Tramadol has a reputation for being a safe, non-opioid alternative to opioids. Nothing could be further from the truth. Several blogs have published about the dangers of tramadol:
But what about seizure risk? Previous studies have been unable to confirm an increased seizure risk with therapeutic doses of tramadol (Seizure Risk Associated with Tramadol Use from EM PharmD blog). However, a new study refutes that premise.
22% of first-seizure patients had recent tramadol use!
This was a retrospecitve study without laboratory confirmation of tramadol intake. Nevertheless, it behooves us not to think of tramadol as a safer alternative to opioids. It is an opioid after all, and it comes with significant adverse effects.
Carbon monoxide (CO) is a colorless, odorless, tasteless toxic gas produced by incomplete combustion in fuel-burning devices and is a leading cause of poisoning morbidity and mortality.
Symptoms can be easily misinterpreted (e.g., headache, nausea, dizziness, or confusion) thus victims may not realize they are being poisoned.
CO detectors use an audible alarm and are effective in alerting potential victims of presence of CO. Some versions offer a digital readout of the CO concentration. Detectors are not a simple alarm level (as in smoke detectors) but are a concentration-time function.
In the UL 2034 Standard, Underwriters Laboratories specifies response times for CO alarms:
Current Occupational Safety and Health Administration permissible exposure limit for CO is 50 parts per million as an 8-hour time-weighted average concentration.
CO detectors have a limited lifespan of up to 7 years.
Forty percent of residential detectors studied failed to alarm in hazardous concentrations, despite outward indications that they were operating as intended.
CO detectors 10 years and older had the highest failure rates.
On a day when the 355th mass shooting this year in the USA occurred in San Bernardino, California, it seems appropriate to discuss gun violence.
A recently accepted publication in the American Journal of Medicine compared morality data from the USA to other high-income countries, and found the following:
The US homicide rates were 7.0 times higher than the aggregated rates of all other high-income countries.
The overall US suicide rate is average
Unintentional firearm deaths were 6.2 times higher in the US.
The overall firearm death rate in the US from all causes was 10.0 times higher.
Bottom line: As stated in the article: “The US has an enormous firearm problem compared to other high-income countries with much higher rates of homicide and firearm-related suicide.”
Mechanical Ventilation for Septic Patients in Resource-Limited Settings
Patient presents with right elbow pain after a fall. What's the diagnosis and what other injury should you look for?

Medial elbow pain is common among baseball pitchers and is also seen in other sports including football, javelin and gymnasts.
More than 97% of elbow pain in pitchers is located medially.
The ulnar collateral ligament of the elbow is an important structure in these patients.
http://www.aafp.org/afp/2014/0415/afp20140415p649-f3.jpg
While initially primarily seen in professional throwers, these injuries are now being seen in younger athletes.
Initially, patients may only note changes in stamina or strength of throws.
Later, they will note pain during the acceleration and follow through-phase of throwing
http://stlhealthandwellness.com/wp-content/uploads/2013/02/elbow03.jpg
The Valgus stress test for UCL deficiency is similar to the valgus test for the knee
https://www.youtube.com/watch?v=f6YvPSVk6G8
Treatment: splinting, ice, NSAIDs
Surgical indications: Failure of non-operative treatment with desire to return to same or higher level competition.
Ketamine has been the drug du jour for everything from agitation to pain, but status epilepticus?
Looking at the pathophysiology of seizures, they occur due to an imbalance between excitatory mechanisms (through glutamate at the NMDA receptors) and inibitory mechanisms (at GABA receptors). The mainstay for seizure treatment has been mostly potentiation of the inhibitory mechanisms, but why not inhibit the excitatory mechanisms at the NMDA receptors?
Ketamine is the only NMDA antagonist that has been investigated for refractory status epilepticus, mostly in retrospective small series, with only 3 prospective cohort studies, totaling to 162 patients (110 adults and 52 pediatrics). Variable results were recorded, from studies with complete response in all patients to complete treatment failure, with a total of 56.5% of the adult patients having electrographic response. The optimal bolus dose appears to be 1.5-4.5 mg/kg, with an infusion of up to 10 mg/kg/hour.
