Digoxin-specific antibody fragments (Fab) are safe and indicated in all patients with life-threatening dysrhythmias and an elevated digoxin concentration. However, full neutralizing doses of digoxin-Fab are expensive and may not be required (not to mention cumbersome to calculate).
Based on pharmacokinetic modeling and published data, a new review suggests a simpler, more stream-lined dosing scheme as follows:
In imminent cardiac arrest, it may be justified to give a full neutralizing dose of digoxin-Fab.
In acute poisoning, a bolus of 80 mg (2 vials), repeat if necessary, titrated against clinical effect, is likely to achieve equivalent benefits with much lower total doses.
With chronic poisoning, it may be simplest to give 40 mg (1 vial) at a time and repeat after 60 min if there is no response.
Why is everyone obsessed about blood pressure management in stroke?
Greater than 60% of patients with stroke have elevated blood pressure, and 15% have a systolic blood pressure (SBP) greater than184 mmHg. That is more common in hemorrhagic stroke than ischemic stroke.
Whether it's an acute hypertensive response or a premorbid uncontrolled hypertension, it is likely to negatively affect the clinical course and neurological outcome.
Below is a suumary of the current guidelines for blood pressure management of stroke subtypes; for a more detailed summary of the guidelines, refer to the original article (below)
Ischemic stroke:
Lytic patients have a target SBP of <185mmHg, whereas nonlytic patients have a higher SBP target of <220mmHg
Hemorrhagic Stroke:
Non-aneurysmal hemorrhage patients with a SBP >180mmHg have a target SBP of <160 mmHg, whereas if their SBP was 150-220 mmHg then lowering it to 140 mmHg is safe. Patients with aneurysmal hemorrhage have a target SBP of <160mmHg
Goal-Directed Resuscitation During Cardiac Arrest
Focusing on high-quality CPR is by far one of the most effective methods to ensure your arrested patient has the best chance to survive. However, emerging evidence suggests that there are additional goals that we should try and accomplish during our resuscitation.
As we continue to move toward goal-directed resuscitation strategies, optimizing coronary perfusion pressure (CPP) may be our next target in “personalizing” the care we provide to those in cardiac arrest.
A recent AHA consensus statement recommended the following physiologic goals during cardiac arrest care:
