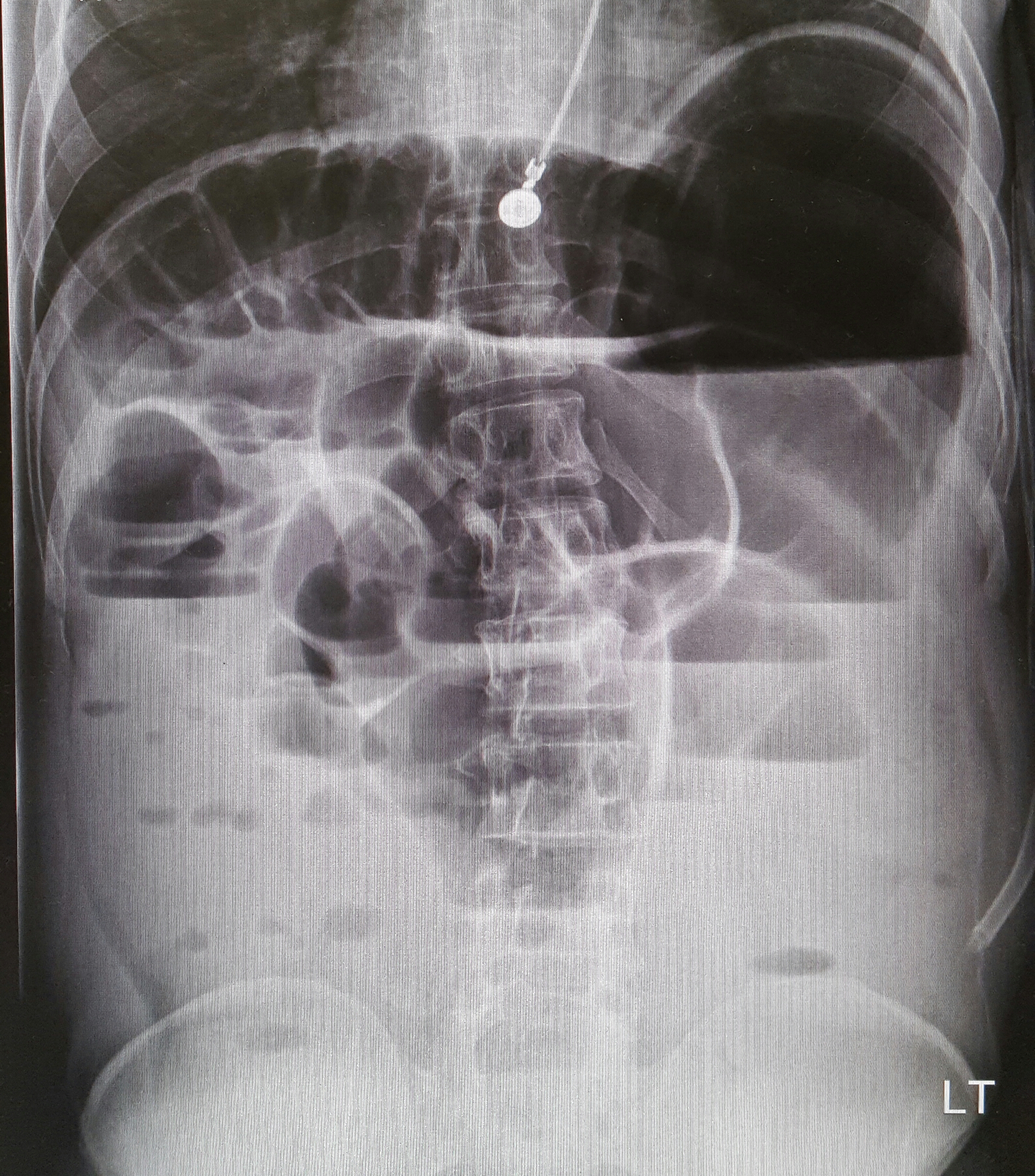
22-year-old male with history of autism, mental retardation who is non-verbal presents with abdominal pain and vomiting for one day. Patient was found clutching his abdomen and moaning. What's the diagnosis?