Bottom Line? Consider using ketamine in patients who are in refractory status - after benzodiazepines, a 2nd line agent (such as fosphenytoin, valproic acid or levetiracetam) and IV anesthetics have failed.
(NMDA: N-methyl-D-aspartate, GABA: -aminobutyric acid)
--The role of antibiotics in acute exacerbations of COPD remains controversial in many settings. However, a recent Cochrane review concludes that antibiotics have "large and consistent" benefit in ICU admissions [1]:
--However, patients on antibiotics had increased side effects, are at risk for increased drug-drug interaction (think azithromycin/levofloxacin), and the effect on multi-drug resistance is unclear.
--GOLD Guidelines are a bit more liberal with their recommendations for antibiotics [2], recommending antibiotics based on symptoms or in patients needing mechanical support.
--TAKEAWAY -- if your patient needs BiPAP or ICU, they should also get antibiotics!
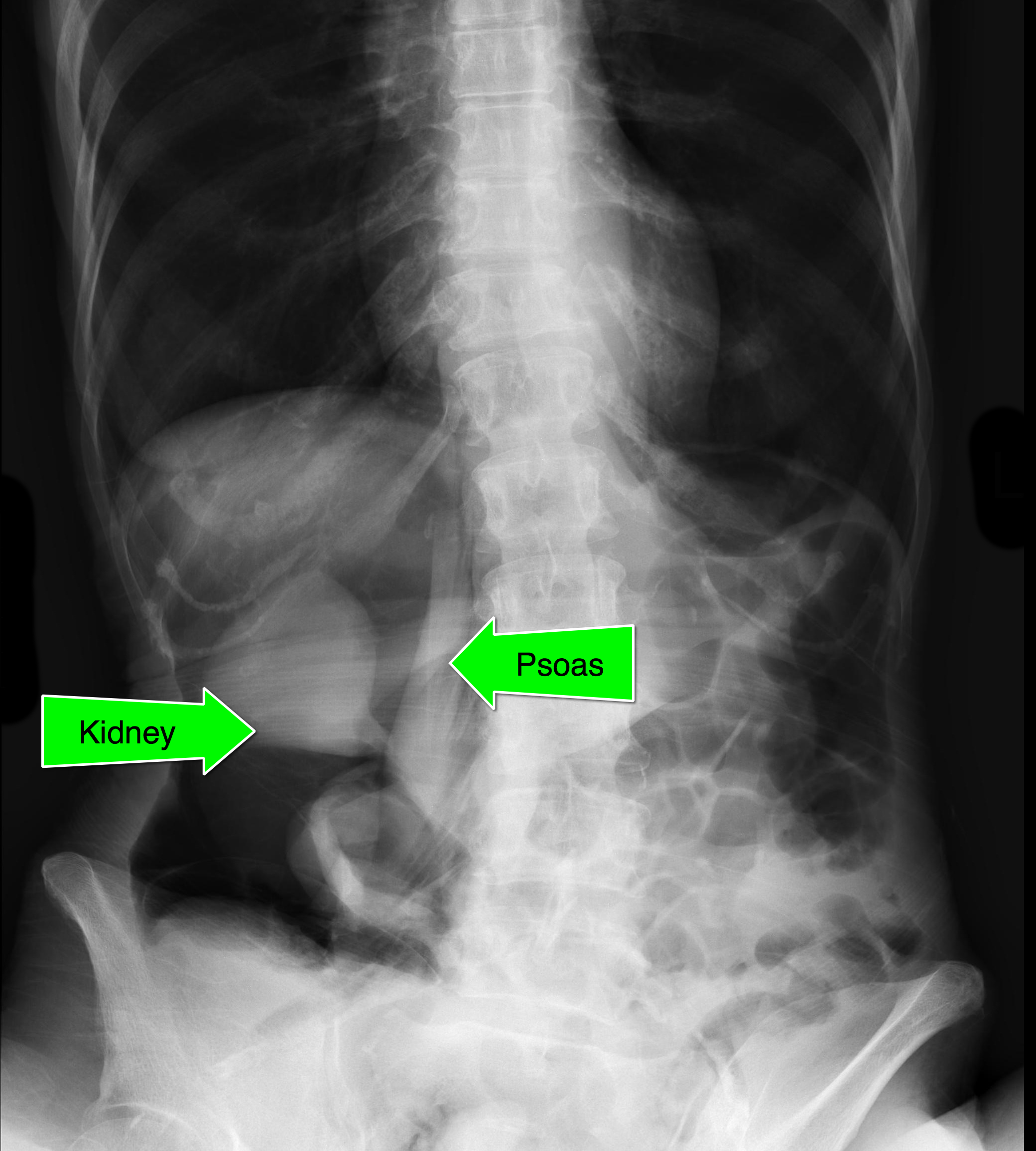
An elderly patient presents with a history of weight loss and chronic constipation. The abdominal Xray is shown below. What's the diagnosis?