Each of these variables can give the provider valuable feedback about how their patient is responding to their resuscitation. Some argue that the DBP target should be much higher (>35 mmHg), with the caveat that pharmacologic optimization can only occur once high quality CPR is confirmed. The goal should always be to minimize the use of epinephrine whenever possible!
Bottom Line: During your next cardiac arrest resus, consider using a goal-directed strategy by monitoring the patient’s CPP, DBP, & EtCO2 to determine the effectiveness of your resuscitation.
Suggested Reading
Follow me on Twitter @JohnGreenwoodMD
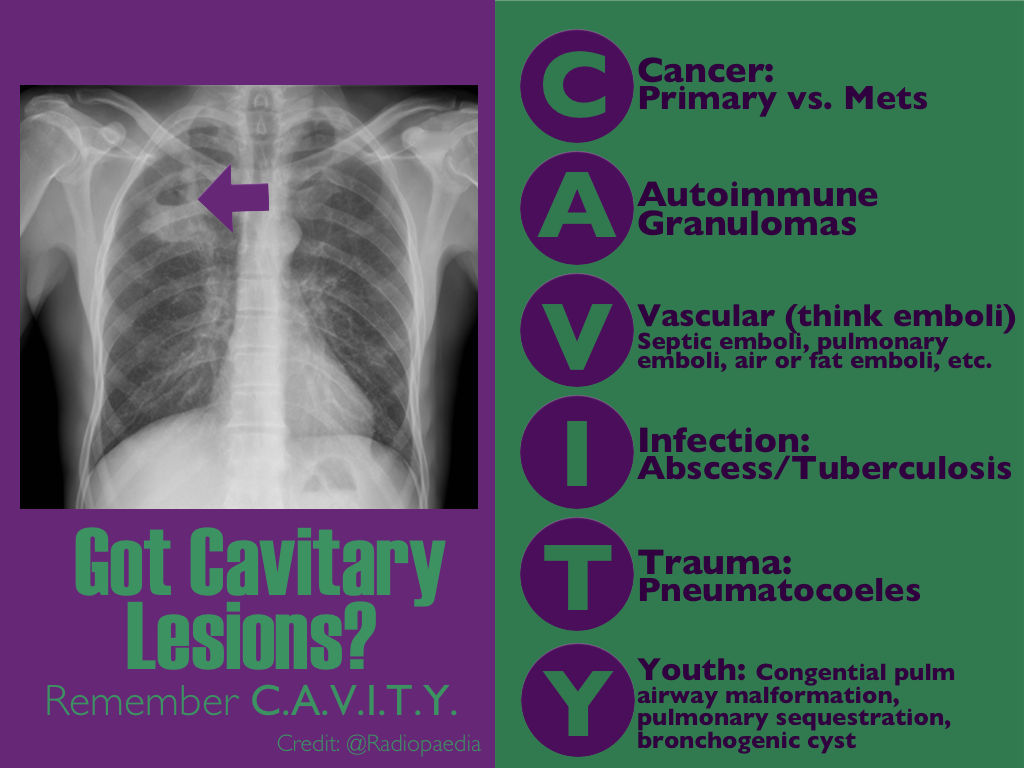
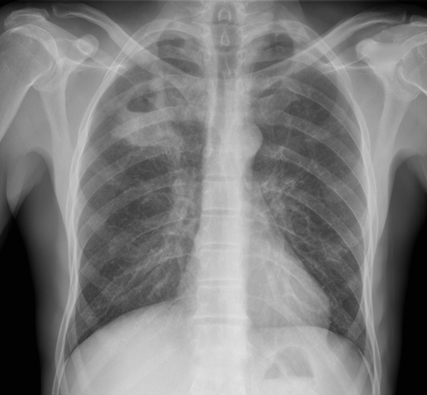
CXR shown below, what's the diagnosis? ...and name 3 differential diagnoses.
PARADIGM Shift in Heart Failure
- Angiotensin-converting enzymes inhibitors (ACE-I) are cornerstone for treatment of heart failure (HF) given the multiple trials which have shown their positive risk reduction in cardiovascular death.
- Studies looking at the effect of angiotensin-receptor blockers (ARBs) on mortality have been inconsistent; thus ARB's have been recommended as 2nd-line for those who have unacceptable side effects to ACE-I.
- A recent double-blinded RCT (PARADIGM-HF) ~8400 patients with class II-IV HF w/ ejection fraction <40% were treated with enalapril (standard therapy) versus novel therapy with neprilysin (neutral endopeptidase) inhibitor combined with an ARB.
- Primary outcomes were death from cardiovascular causes and hospitalization for HF; The RCT was ceased early (~27 months) because of an overwhelming benefit with the new agent.
- At study closure death occurred 26.5% in the standard group versus 21.8% in the novel group. The risk of HF hospitalization was decreased 21% with novel therapy.
- In early studies the use of a neprilysin inhibitor combined with an ARB has shown superior effects to current standard therapy (ACE-I), however long-term effects of this novel therapy are yet to be determined.
In May 2014, the U.S. Public Health Service released the first comprehensive clinical practice guidelines for PrEP.
Pre-Exposure Prophylaxis (PrEP) has been shown to decrease the risk of HIV infection in people who are at high risk by up to 92%, if taken consistently.
How this applies to the ED patient:
For more information, the CDC has a comprehensive website dedicated to PrEP.
Dysrhythmia-induced sudden death, termed "sudden sniffing death syndrome," is well described phenomena due to inhalant (chlorinated and aromatic hydrocarbon) abuse.