Retroperitoneal hemorrhage
The pathophysiology is unknown. Some hypothesize that occult vasculopathy and arteriosclerosis of the small vessels in the retroperitoneum may render them friable and therefore prone to rupture. This can be seen in minor trauma in sports and forceful vomiting or coughing. Spontaneous bleeding starts at the microvascular level, and large vessels become disrupted or stretched as the hematoma enlarges.
Retroperitoneal hemorrhage occurs in a variety of clinical circumstances, including spontaneous hemorrhage into a pre-existing benign adrenal cyst or bleeding from a left inferior phrenic artery, tumors of the adrenal gland and kidney, rupture of any blood vessel (most commonly infrarenal aorta); percutaneous interventions (such as cardiac catheterization), trauma, and polycythemia vera,
It is most commonly seen in association with patients with bleeding abnormalities, in HD patients and with anticoagulation therapy,. Risk is much greater with unfractionated heparin therapy than with warfarin. In most of the heparin patients studied, their coagulation parameters were in the therapeutic range.
Patients may present to the non acute area of the ED with back, lower abdominal or groin discomfort, Over time, this may progress to hemodynamic instability, and a fall in hemoglobin, Early identification is crucial to improving patient morbidity and mortality. Early symptoms depend on the location of the bleeding.
Hematoma near or within the iliopsoas muscle usually presents as femoral neuropathy (groin pain or leg weakness).
Femoral neuropathy caused by retroperitoneal hematoma can present with sudden onset severe pain in the affected groin and hip, with radiation to the anterior thigh and the lumbar region. This can easily be missed as the presentation is similar to a pulled msucle or strained hip/back. Iliopsoas muscle spasm often results in the characteristic flexion and external rotation of the hip, and any attempt to extend the hip will result in severe pain. Over time, pain and parasthesia in the antero-medial thigh and leg is seen.
Non –communicable diseases (NCDs), primarily cardiovascular diseases, cancer, respiratory diseases and diabetes, are significantly increasing globally. According to the WHO, cardiovascular diseases alone account for 17.5 million deaths annually- the most of any NCD.
If someone has return of spontaneous circulation after cardiac arrest, but does not have ST-elevations on their post-arrest ECG, should you emergently activate the cath lab?
In a just released systematic review and meta-analysis in Resuscitation, Dr. Millin and colleagues found that almost one third of patients successfully resuscitated without ST elevation on their ECG had a culprit lesion that would benefit from emergent intervention.
Bottom Line: While this is not definitive proof to emergently activate the cath lab for a NSTEMI, it is another strong indication that post cardiac arrest patients without ST elevation may benefit from emergent percutaneous coronary intervention.
Pitfalls with PLR
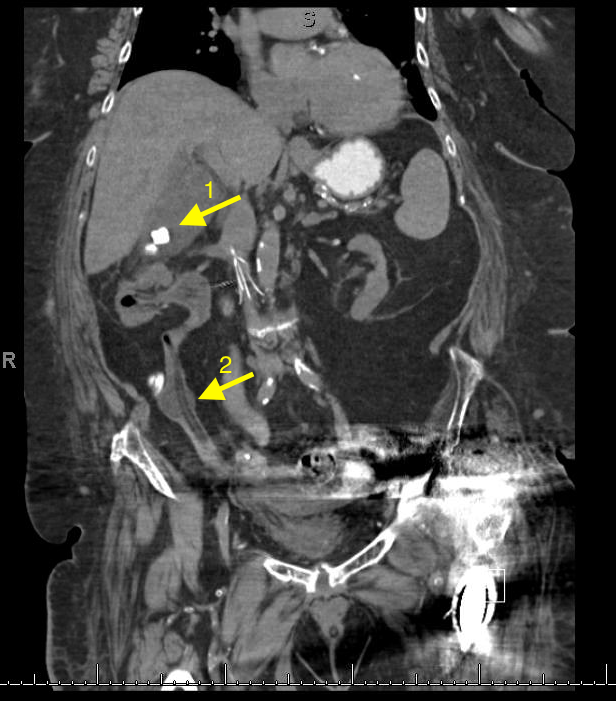
A 67 year old female with history of CVA, presented from a nursing home with RUQ abdominal pain and inablitiy to tolerate PO for 3 days. A CT scan of her abdomen was obtained. What is the diagnosis ?

