Below is a list of pharmacy-related pearls from the 2016 Surviving Sepsis Guidelines:
At the Society of Critical Care Meeting (SCCM) this month, updates to the Surviving Sepsis Guidelines were released. Recommendations include:
--Initial 30mL/kg crystalloid resuscitation with frequent reassessment of fluid responsiveness using dynamic (not static) measures [goodbye CVP/ScvO2!]
--Initiation of broad-spectrum antibiotics within ONE hour of sepsis recognition [two agents from different classes]
--Further hemodynamic assessement (e.g. echo for cardiac function) if clinical assessment does not reveal the type of shock [get out the ultrasound!]
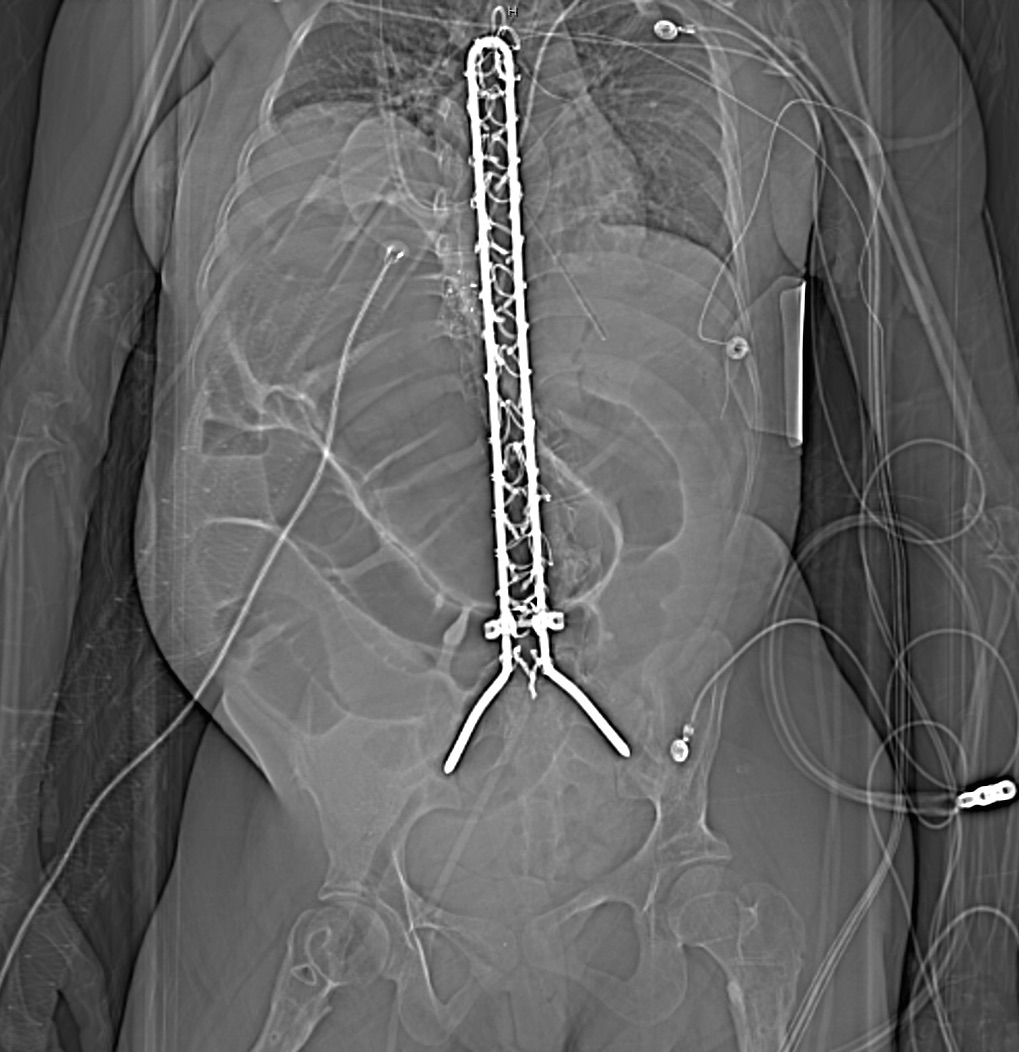
25 year-old female with hx of cerebral palsy with significant developmental delay, s/p G-tube who presented with acute hypoxic respiratory failure, hypotension and a distended, tense abdomen. A CT was done with the scout film below. What's the diagnosis?
During a busy ED shift, your 40yo charge nurse asked you to look at his hand. He is known avid mountain biker. He has pain in his right 4th and 5th digits. . He feels a lack of coordination and a feeling of “clumsiness” of the hand. Where is his possible nerve compression and what do you expect to find on exam?
Ulnar nerve entrapment is sometimes called “handlebar palsy.”
Compression location is Guyon’s canal.
The ulnar nerve supplies the intrinsic muscles of the hand AND the extrinsic muscles for flexion of the 4th and 5th digits. This is what aids in a “power grip” and why he may have diminished grip strength on exam.
Also innervates the ADDuctor pollicis and 1st dorsal interosseous muscles (pinch)
Note the ulnar nerve also passes through the radial tunnel at the elbow. Entrapment here is called Radial tunnel syndrome or Cubital tunnel syndrome and causes forearm pain and paresthesias in the 4th and 5th digits with grossly normal motor and sensory function.
As a follow up to Dr. Winter’s Pearl on Anaphylaxis on 1/24/2017, here’s a handy pearl for pediatric anaphylaxis (part 1).
Anaphylaxis: rapid and potentially life-threatening involvement of at least 2 systems following exposure to an antigen.
