Vasovagal syncope is a subtype of neurally mediated syncope, and it is distinctly different from orthostatic hypotension.
Patients with orthostatic syncope have severe orthostatic hypotension that results in transient loss of consciousness immediately or within moments of standing up. This is different from neurally mediated syncope, which develops gradually under conditions of prolonged orthostatic stress such as standing for several minutes. Tilt table testing is useful for true orthostatic syncope, but not for neurally mediated syncope. In addition, checking for “orthostatic hypotension” may not capture patient with orthostatic syncope, because the hypotension occurs so quickly after standing up. Of note, patients may still have orthostatic tachycardia or intolerance with neurally mediated syncope.
Antibiotics in Sepsis
It is common teaching that a Segond Fracture is associated with ACL tears. A reverse Segond fracture, avulsion fracture of the knee due to avulsion of the deep fibers of the medial collateral ligament, has also been described that was initially reported as associated with PCL tears. However, a more recent study has not been able to collaborate the PCL connection, but has shown that a reverse Segond fracture is associated with multiple ligamentous injuries to the knee.
Take home point: If you note a Reverse Segond fracture on your plain flips have the patient followup with orthopedics for a possible MRI, as they probably have other ligamentous injuries that might need treatment.
IM ziprasidone (Geodon) has a relatively quick onset of action with a half-life of 2-5 hours. Although commonly used in adults, there has not been a study looking at an effective dose in pediatrics. Based on the study referenced, the suggested pediatric dose of ziprasidone is 0.2 mg/kg (max 20mg).
Currently, Nigeria is having the worst outbreak of bacterial meningitis in almost 10 years, involving 23 states, 13,420 suspected cases, and 1,069 deaths, as of May 9.
Bacterial meningitis outbreaks frequently occur in West Africa. The area most frequently struck by epidemics of bacterial meningitis is in the sub-Saharan region of Africa. This includes 26 countries and over 400 million people. Epidemics most often occur in the dry season from December-June. Neisseria meningitides serogroup A historically accounts for approximately 90% of the cases.
The U.S. Centers for Disease Control and Prevention recommends quadrivalent vaccines (protects against four serogroups A, C, W, and Y) for individuals traveling or living in countries in which meningococcal disease is hyperendemic or epidemic.
High flow nasal cannula (HFNC) is a valid option in the management of acute hypoxic respiratory failure (AHRF) without hypercapnia, as evidenced by multiple studies including the FLORALI trial. Failure of HFNC, however, may result in delayed intubation and worsened clinical outcomes.
Factors predicting HFNC failure and subsequent intubation include:
Consider whether or not HFNC is appropriate in your patient with AHRF, and if you use it, reevaluate your patient to ensure improvement, or escalate their respiratory support.
Iliotibial band tendonitis
IT band is the continuation of the tensor fascia lata and inserts on the tibia at Gerdy's tubercle
Common cause of lateral knee pain seen in Primary care/Sports med clinics
Mechanism: May be due to excessive friction between the IT band and the lateral femoral condyle
Second most common overuse injury of the knee (PF syndrome). Not an acute event.
Affects up to15% of active individuals
Impingement zone is at 30 degrees of knee flexion
Most common in runners and cyclists
Pain localized over the lateral femoral condyle. Better w/ rest. Often occurs at a predictable distance into the run and not at onset.
Exacerbated with changes to mileage or running terrain.
Additional risks include poor shoes (best to change every 300 to 500 miles), excessive foot pronation (pes planus), quad versus hamstring strength asymmetry, weak hip ABductors, leg length discrepancy, tight IT band.
Lisfranc Fracture: Typically consists of a fracture of the base of the second metatarsal and dislocation, though it can also be associated with fractures of a cuboid.
Click below see image of fracture
Bottom line: Do not prescribe codeine or tramadol for cough or pain in children and breastfeeding moms.