Patellofemoral Syndrome Treatment options
Patients do best with a combined intervention (ie, exercise therapy, education, manual therapy and taping) plan or patellofemoral bracing may improve outcomes for people with patellofemoral syndrome and the subtype of patellofemoral osteoarthritis.
For for the ED, we can start NSAIDs, and then have them follow up with Physical Therapy, A sports trainer if in organized sports, or with a sports medicine physician/PCP. Physical therapy is targeted at strengthening the quadricep muscle particularly vastus medialis, which improves the patella’s tracking with knee flexion.
114 children with bronchiolitis had end tidal carbon dioxide (ETCO2) measured on presentation to the ED. The ETCO2 levels did not differ significantly between admitted and discharged patients. In the subset of admitted patients, there was no correlation with ETCO2 on admission and days of oxygen requirement or length of stay.
Bottom line: Initial ETCO2 does not predict outcome for patients with bronchiolitis.
Naloxone has been used to reverse opioid-induced respiratory depression for decades. The “standard” dose of opioid intoxication has been 0.4 mg. However, over the past decade, initial naloxone dose for opioid intoxication has evolved to recommend a lower initial dose (0.04 – 0.05 mg).
A recent article by Connors et al. reviewed 25 medical resources (internet, medical texts and study guides) of different medical specialties (internal medicine, medical toxicology, emergency medicine, pediatrics, anesthesiology, pain medicine and general medicine)
Findings:
Recent editions of emergency medicine text (Rosen’s and Tinitinalli) recommend using 0.04 – 0.05 mg IV in ED patients with history of opioid dependence. Higher doses of naloxone are recommended for non-opioid dependent/apneic patients.
However, history of opioid dependence is difficult to obtain in patients with opioid induced CNS/respiratory depression.
Administering 0.4 mg or higher dose may/can acute agitation or opioid withdrawal symptoms that can utilize more ED resources to calm agitated patient/management of withdrawal. Thus it may be prudent to use low-dose strategy (0.04 mg IV with titration) to minimize the risk of precipitating naloxone-induced opioid withdrawal/agitation.
Bottom line:
In opioid-induced respiratory depression/apneic patients:
To make 0.04 mg naloxone solution:
During rapid sequence intubation (RSI) we endeavor to avoid positive pressure ventilation, prior to securing a definitive airway. As such, an adequate buffer of oxygen is necessary to ensure a safe apneic period. This process involves replacing the residual nitrogen in the lung with oxygen. It has been demonstrated that a standard nonrebreather (NRB) mask alone does not provide a high enough fractional concentration of oxygen (FiO2) to optimally denitrogenate the lungs (1). Even when a nasal cannula at 15L/min is utilized in addition to the NRB, the resulting FiO2 is not ideal. A bag-valve mask (BVM) with a one-way valve or PEEP valve has been demonstrated to provide oxygen concentrations close to that of an anesthesia circuit. But its effectiveness is drastically reduced if a proper mask seal is not maintained during the entire pre-oxygenation period (1). This is not always logistically possible in the chaos of an Emergency Department intubation.
A standard NRB with the addition of flush-rate oxygen appears to be a viable alternative. Recently published in Annals of Emergency Medicine, Driver et al demonstrated that a NRB with wall oxygen flow rates increased to maximum levels, rather than the standard 15L/min, provided end-tidal O2 (ET-O2) levels similar to an anesthesia circuit (2).