Medications (max: adult doses)
Get it?!?! Easy right? Instead of fumbling through an app or reference card during your next case of pediatric anaphylaxis, be a rock star "EM DR" by remembering the “Rule of 2’s”.
(Can't help it...ya'll know I love my mnemonics!!)
Methadone overdose produces classic signs and symptoms of opioid intoxication - CNS and respiratory depression with pinpoint pupils. However, methadone overdose has also been associated with hypoglycemia – a relatively uncommon adverse effect.
Bottom line:
Patients may present to the ED with new onset weakness due to myasthenia gravis (MG). A group that is frequently missed is late-onset MG, which occurs after the age of 50. It is frequently misdiagnosed as a stroke or transient ischemic attach (TIA).
Two cardinal features:
Bonus pearl: Ocular symptoms are present in up to 85% of patients with MG, with unilateral ptosis or asymmetric bilateral ptosis being the most common presentations.
Epinephrine in Anaphylaxis
More studies are needed, but the existing data shows that medical adhesives may be quicker without impacting cosmetic and functional outcome.
Urine drug screens are most commonly performed by immunoassay technology utilizing monoclonal antibodies that recognizes a structural feature of a drug or its metabolites. They are simple to perform. provide rapid screening, and qualitative results on up to 10 distinct drug classes with good sensitivity but imperfect specificity. This can lead to false positive results and the need for confirmatory testing. UDS does not detect synthetic opiates or cannabinoids, bath salts (synthetic cathinones), and gamma-hydroybutyrate. Most common drug classes detected are the following:
· Opioid deaths, such as from heroin and prescription opioids, are a major problem globally
· In the U.S., since 1999 overdose deaths from prescription opioids have quadrupled.
o Almost half of opioid deaths involve a prescription opioid
· The most common drugs related to prescription opioid deaths are:
o Methadone
o Oxycodone
o Hydrocodone
It is not uncommon for critically ill patients to require invasive monitoring of their blood pressure. In these patients, radial arterial lines are often inserted. Traditionally these lines are placed using palpation of the radial pulse. This technique can lead to unacceptably high failure rate in the hypotensive patient commonly encountered in the Emergency Department.
A recent meta-analysis by Gu et al demonstrated the use of dynamic US to assist in the placement of radial arterial lines decreased the rate of first attempt failure, time to line insertion and the number of adverse events associated with insertion.
You are covering a sporting event or working an ED shift when a young adolescent athlete without significant PMH presents with SOB and wheezing associated with exercise.
You immediately think exercise-induced asthma, prescribe a short-acting bronchodilator and pat yourself on the back.
While you may be right, there is increasing recognition of an alternative diagnosis
Exercise-induced laryngeal obstruction (EILO)
During high intensity exercise, the larynx can partially close, thereby causing a reduction in normal airflow. This results in the reported symptoms of SOB and wheezing.
This diagnosis has previously been called exercise induced vocal cord dysfunction. As the narrowing most frequently occurs ABOVE the level of the vocal cord, EILO is a more correct term.
While exercise induced bronchoconstriction has a prevalence of 5-20%, EILO is less common with a prevalence of 5-6%.
Patients are typically adolescents, with exercise associated wheezing and SOB, frequently during competitive or very strenuous events. Wheezing is inspiratory and high-pitched. Symptoms are unlikely to be present at time of medical contact unless you are at the event as resolution occurs within 5 minutes though associated cough or throat discomfort can persist after exercise cessation. EIB symptoms typically last up to 30 minutes following exercise.
Inhaler therapy is unlikely to help though some athletes report subjective partial relief. This may be explained as approximately 10% of individuals have both EIB and EILO.
In athletes with respiratory symptoms referred to asthma clinic, EILO was found in 35%.
Consider EILO in athletes with unexplained respiratory symptoms especially in those with ongoing symptoms despite appropriate therapy for EIB.
A small retrospective study of an acute poisoning cohort attempted to identify risk factors for severe outcome in salicylate poisoning.
Severe outcomes were defined as
A multivariate analysis of 48 patients showed that older age and increased respiratory rate were independent predictors of severe outcomes when adjusted for salicylate level.
Initial salicylate acid level was not predictive of severe outcome.
Elevated lactic acid level was also a good predictor of severe outcome in univariate analysis but not in multivariate analysis.
Limitations
Bottom line
--Recent meta-analysis comparing continuous infusion versus intermittent bolus dosing of beta-lactam antibiotics demonstrates mortality benefit (NNT = 15) in patients with severe sepsis or septic shock. (1)
--Consider beta-lactam continuous infusion on your septic patients if your hospital pharmacy allows
[Thanks to Anne Weichold, CRNP for providing the article for this pearl!]
A 60 year-old man with history of atrial fibrillation, CAD presents with left lower leg/foot pain for a few days. His foot is seen below. What's the diagnosis?


In a study comparing ketorolac IV doses of 10 mg, 15 mg, and 30 mg, no difference in pain score reduction or need for rescue analgesia was observed.
Lactic acidosis is the most common cause of anion gap metabolic acidosis in all hospitalized patients. An elevated lactate level is an important marker of inadequate tissue perfusion causing subsequent shift to anaerobic metabolism and occuring in a variety of disease states such as sepsis. In patients with unexplained lactic acidosis without systemic hyoperfusion or seizure suspect the following toxins:
Vitamin B12 deficiency can cause significant disease, including severe neurologic problems. However, patient presentations can vary greatly.
Signs and symptoms can include:
Prolonged B12 deficiency can lead to significant neurologic complications, frequently related to the spinal cord, and can include: