Misclassification of adverse drug effects as allergy is commonly encountered in clinical practice and can lead to use of suboptimal alternate medications which are often less effective.
The World Health Organization announced on November 18th, 2016 that the Zika virus and associated consequences will no longer Public Health Emergency of International Concern. This changes the originally recommendation in February 2016.
However, Zika remains a “significant enduring public health challenge requiring intense action”. The consequences of the disease remains significant, especially for pregnant women and infants.
--In this study, PE was diagnosed in ~17% of patients hospitalized for syncope (though this represents only ~4%% of patients presenting to the ED with syncope).
--Patients with PE were more likely to have tachypnea, tachycardia, relative hypotension, signs of DVT, and active cancer -- take a good history and do a good physical exam!
--Consider risk stratifying (Wells/Geneva) and/or performing a D-dimer (i.e "rule out" PE) on your syncope patients, particularly when no alternative diagnosis is apparent.
Incidence and Cost of Ankle Sprains US Emergency Departments
In a sample of 225,114 ED patients with ankle sprains:
Lateral ankle sprains represent the vast majority of all ankle sprains (91%).
Lateral ankle sprains incur greater ED charges than medial sprains ($1008 vs. $914).
Lateral ankle sprains were more likely to have associated pain in the limb, sprain of the foot and abrasions of the hip/leg than medial sprains.
Medial sprains were more likely to include imaging.
Hospitalizations were more likely with high ankle sprains than lateral sprains.
There is a higher incidence of ankle sprains in younger patients (≤25 years) and in female patients (57%).
Which first-line vasoactive drug is the best choice for children with fluid-refractory septic shock? A prospective, randomized, blinded study of 120 children compared dopamine versus epinephrine in attempts to answer this debated question in the current guidelines for pediatric sepsis.
Bottom line: Dopamine was associated with an increased risk of death and healthcare–associated infection. Early administration of peripheral or intraosseous epinephrine was associated with increased survival in this population.
What Matters in Cardiac Arrest?
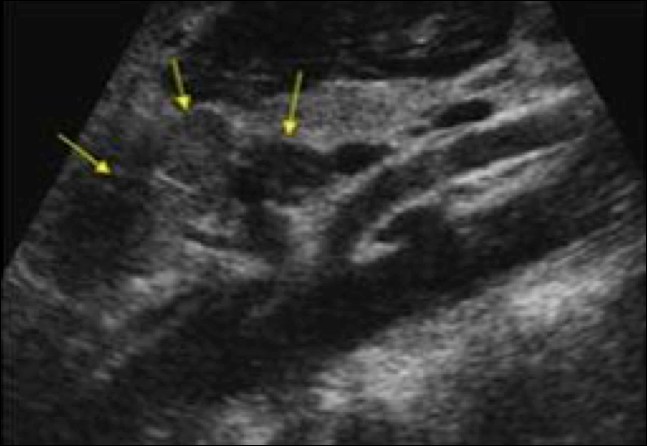
A 15 months old male with no past medical history, presenting with two days of decreased oral intake and decreased urine output. The exam was notable for minimal tenderness of abdomen. During an oral fluid challenge in the ED, the patient had a single episode of bilious vomiting. The ED physician ordered an ultrasound study and the results are shown below. What is the diagnosis?