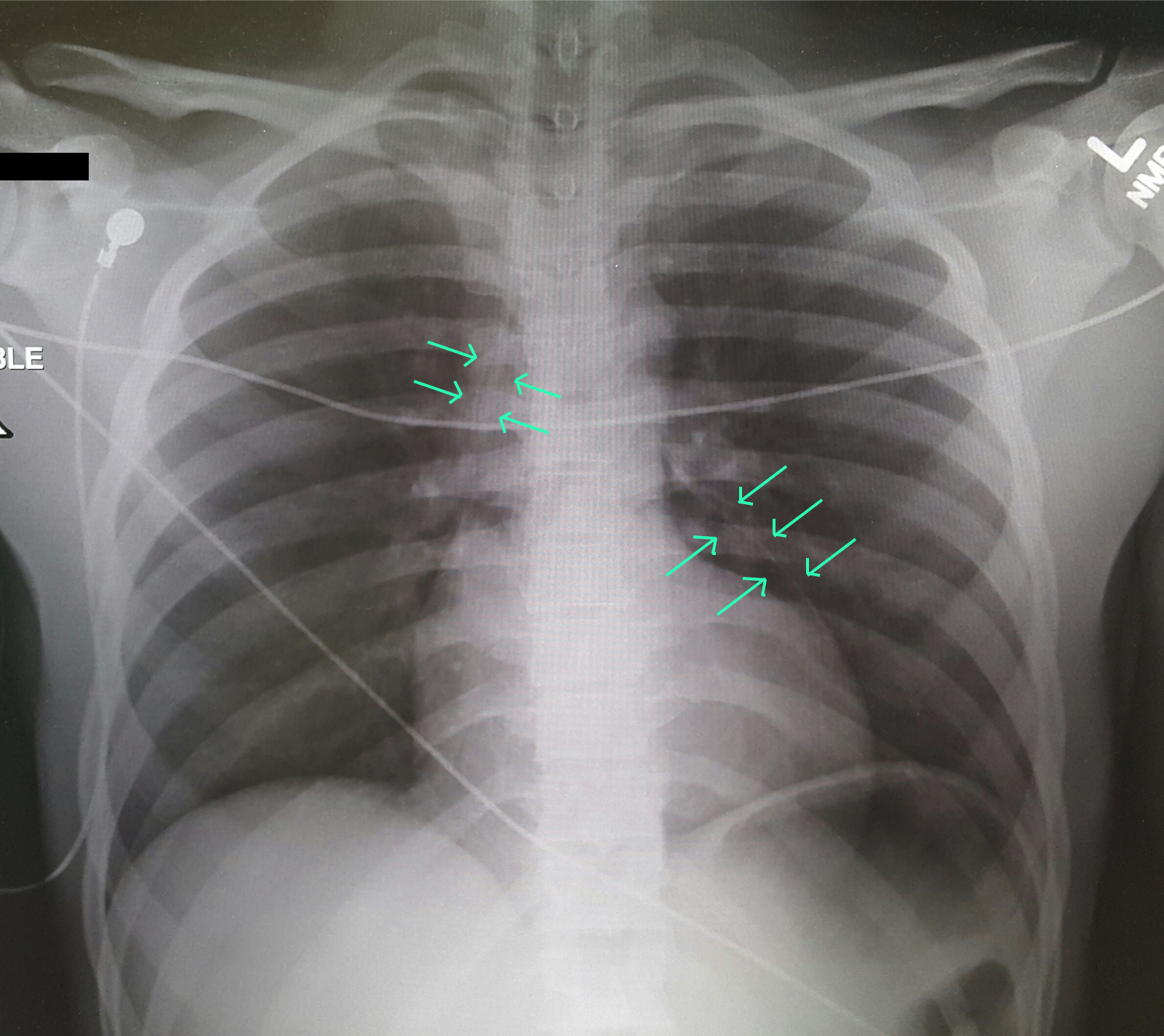
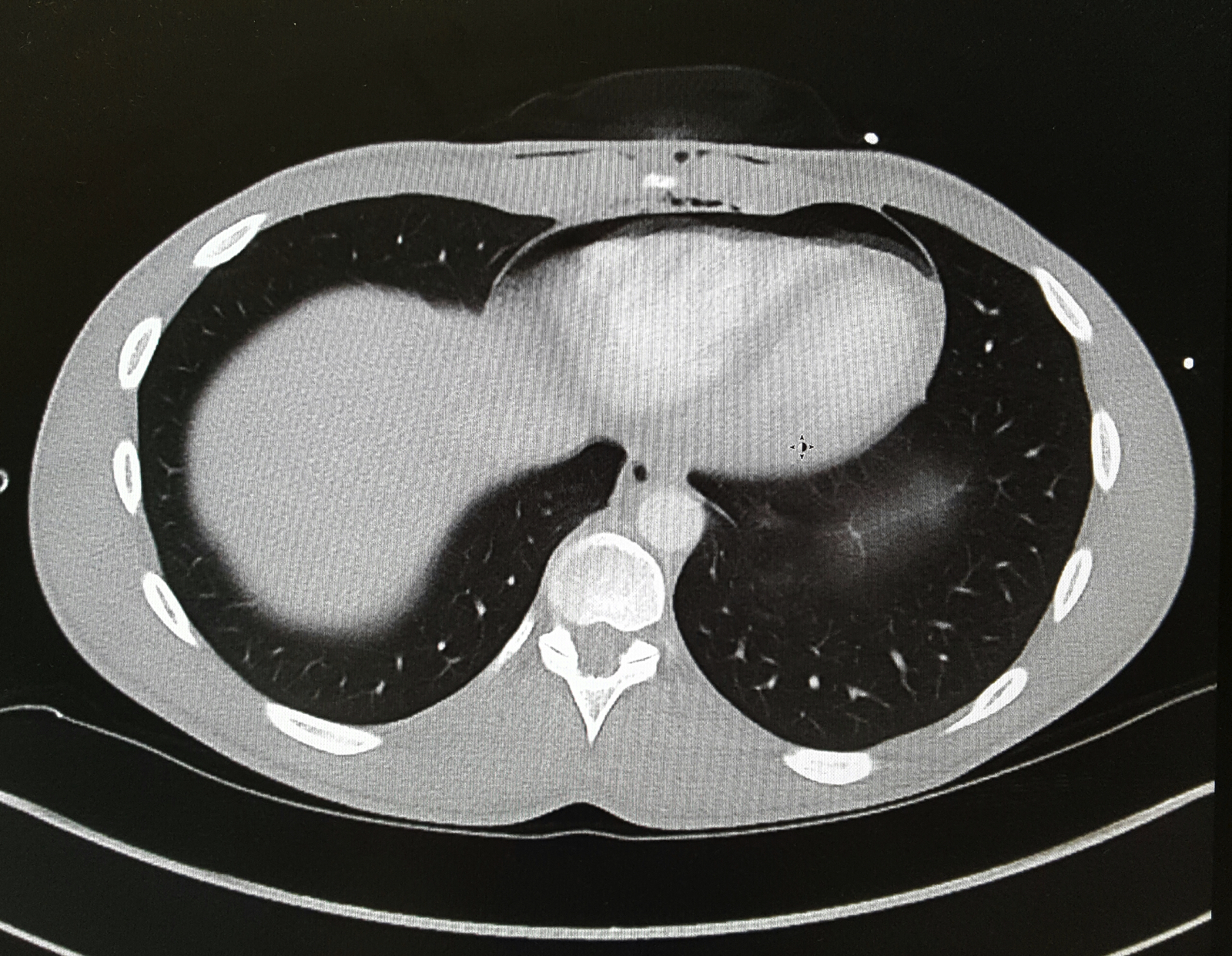
