 h).
The two-bag 20 h acetylcysteine regimen was well tolerated and resulted in significantly fewer and milder non-allergic anaphylactic reactions than the standard three-bag regimen.
Study 2 [3]
Prospective observational study of a modified 2-phase acetylcysteine protocol. The first infusion was 200 mg/kg over 4-9 h. The second infusion was 100 mg/kg over 16 h. Pre-defined outcomes were frequency of adverse reactions (systemic hypersensitivity reactions or gastrointestinal); proportion with ALT > 1000 U/L or abnormal ALT.
The 2-phase acetylcysteine infusion protocol resulted in fewer reactions in patients with toxic paracetamol concentrations.
Final word: Two-bag regimens seem to offer advantages compared to the traditional three-bag regimen with regard to reduced adverse drug reactions. Look for more data, particularly on effectiveness, and a potential transition to a two-bag approach in the future.
Bottom Line:
There are so many variables to monitor during CPR; speed and depth of compressions, rhythm analysis, etc. But how much attention do you give to the ventilations administered?
The right ventricle (RV) fills secondary to the negative pressure created during spontaneously breathing. However, during CPR we administer positive pressure ventilation (PPV), which increase intra-thoracic pressure thus reducing venous return to the RV, decreasing cardiac output, and coronary filling. PPV also increases intracranial pressure by reducing venous return from the brain.
So our goal for ventilations during cardiac arrest should be to minimize the intra-thoracic pressure (ITP); we can do this by remembering to ventilate "low (tidal volumes) and slow (respiratory rates)"
What’s the name of this CT finding and name two potential causes?

Sever's disease also known as calcaneal apophysitis, is the most common cause of heel pain in the young adolescent (ages 8 to 12).
It can be thought of as the Achilles tendon equivalent of Osgood-Schlatter's disease (patellar tendon insertion pain).
It is a non inflammatory chronic repetitive injury.
Commonly seen bilaterally in up to two -thirds of cases.
Patients will complain of activity related pain to the heel.
There may be tenderness and local swelling at the Achilles tendon insertion.
Radiographs are not necessary for acute cases.
Treat with activity modification, heel raise, physical therapy.
Caffeine is the most commonly used psychoactive substance in the world. It is widely available in coffee, tea, chocolate,soft drinks, OTC medicines, and energy drinks. The vast majority of people consuming caffeine appear to suffer no harm while enjoying it's stimulating effects. This has led to the widely held perspective that caffeine is a completely benign substance with no adverse health effects exists.
Although, children and adolescents are at particular risk, many caffeine containing products are specifically marketed at them. Alarmingly, statistics demonstrate that caffeine intake among children and adolescents has increased by 70% in the last 30 years. Energy drinks are of special concern as they represent the fastest growing component of the beverage industry, contain significant quantities of caffeine as well as high levels of sugar, and can place children at high risk for caffeine intoxication.
There are many negative health consequences documented with caffeine use which occur in a dose dependent manner with individuals differing in their susceptibility to caffeine-related adverse effects:
Chronic Effects: