Although it is summer, preparations are being made for the 2016-2017 influenza season. The Center for Disease Control (CDC) no longer recommends the live attenuated influenza vaccine (LAIV4). The American Academy of Pediatrics has supported this statement.
The LAIV4 (the only intranasal vaccine available) was offered to patients over the age of 2 years without respiratory problems. Observational studies during the 2013-2015 seasons have shown that the LAIV4 has an adjusted vaccine efficacy of 3% compared to 63% for the inactivated vaccine (intramuscular). Children who received the intranasal vaccine were almost 4 times more likely to get the flu compared to children who received the injection.
Bottom line: Only the intramuscular shot is recommended for this upcoming season. This is causing many primary care practices to scramble to obtain enough vaccine.
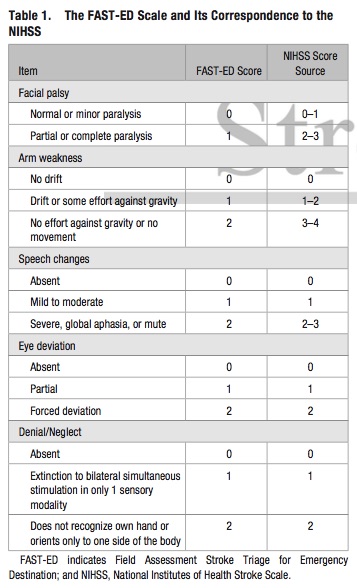
Bottom Line: Additional assessment of gaze deviation, aphasia and neglect, as included in the FAST-ED scale, increases the accuracy of predicting LVOS.
LVADs and RV Failure
Sesamoid Injuries
Unlike other bones in the human body that are connected to each other at joints, sesamoid bones are only connected via tendons (or are imbedded in muscle).
The largest sesamoid bone is the patella.
2 small sesamoid bones lie on the plantar foot near the great toe
Sesamoid bones can fracture and the surrounding tendons can become inflamed (sesamoiditis)
Traumatic injury is usually due to hyperextension and axial loading
Sx: Pain located under the great toe on the ball of the foot (Gradual with sesamoiditis and acutely with a fracture).
There may be associated swelling and bruising. Pain with palpation, flexion and extension.
The medial/tibial sesamoid is larger, has great weight bearing status and is more commonly injured that its lateral counterpart.
In many people (10 - 25%) the medial sesamoid of the foot has two parts (bipartite). This finding is bilateral in 25% of people.
This may confuse some providers as it may appear to be a fracture
Look for a smooth contour to the bones and clinically correlate (bruising, soft tissue swelling, etc.) if it is an incidental finding.
Other radiographic clues include
1) The fractured sesamoid is usually slightly larger than the lateral sesamoid while the bipartite sesamoid has a much larger medial sesamoid than lateral sesamoid
2) The fractured sesamoid shows a sharp, radiolucent, uncorticated line between the two fragments while the bipartite sesamoid has two corticated components
3) The fractured sesamoid fragments often fit together like pieces of a puzzle while the bipartite sesamoid has two components that do not fit together snugly
4) Other means to differentiate the two involve MRI and bone scanning
Treatment involves a stiff-soled shoe or applying a cushioning pad or J-shaped pad around the area to relieve pressure.
It may take months for the pain to subside.
http://www.apfmj-archive.com/afm5_3/afm50.htm#F1
There are many definitions for a disaster. Per the International Federation of Red Cross and Red Crescent Societies (IFRC), they define a disaster as:“…a sudden, calamitous event that seriously disrupts the functioning of a community or society and causes human, material, and economic or environmental losses that exceed the community’s or society’s ability to cope using its own resources. Though often caused by nature, disasters can have human origins.”
However, in the heat of the moment, a shorter definition is easier to remember. The IFRC also define a disaster as:
A shorter, more practical definition is:
Fluoroquinolone antibiotics are used to treat a wide range of infections and as prophylaxis against infection in certain immune compromised patients. In 2008 the FDA issued a boxed warning for tendonitis and tendon rupture for the fluoroquinolone antibiotic class, and in May 2016 a statement recommending the use of alternate therapies for uncomplicated UTIs and upper respiratory infections was issued. The mechanism by which fluoroquinolones causes tendon injury has not been elucidated, but may be related to oxidative stress caused by the overproduction of reactive oxygen species in tenocytes.
Adverse event reporting to the FDA is performed voluntarily by healthcare professionals and consumers through MedWatch. An analysis of tendon rupture events associated with fluoroquinolone use reported to the FDA’s Adverse Event Reporting System (FAERS) database was recently published.
What they found:
Application to clinical practice:
Plain films are commonly used to screen children for pelvic fractures or dislocations following blunt torso trauma
The sensitivity of this common screening practice is unknown
A recent study looked at this question.
Of 451 patients with pelvic fractures or dislocations, 382 had AP radiographs. Injury was correctly identified in 297 patients (sensitivity 78%).
The sensitivity was greater in the sicker subgroups :92% for those requiring operative intervention and 82% for those with hypotension
Plain AP pelvic radiographs should have a limited role in the sole evaluation of children with blunt torso trauma.
They should be incorporated in the assessment of hemodynamically unstable children and those in whom the clinician is not planning on otherwise obtaining an abdominal/pelvis CT.
Laundry detergent pods were introduced in 2012 to make washing clothes more "convenient." Since then, pediatric exposures to laundry detergent pods have increased as the use of these detergent pods have become more common in homes. Like other household chemical exposure, small, colorful candy like appearances of laundry detergent pods can attract the attention of < 3 years old children resulting in unintentional exposure due to curiosity or taste.
Most frequent clinical effects (2013 - 2014 national poison center data) from exposure to detergents in general (laundry detergent pods and nonpods & dishwasher detergent):
Laundry detergent pod vs. nonpods:
Laundry detergent pods (only) also resulted in following:
Cases of caustic exposure-like injuries have also been reported (corneal abrasion and esophageal injury)
Bottom line:
Pediatric laundry detergent (nonpods) exposures usually have self-limited symptoms. However, laundry detergent pod exposure can cause more serious clinical effects that may require hospitalization.
Multiple sclerosis (MS) relapses are defined as new or worsening neurologic deficits lasting 24 hours or more in the absence of fever or infection. Symptoms may be visual, motor, sensory, balance or cognitive. It is a clinical diagnosis, but the presence of a new gadolinium-enhancing lesion on MRI can be used as a radiologic marker of an MS relapse. However, it is unclear whether asymptomatic lesions should be treated, making it prudent to rely on the clinical evaluation rather than the MRI for diagnosis.
Moderate to severe relapses should be treated within 1 week of onset. The mainstay of treatment for relapses is IV methylprednisolone, usually dosed at 500mg to 1g per day for 3-7 days.
Similar symptoms occurring in the presence of fever, heat exposure, stress or infection (such as urinary or upper respiratory tract infections) are "pseudoexacerbations", and should not be treated as an MS relapse.
There are 4 types of respiratory failure that all providers should be familiar with
Type 1: Hypoxemic, PaO2 <50; this can include shunt , V/Q mismatch, or high altitude. Pulmonary edema, ARDS, pneumonia are common causes of this type of failure.
Type 2: Hypercapnic respiratory failure; decreased RR or tidal volume. This includes neuromuscular disorders including GBS or Myasthenia Gravis, in addition to medication overdose. COPD and asthma can lead to this type of respiratory failure as well.
Type 3: Peri-operative; atelectasis; decreased FRC from being supine or obese during the operative period.
Type 4: Shock or hypoperfusion leading to increased work of breathing and respiratory failure.
The PATCH trail, recently published in the Lancet, looked at whether giving platelets to patients, that were on anti-platelet therapy (e.g.: aspirin, clopedrigrel, or dipyridamole) for at least 7 days at the time of their spontaneous intracerebral hemorrhage, improved neurologic outcomes and mortality.
This was a large (60 hospitals) multicener, open-label, masked endpoint, randomized trial that enrolled a total of 190 patients (97 platelet transfusion and 93 standard care).
The outcomes were surprising. Patient in the Platelet group had a higher rat of death or dependence at 3 months (Adjusted OR 2.05; 95% CI 1.18 3.56; p = 0.0114).
The authors concluded "Platelet transfusion seems inferior to standard care for people taking anti-platelet therapy before a spontaneous intracerebral hemorrhage"
Though this is the first study to look at this, the studies design and outcomes should really make use reconsider whether we give these patients platelets. The thought is that ICB or hemorrhagic strokes also have a component of ischemic stroke and a watershed area that's blood flow becomes compromised with the platelet transfusion.
TAKE HOME POINT: We should not routinely transfuse platelets in our patients that were on antiplatelet therapy prior to their ICB.
In consideration of the recent shootings in Orlando, Florida, how common are intentional homicides globally?
Please keep the families and friends of the victims of the Orlando events, as well as the many emergency workers who helped them, in your thoughts and prayers.
Loperamide is a peripheral mu-opioid receptor agonist that is found in over the counter anti-diarrheal medication. Following the trend of opioid abuse epidemic, loperamide has been promoted on online drug-use forum as a treatment for opioid withdrawal and as a possible alternative to methadone. At the same time, recreational use of loperamide has been increasing as an opioid alternative. Unlike therapeutic use of loparamide (2 – 4 mg), loraparmide abusers take supratherapeutic doses (e.g. 50 – 100 mg) to penetrate the CNS to produce opioid effects.
In published case reports, loperamide caused cardiac Na channel blockade (similar to TCA and bupropion) and K channel blockade, resulting in EKG changes including QRS interval > 100 msec with terminal R wave in aVR and QTc prolongation, respectively. Loperamide associated death has also been reported (autopsy finding), although the exact cause of death was not determined.
It is unclear if administration of NaHCO3 can reverse the cardiac Na channel blockade as in TCA and bupropion as the clinical experiences have been limited.
Bottom line:
Heat Stroke
Medication-overuse headache (MOH) is one of the most common chronic headache disorders
Worldwide prevalence of 1 2%
Characterized by chronic headache and overuse of different headache medications
Withdrawal of the overused medication is the treatment of choice
A 2014 study looked at adolescent patients treated in a headache clinic with chronic post traumatic headaches (concussion headaches)
77 had chronic post-traumatic headache of 3-12 months' duration
54 of 77 (70.1%) met criteria for probable medication-overuse headache.
After the OTC medicine was stopped 68.5% had resolution or improvement !!
Excessive use of analgesics postconcussion may contribute to chronic post-traumatic headaches in some adolescents.
Sometimes the advise of "just keep taking the motrin and it'll get better" isnt the answer
Ketamine is gaining traction as a prehospital option for managing severe agitation or excited delirium syndrome. Previous reports have mostly been case series, but a new prospective study adds some important information that may help delineate ketamine's role in this setting. [1] The study and an accompanying commentary are both open access. [2]
What They Did
Open-label before-and-after prospective comparison of haloperidol (10 mg IM) versus ketamine (5 mg/kg IM) for the treatment of acute undifferentiated agitation.
What They Found
Appliation to Clinical Practice
Gadolinium - To Use or Not Use?
| Non-Contrast MRA/MRV | Contrast-Enhanced MRA/MRV | |
| How Does It Work? | * Time-of-flight (TOF) is a commonly used sequence * Relies on flow of blood into imaging plane * Difference between signal of blood and suppressed background tissue | * Similar to CT angiography/venography * Higher intravascular signal purely from gadolinium-based contrast, not dependent on flow
|
| Pros | * Does not require contrast
| * Generally better image quality * Shorter acquisition time |
| Cons | * Slow, turbulent, or retrograde flow may result in signal loss * Over-estimates stenosis * Longer acquisition time | * RIsks associated with contrast use * Timing of image acquisition important |
| Applications | * Patients with allergy to gadolinium, renal dysfunction, pregnancy * Evaluation of intracranial vessels and cerebral venous system | * Evaluation of stenoses and occlusions of the neck vessels and their origins at the aortic arch
|
In settings where community-acquired MRSA is prevalent, which antibiotic is best for uncomplicated wound infections?
New Study
What They Found
Application to Clinical Practice