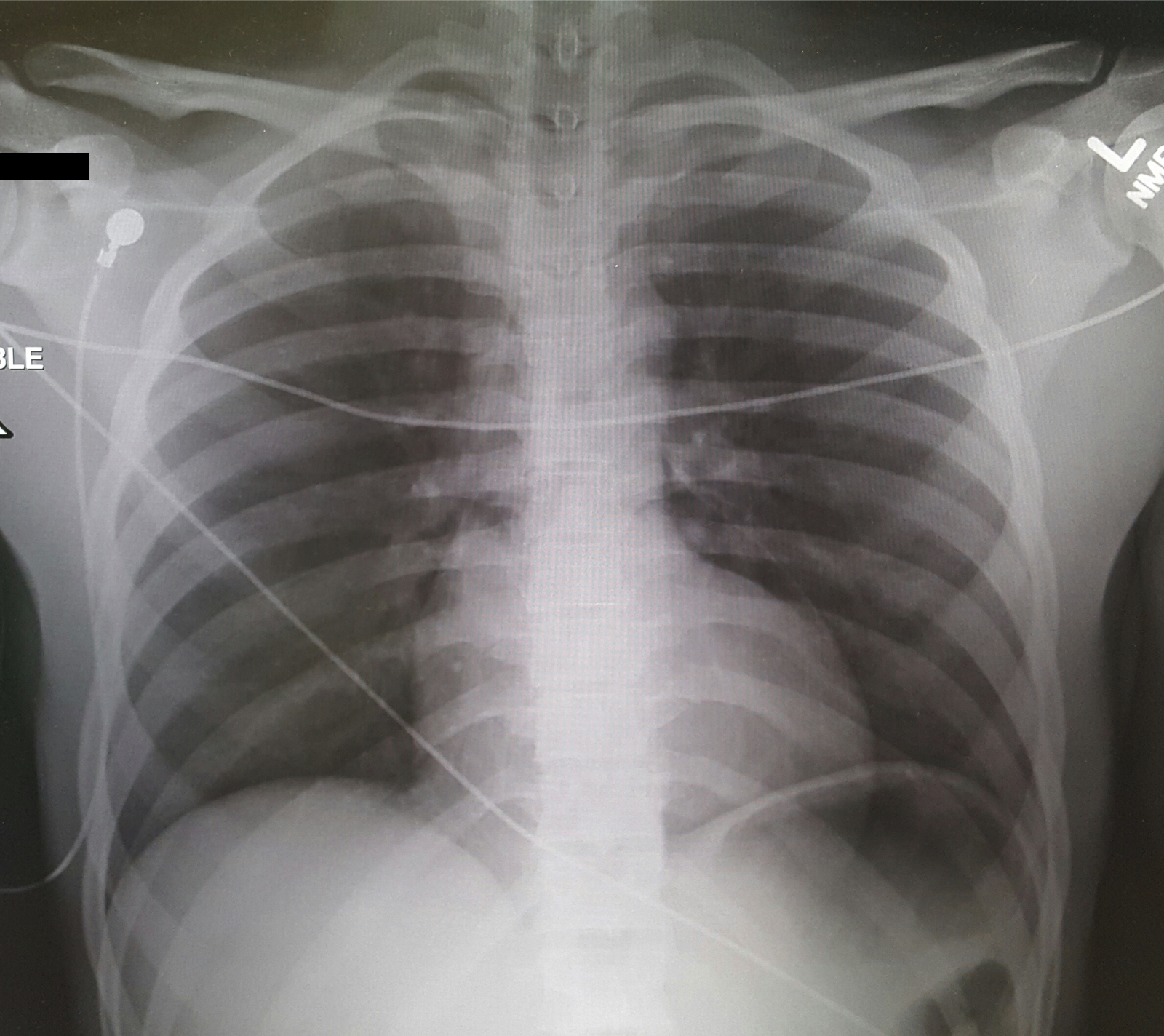
A 25-year-old male was brought in by EMS with a stab wound to the chest. What's the diagnosis?
Young athletes, especially around the age of puberty, are at higher risk for pelvic avulsion fractures
Often seen in sports that require sprinting, rapid changes in movement or jumping
Caused by sudden, forceful contraction of the muscles of the abdominal, the hip and thigh or the hamstring
Avulsion fractures can occur at many areas of the pelvis.
A mnemonic is: Alabama’s stoned rappers got ill hunting armadillos
· Iliac crest: Abdominal muscles
· Anterior superior iliac crest: Sartorius
· Anterior inferior iliac crest: Rectus femoris
· Greater trochanter: Gluteal muscles
· Lesser trochanter: Iliopsoas **(rare in adults)
· Ischial tuberosity: Hamstrings
· Pubic symphysis: Adductor group
http://roentgenrayreader.blogspot.com/2010/07/pelvic-avulsion-fractures.html
** Isolated nontraumatic avulsion fractures of the lesser trochanter in adults is a pathognomonic sign of metastatic disease
This site has some good images of common injury patterns
http://radiopaedia.org/articles/apophyseal-avulsion-fractures-of-the-pelvis-and-hip
Antipsychotic as a class has diverse range of toxicity. The atypical (2nd generation) antipsychotics are considered to possess less toxicologic manifestation compared to the typical (1st generation) antipsychotics - lower K channel blockade and minimum Na channel blockade properties. However, select atypical antipsychotics overdose can results in significant morbidity in addition to sedation.
Alpha-1 blockade (hypotension)
Antimuscarinic effect (anticholinergic toxicity)
Delayed rectifier K channel blockade (QT prolongation)
Bottom line: Although lethal overdose from atypical antipsychotics are rare, they can result in significant clinical toxicity when ingested alone or in combintation with other classes of medications.
Bottom Line:
--Aggressive BP management (SBP <140) in atraumatic intracerebral hemorrhage (ICH) does NOT signifcantly improve mortality or disability compared with traditional goal (SBP <180) [1]
--However, a lower goal (SBP <140) has been shown to decrease hematoma size and be safe compared to a higher goal (SBP <180) [2]
Prothrombin complex concentrate (PCC) and fresh frozen plasma (FFP) are used for INR reversal in patients on vitamin K antagonists (VKA) (e.g., warfarin) with life-threatening bleeding. Guidelines from the Neurocritical Care Society and Society of Critical Care Medicine recommend using PCC over FFP for patients with VKA-associated hemorrhage and an INR >=1.4.
New study-INCH trial:
What they found:
Application to clinical practice:
Zika virus and its transmission is currently an important infectious disease topic in the United States and the Western Hemisphere. With domestic spread in the Continental United States, and the likely further spread to other parts of the southern United States, continued vigilance by healthcare providers remains important.
What are the signs and symptoms of Zika?
Most common signs and symptoms are:
Other symptoms can include
Symptoms can generally last 2 to 7 days. Most individuals will have minimal or no significant symptoms and may not seek medical care. These symptoms are similar to other arboviruses, such as dengue or chikungunya. Potential serious complications include Guillian Barre syndrome.
Of course, the main concern remains infection of pregnant women and the impact that Zika has on the developing fetus, especially for the brain.
Ketamine for RSE?
Ataxia is an important clinical sign of cerebellar pathology, but how is it actually described?
Stance ataxia: inability to stand with feet together for more than 30 seconds
Gait ataxia
Sensory ataxia: the first 2 elements, in addition to a positive Romberg sign
Truncal ataxia: oscillation of body while sitting or standing
Limb ataxia: functional impairment in performing actions such as writing or buttoning and improves with slowing down the movement
Dysdiadokinesia: impairment of rapidly alternating movement
Intention tremor: tested by finger-to-nose and heel-to-shin.
Dysmetria: pastpointing or undershooting on finger-chasing or shin-tap.
Dysarthria: irregular and slow speech with unnecessary hesitation
Nystagmus and other ocular disturbances, such as ocular flutter and opsoclonus.
The first 3 are present in both cerebellar pathology and loss of proprioceptive input, the rest are usually due to cerebellar pathology or ataxic syndrome.