Using 1.5 mg/kg or 2 mg/kg of IV ketamine led to less redosing compared to using 1 mg/kg IV.
Recently a review paper was published regarding the duration of observation in heroin overdose patients who received naloxone.
It made several conclusions regarding heroin overdose:
It should be pointed out that this is a review paper of limited number of articles with variable quality. Additionally, the clinical history of “heroin use” may be unreliable as fentanyl and novel synthetic opioids are also sold as “heroin.” Providers should exercise appropriate clinical judgement when caring for these patients.
It is well documented that when left to our own respiratory devices we will consistently over-ventilate patients presenting in cardiac arrest (1). A simple and effective method of preventing these overzealous tendencies is the utilization of a ventilator in place of a BVM. The ventilator is not typically used during cardiac arrest resuscitation because the high peak-pressures generated when chest compressions are being performed cause the ventilator to terminate the breath prior to the delivery of the intended tidal volume. This can easily be overcome by turning the peak-pressure alarm to its maximum setting. A number of studies have demonstrated the feasibility of this technique, most recently a cohort in published in Resuscitation by Chalkias et al (2). The 2010 European Resuscitation Council guidelines recommend a volume control mode targeting tidal volumes of 6-7 mL/kg and a respiratory rate of 10 breaths/minute (3).
https://images.radiopaedia.org/images/3173801/1ee24da1a6fe907a27d2bf20481174.jpg
Young toddler presents with left lower leg pain. What is the diagnosis??
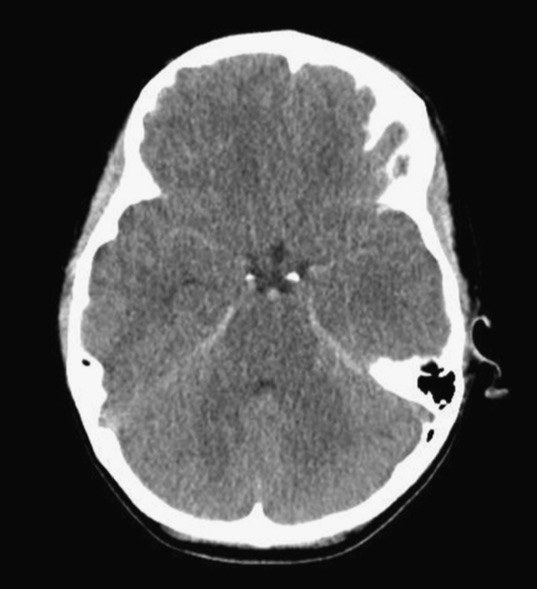
Patient found pulseless after submersion in water for 20 minutes. After ROSC, patient’s GCS was 3 and pupils are dilated and nonreactive.
It's Election Day in the US, so here are some interesting facts about Presidential causes of death:
George Washington likely died from epiglottitis on 12/14/1799
CLICK BELOW FOR MORE INTERESTING FACTS!
8 year-old female with no PMH who presents with concerns for "purple patches" popping up on her arm for 2-3 days. Stated that one appeared and then, the other one appeared 12 hours later. She denied any trauma whatsoever, history of easy bleeding/bruising and did feel safe at home. The rest of the review of systems was negative.
Patient said there was mild pain when the area was touched. The rest of the physical examination was normal.
What's the diagnosis? (Image below)

Do you have a patient with renal insufficiency who is in need of an anticoagulation bridge to warfarin? Subcutaneous unfractionated heparin (UFH) as an initial dose of 333 Units/kg subcutaneously followed by a fixed dose of 250 Units/kg (actual body weight) every 12 hours may be an alternative to admission for heparin infusion with monitoring.
As noted in a previous post, the FASH exam is the Focused Assessment with Sonography for HIV/TB. Below are typical ultrasound images of a positive FASH exam.
Peri-aortic lymph nodes- Multiple enlarged nodes, 97.1% specific for TB
Splenic lesions – multiple ‘punched out’ lesions

The effusions often have fibrous stranding
Submitted by Dr. Laura Diegelmann
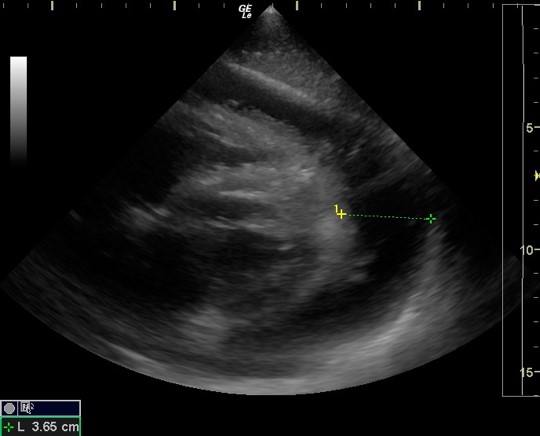
Dynamic LVOT Obstruction
30 year old female presents with a painful finger for 1 week. Finger exam showed the following. What is the diagnosis ?

Typically, empiric treatment for lobar community acquire pneumonia (CAP) in immunized < 5 year olds (preschool) is amoxicillin (45mg/kg BID or 30 mg/kg TID for resistant S. pneumoniae) for outpatient and ampicillin or ceftriaxone for inpatient. Additional coverage with azithromycin is typically recommended for school age and adolescent patients (>= 5 years), but not necessarily for younger children unless there is a particular clinical suspicion for atypical pneumonia with history, xray findings, or sick contacts.
However, in sickle cell patient with suspicion for acute chest syndrome, azithromycin is recommended for all ages groups, as atypical bacteria such as Mycoplasma are a common cause of acute chest syndrome in patients of all ages with sickle cell disease even young children. In a prospective series of 598 children with acute chest syndrome, 12% of the 112 cases in children less than 5 had positive serologic testing of M. pneumoniae (9% of all cases had M. pneumoniae) (Neumayr et al, 2003).
Recently, a retrospective study of unintentional buprenorphine/naloxone exposure among pediatric population was published. All patients were evaluated by toxicologists at the time of initial hospital presentation (or transfer) at the study center.
Bottom line
{kind=link}
{kind=link}