Haloperidol has a higher D2 receptor antagonist effect than standard antiemetic treatment agents such as metoclopramide. In addition, newer antipsychotic agents such as Olanzapine have a high affinity at multiple antiemetic sites such as the dopamine and serotinergic receptors.
While formal RCT's are still in the works, multiple sources including palliative care, emergency medicine, and pain journals support their use in refractory emesis.
Consider Haloperidol 3-5 mg IV.
Check an EKG for long QTc prior to use. Consider dose reduction of haloperidol in those with hepatic impairment. Also consider dose reduction in patients taking carbamazepine, phenytoin, phenobarbital, rifampicin, or quinidine due to that pesky CYP3A4 inhibition.
Consider Olanzapine 2-5 mg IV.
Several case reports have shown a higher rate of success with olanzapine for refractory emesis. Olanzapine has similar precautions as those to haloperidol (EKG, hepatic impairment), although it's CYP drug interactions are less common. Additionally, use olanzapine cautiously in hyperglycemic patients as there are several case reports of olanzapine prompting episodes of DKA. Consider frequent blood sugar checks or small doses of insulin in hyperglycemic patients.
Take Home Points:
Consider the antipsychotic agents Haloperidol or Olanzapine for patients with refractory emesis, they may be more effective than traditional antiemetics.
Get an EKG prior to administration to check for QTc prolongation. As the classical and atypical antipsychotic agents are sedating, use caution in conjunction with other sedating medications (such as benzodiazepines).
Ventilator Settings for the Post-Arrest Patient
Septic Arthritis in Children
Classic presentation: Pain, fever (may not always be present)
Limited range of motion of joint or refusal to bear weight,
Joint swelling (difficult to visualize in hip or shoulder),
Limb held in position that allows greatest capsular volume (elbow held in 30° flexion for example)
Diagnostic testing may include diagnostic markers (ESR, CRP) or imaging (US/MRI)
Most common organisms: Staph and Strep, Neisseria (adolescents), HACEK organisms, consider gram negatives in immunocompromised children
DDX: Transient synovitis, osteonercrosis or osteomyelitis, Psoas abscess, acute leukemia, Lyme disease
A common ED presentation is the child with the painful limp
35% of all cases of septic arthritis
>50% of cases occur in children younger than 2yo
Hip held in flexion, Abduction, external rotation
Fever and inflammatory markers are more sensitive than WBC count and refusal to bear weight
Kocher criteria:
1) Refusal to weight bear on affected side
2) Sed rate greater than 40mm/hr
3) Fever (>38.5°C
4) WBC count of >12,000 mm3
IF
- 4/4 criteria are met, there is a 99.6% chance of septic arthritis;
- when 3/4 criteria are met, there is a 93% chance of septic arthritis;
- when 2/4 criteria are met, there is a 40% chance of septic arthritis;
- when 1/4 criteria are met, there is a 3% chance of septic arthritis;
CRP can also be incorporated into a diagnostic algorithm
CRP>2.0 (mg/dl) in a child who refuses to bear weight yields a 74% probability of septic arthritis
Predictive factors of asthma development in patients diagnosed with bronchiolitis include:
- Male sex (OR 1.3)
- Family history of asthma (OR 1.6)
- Age greater than 5 months at the time of bronchiolitis diagnosis (OR 1.4)
- More than 2 episodes of bronchiolitis (OR 2.4)
- Allergies (OR 1.6)
Lactic acids are often elevated in critical care patients (e.g. septic shock). It can be also elevated in setting of drug overdose or less frequently in therapeutic use due to interference of oxidative phosphorylation. Some of the agents include:
Bottom line:
The Centers for Disease Control and Prevention (CDC) just released an official health advisory through the Health Alert Network entitled: “CDC Recommendations for Diagnosing and Managing Shigella Strains with Possible Reduced Susceptibility to Ciprofloxacin”
Concerning treatment, one key point is:
Do not routinely prescribe antibiotic therapy for Shigella infection. Instead, reserve antibiotic therapy for patients for whom it is clinically indicated or when public health officials advise treatment in an outbreak setting.
o Shigellosis is generally a self-limited infection lasting 5-7 days.
o Unnecessary treatment with antibiotics promotes resistance.
o Treatment can shorten the duration of some illnesses, though typically only by 1-2 days
Save time by using bedside ultrasound to confirm above-the-diaphragm central venous catheter (CVC) placement rather than waiting for chest x-ray confirmation:
1. Perform rapid push of saline (it doesn’t have to be agitated) through CVC while cardiac probe is placed with right atrium in view. Immediate visualization of bubbles (or “atrial swirl”) essentially confirms correct placement.