Common inhalants include:
Chlorinated hydrocarbons: Degreasers, spot removers, dry-cleaning agents
Fluorocarbons: Freon gas, deodarants
Toluene: Paint thinners, spray paint, airplane glue
Butane: Lighter fluid, fuel
Acetone: Nail polish remover
The common theory behind the syndrome is cardiac sensitization that increases susceptibility of the heart to systemic catecholamines (epinephrine, norepinephrine, etc). Usually, it occurs after an episode of exertion in that any excess catecholamine exposure causes irritability of the myocardium, resulting in dysrhythmias (V. fib, V. tach) and cardiac arrest.
If acute dysrhythmias is due to myocardial sensitization, sympathomimectis should be avoided. Beta-adrenergic antagonist can be used for the catecholamine-sensitized heart.
Hyperthermia can be defined as a core body temperature > 38.5ºC. In contrast to fever, the body’s temperature rises uncontrollably and the body is not able to dissipate the heat. There can be many causes of hyperthermia, including from environmental exposure.
There are two main environmental heat illnesses, heat exhaustion and heat stroke.
Heat exhaustion:
Heat stroke
Bottom line:
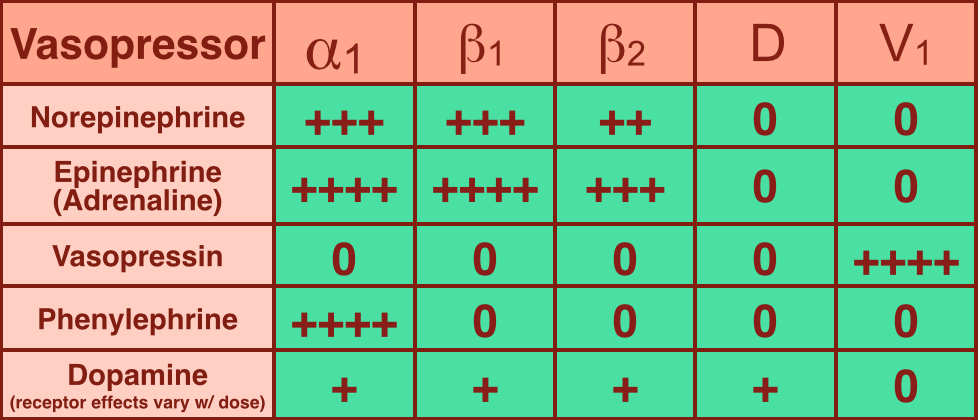
Vasopressors are used in shock-states to increase mean arterial pressure (MAP) and improve distal tissue perfusion. Additionally, some agents have effects on the heart to augment cardiac output.
Receptors that vasopressors work on include:
Norepinephrine (NE): excellent vasopressor for most types of shock and recommended as a first-line agent in the Surviving Sepsis Guidelines.
Epinephrine (a.k.a. Adrenaline): in several countries the first-line agent for shock (including sepsis).
You are scaning the liver with ultrasound and you see this. What's the diagnosis?
Sick Sinus Syndrome
- Sick sinus syndrome (SSS) is a cardiac conduction disorder characterized by symptomatic dysfunction of the sinoatrial (SA) node.
- SSS usually manifests as sinus bradycardia, sinus arrest, or sinoatrial block, and is sometimes accompanied by supraventricular tachydysrhythmias.
- Symptoms of SSS include: syncope, dizziness, palpitations, exertional dyspnea, fatigability from chronotropic incompetence, heart failure, and angina.
- Clinically significant SSS typically requires pacemaker implantation. Approximately 30% to 50% of pacemaker implantation in the United States list SSS as the primary indication.
- 2 large, prospective cohorts with an average follow-up of 17 years, observed the incidence of SSS increases with age, does not differ between men and women, and is lower among blacks than whites.
- Risk factors for SSS included greater BMI & height, elevated NT-proBNP level & cystatin C level, longer QRS interval, lower heart rate, hypertension, and right bundle branch block.
Some radiology pearls concerning ankle pain and fractures courtesy of David Bostick and Michael Abraham
Maisonneuve fracture – fracture of the medial malleolus with disruption of the tibiofibular syndesmosis with associated fracture of the proximal fibular shaft (http://radiopaedia.org/articles/maisonneuve-fracture)
When to look for high fibular fracture
Always look for avulsion fracture of 5th metatarsal styloid in patients with ankle pain and
no obvious fractures
Dans-Weber Classification – for lateral malleolar fractures (http://radiopaedia.org/articles/ankle-fracture-classification-weber)
Elevated intracranial pressure (ICP), defined as >20mmHg, is frequently encountered in patients with severe traumatic brain injury (TBI). A step-wise approach would include:
1. Analgesia and sedation: frequently forgotten.
2. Hyperosmolar agents: both hypertonic saline and mannitol can be used. Neither is superior.
3. Induced arterial blood hypocarbia using hyperventilation (must monitor for cerebral ischemia)
4. Barbiturates (last resort due to side effects)
5. Surgical:
a. CSF drain
b. Decompressive craniectomy: benefits challenged by the DECRA study
Stocchetti N, Maas AIR. Traumatic Intracranial Hypertension. N Engl J Med 2014; 370:2121-30.
Background
Data
What to do
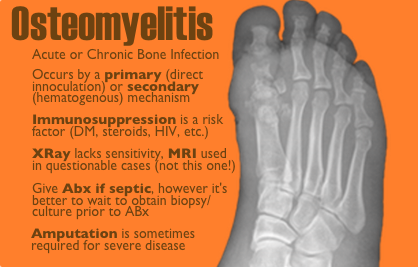
50 year-old female with diabetes complains of pain and discharge from a poorly healing wound. XRay below. What's the diagnosis?

GRACE Score
- The Global Registry of Acute Coronary Events (GRACE) is an international database tracking outcomes of patients presenting with acute coronary syndromes (ACS).
- GRACE score is calculated based on 8 variables: Age, HR, systolic BP, creatinine, killip class, ST-segment deviation on EKG, cardiac biomarkers, and cardiac arrest on admission.
- Several reports have shown that the GRACE score is a better predictor of clinical outcome (risk of death or the combined risk of death or myocardial infarction at 6 months) than the TIMI score.
- A recent study evaluated the relationship between GRACE score & severity of coronary artery disease (CAD) angiographically evaluated by Gensini score in patients with NSTE-MI.
- Results showed that the GRACE score has significant relation with the extent & severity of CAD as assessed by angiographic Gensini score.
- GRACE score was shown to be important both for determining the severity of the CAD and predicting death within 6 months of hospital discharge from NSTE-MI.
Patellar tendonitis aka jumpers knee
Activity related knee pain due to degenerative, micro injury rather than an inflammatory process
Up to 20% in jumping athletes
Anterior knee pain during or after activity
Bassett Sign:
a) Tenderness to palpation with knee in full extension (patellar tendon relaxed)
b) No tenderness with knee in flexion (patellar tendon tight)
E-cigarette popularity has increased and with that another possible source of toxicity. The most recent MMWR shows how e-cigarette use has increased over the past 5 years. The general toxicity involves nicotine toxicity with nausea, vomiting, eye irritation as the major sources of toxicity. Only one reported death where the nicotine reservoir was accessed and then injected IV in a suicide attempt.
There are some reports of asthma exacerbations but is more likely due to the vapor flavor and not the nicotine.
General Background:
Heat transfer is important to understand, especially when evaluating and treating someone who is hyperthermic or hypothermic. Are they really hot (or cold) from exposure, or is there an underlying metabolic or toxicological cause?
Mechanisms of Heat Transfer:
There are 4 main methods of heat transfer:
Bottom line:
When evaluation someone for hyper- or hypothermia from a potential environmental exposure, be sure to obtain the history about where they were found and the circumstances in which they were found. This can help you develop your diagnostic differential.