This one is tricky so here's a hint: why is the right kidney and psoas muscle so well defined?

Steroids and Back Pain:
This pearl, https://umem.org/educational_pearls/2805/, by Dr. Corwell reported on the trail published in JAMA that showed that Steroid use does NOT help in the treatment of acute sciatica. But what about just general back pain. Do steroids help with that?
An article published in January in the Journal of Emergency Medicine, http://dx.doi.org/10.1016/j.jemermed.2014.02.010, reported on a randomized controlled trial of prednisone 50mg daily for 5 days versus placebo for the treatment of Emergency Department patients with Low Back Pain.
The study showed that at follow-up there was no difference between the groups in respect to pain, resuming normal activities, returning to work, or days lost from work. More patients in the prednisone group then the placebo group sought additional medical treatment (40% vs 18%).
CONCLUSION: The authors detected no benefit from oral corticosteroids in ED patients with musculoskeletal back pain, and it might actually increase their chance of returning for additional medical care. Just say NO to steroids in back pain.
Electronic cigarettes have been gaining popularity in the U.S. as a smokeless delivery system for nicotine. These devices require liquid nicotine (e-liquid) that are vaporized and inhaled (vaping).
E-liquid can have nicotine concentration as high as 100 mg/mL, which are diluted prior to use. When ingested in high concentration and in sufficient volume (1 vial = 15 mL) patients can develop significant nicotinic toxicity. Recently a case of cardiac arrest has been reported after ingesting two 15 ml vial (100 mg/mL).
Nicotine mimics the effects of acetylcholine (Ach) release by binding to nicotinic receptors located in:
Clinical manifestation of toxicity (similar to cholinergic toxidrome) is biphasic with early central stimulation followed by depression. (see table below)
|
| GI | Respiratory | Cardiovascular | Neurologic |
| Early (1 hr) | Nausea Vomiting Salivation Abdominal pain | Bronchorrhea Hyperpnea | Hypertension Tachycardia Pallor | Agitation Anxiety Dizziness Blurred vision Headache Hyperactivity Tremors Fasciculation Seizures |
| Late (0.5-4 hr) | Diarrhea | Hypoventilation Apnea | Bradycardia Hypotension Dysrhythmias Shock | Lethargy Weakness Paralysis |
Management: There is no specific antidote or reversal agent. The management of nicotine toxicity focuses on organ-specific dysfunction.
There are two main models of Emergency Medical Services (EMS) Systems
Franco-German
Anglo-American
Hook of Hamate Fracture
Rare (2% of all carpal fractures)
Mechanism usually direct blow from a stick sport (golf, hockey, baseball)
Presents with hypothenar pain and pain with gripping activities
Physical examination - local swelling and tenderness to palpation over hook of hamate
Diagnostic test - Hook of hamate pull test
https://www.youtube.com/watch?v=A-mjRnC1yWQ
XR - standard wrist series but add carpal tunnel view
http://openi.nlm.nih.gov/imgs/512/60/2904904/2904904_256_2009_842_Fig1_HTML.png
http://www.cmcedmasters.com/uploads/1/0/1/6/10162094/7851913.png?359
Not to be outdone by the recent FDA approval of Idarucizumab to reverse dabigatran, a new factor Xa reversal agent is under investigation. "Andexanet binds and sequesters factor Xa inhibitors within the vascular space, thereby restoring the activity of endogenous factor Xa and reducing levels of anticoagulant activity, as assessed by measurement of thrombin generation and anti factor Xa activity, the latter of which is a direct measure of the anticoagulant activity."
Design
Two parallel randomized, placebo-controlled trials (ANNEXA-A [apixaban] and ANNEXA-R [rivaroxaban]) were conducted in healthy vounteers to evaluate the ability of andexanet to reverse anticoagulation, as measured by the percent change in anti factor Xa activity after administration.
What they Found
Compared to placebo, andexanet significantly reduced anti-factor Xa activity, increased thrombin generation, and decreased unbound drug concentration in both the apixaban and rivaroxaban groups.
Application to Clinical Practice
Last month we discussed causes of serotonin syndrome including common ED medications such as cyclobenzaprine (Flexeril), tramadol (Ultram), metoclopramide (Reglan), and ondansetron (Zofran).
Let’s conclude this series and discuss how to treat serotonin syndrome:
This concludes our 3-part series on serotonin syndrome!
Risk factors for invasive candidal infections
If there weren't enough reasons to avoid opioids, here is another: opioids don't work for low back pain (LBP).
Objective
A well-done, double-blind, randomized controlled trial from JAMA set out to compare functional outcomes and pain at 1 week and 3 months after an ED visit for acute LBP among patients randomized to a 10-day course of (1) naproxen + placebo; (2) naproxen + cyclobenzaprine; or (3) naproxen + oxycodone/acetaminophen.
Intervention
Outcome
Neither oxycodone/acetaminophen nor cyclobenzaprine improved pain or functional outcomes at 1 week compared to placebo, and more adverse effects were noted.
Application to Clinical Practice
Among patients with acute, nontraumatic, nonradicular LBP presenting to the ED, avoid adding opioids or cyclobenzaprine to the standard NSAID therapy.
Designer drugs are structural or functional analogs of controlled substances produced to mimic pharmacological effects of the original compound while circumventing legal restrictions and detection on drug screens. Considered "legal highs" by the public, these highly potent drugs are produced in clandestine laboratories with no regulations for quality control or clinical testing for phamacological effects and thus present major threat to public health. Examples include synthetic hallucinogens (DOM: STP), opiates ( methylfentanyl:china white), stimulants (methamphetamine:crank, MDMA: ecstasy, cathinones:bath salts) and synthetic cannabinoids (spice).
The synthetic cannabinoids are the newest designer drugs and numerous cases of intoxication are being reported including some fatalties.Cannabinoids fall into 3 classes: endocannabinoids, phytocannabinoids, synthetic. Marijuana, the best known cannabinoid is plant derived and its psychoactive effects are mainly due to delta-9-tetrahydrocannabinol (THC) which binds with the endocannabinoid receptors CB1 and CB2 found throughout the central and peripheral nervous system and peripheral organs. The CB receptors interact with opiate receptors which is likely responsible for the analgesic effect.
Since 1984, the John Huffman research group at Clemenson University synthesized over 450 cannabinoid compounds for biomedical reseach known as "JWH compounds". These compounds hold great promise in the investigation of multiple diseases and development of new novel therapies. Over the last several years, these cannabinoid compounds began cropping up sprayed onto herbs marketed in colorful packets and sold on the internet, convienence stores, and head shops. Although clearly labeled as "not for human consumption" considered on the street as a legal alternative to marijuana.
Key Points:
- Anterior shoulder dislocations often require surgical management in young adults due to recurrence, but are less common in pediatric patients, particularly under age 10
- A study this year showed that 14-16 year olds are similar to 17-20 year olds in recurrence risk (around 38%- when non-operative management), and this is especially true of males.
- The recurrence rate is lower in the 10-13 age group, but there are also less dislocations in this group as well, making this group harder to assess
- Remember to consider both chronologic and bone age if you are deciding to refer a patient for outpatient surgery follow up, bone age is more accurate to determine healing and response to non-operative treatment
- Consider early referral for surgical management and counseling regarding recurrence risk in the 14-16 year age group after anterior shoulder dislocations