2. Perform the usual search for ipsilateral lung-sliding and the waves-on-the-beach to rule out procedural pneumothorax.
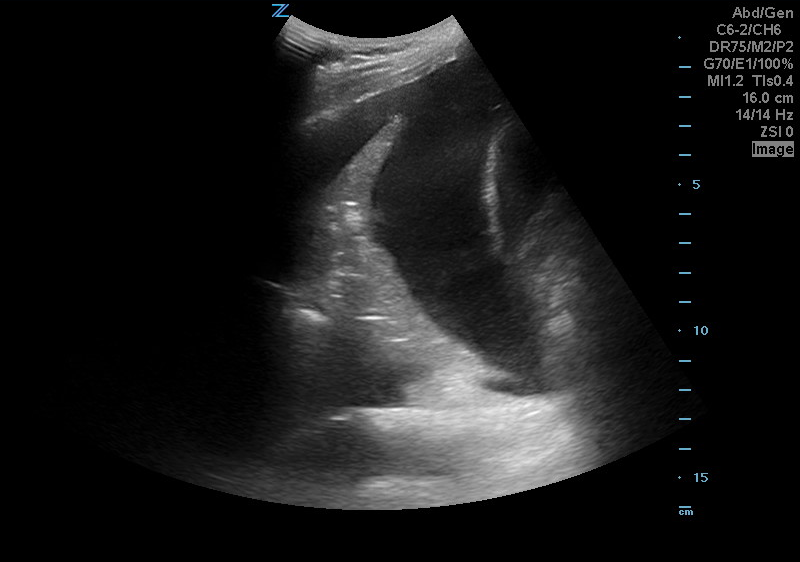
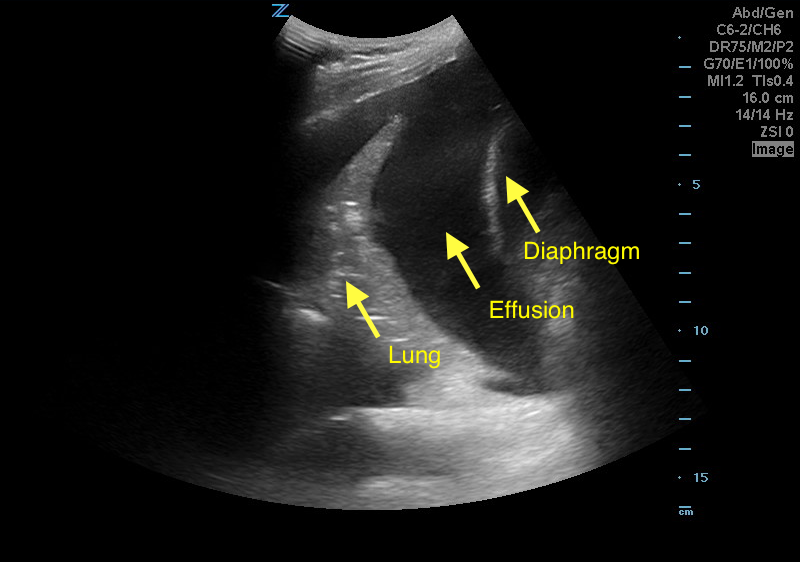
A 50 years old male with a history of CHF, presenting to the ED with progressively worsening shortness of breath. POCUS was performed. The picture shows the left lower part of the chest. What is the diagnosis?