Abdominal pain in children can be just as frustrating as dizzy in the elderly. Your exam is targeted at quickly ruling out acute pathologies, but then what? The diagnosis is often functional gastrointestinal disorders, like the ever exciting constipation. Abdominal migraine (AM) is an additional entity to consider during your emergency department evaluation.
The following factors are often associated with AM:
- peak incidence at 7 years old
- paroxsymal, periumbilical abdominal pain lasting more than 1 hour
- family history of migraine
- episodes not otherwise explained by known pathology.
AM can be associated with headache, pallor, anorexia, photophobia, and fatigue. There are multiple theories on the pathogenesis, which can be found in the article cited below. If there is a known history, and the patient is presenting with an exacerbation, the treatment protocols for migraine headache may be employed with good success.
________________________________________________________________
Bottom Line:
AM is increasingly recognized as a source of recurrent abdominal pain in children. If other organic pathologies can be ruled out, this may be an important diagnosis to consider so your patient can get the appropriate follow up and outpatient management.
From 1960s to 1970s, physostigmine was routinely administered as part of the "coma cocktail." Since the publication of two cases by Pentel (1980) that resulted in asystole after administration of physostigmine in TCA poisoned patient, its use has declined significantly.
However, physostigmine still possess limited but clinically useful role in the management of patients with antimuscarinic/anticholinergic induced delirium.
Recently, a prospective observational study was performed in the use of physostigmine when recommended by a regional poison center.
In 1 year study period, physostigmine was recommended by a regional poison center in 125 of 154 patients with suspected antimuscarinic/anticholinergic toxicity.
common exposures were
57 of 125 patients received physostigmine per treating team.
Of the remaining patients,
Delirium control
Adverse events (physostigmine group vs. non-physo group) - no statistically significant difference.
Conclusion:
Physostigmine can safely control antimuscarinic/anticholinergic-induced delirium.
Legionella is an important cause of community-acquired pneumonia. It ranks among the three most common causes of severe CAP leading to ICU admission and carries a high mortality rate – up to 33%. Resulting from inhalation of aerosols containing Legionella species and subsequent lung infection, it is often associated with contaminated air conditioning systems, and other hot and cold water systems.
Recommended antibiotic regimens include a fluoroquinolone, either in monotherapy or combined with a macrolide (typically Levaquin +/- or Azithromycin).
A retrospective, observational study published in the Journal of Antimicrobial Chemotherapy in 2017 looked at 211 patients admitted to the ICU with confirmed severe legionella pneumonia treated with a fluoroquinolone vs a macrolide and monotherapy vs combination therapy. Combination therapy included fluoroquinolone + macrolide, fluoroquinolone + rifampicin, or macrolide + rifampicin.
Of these 211 cases, 146 (69%) developed ARDS and 54 (26%) died in the ICU. Mortality was lower in the fluoroquinolone-based group (21%) than in the non-fluoroquinolone based group (39%), and in the combination therapy group (20%) than in the monotherapy group (34%). In a multivariable analysis, fluoroquinolone-based therapy, but not combination therapy was associated with a reduced risk of mortality (HR 0.41).
Take Home Points:
-Remember, our usual blanket coverage with vanc + zosyn in the ED does not cover atypicals!
-Consider Levaquin instead of Azithro if there is clinical concern for Legionella PNA
-hyponatremia, abnormal LFTs may be clues in the appropriate context
Based in part upon Geriatric Emergency Department Guidelines, the American College of Emergency Physicians has initiated a Geriatric Emergency Department Accreditation Program. Emergency departments (EDs) can be accredited at one of three levels- Gold (Level 1), Silver (Level 2) and Bronze (Level 3). There are various aspects upon which and EDs’ level is determined, including nurse and physician staffing and education, appropriate policies and protocols, quality improvement activities, outcome measures, equipment and the physical environment.
Medical decision-making capacity refers to the patient’s ability to make informed decisions regarding their care, and emergency physicians are frequently required to assess whether a patient possess this capacity. Patients with acute or chronic neurological diseases (such as dementia) may lack this capacity, and this should be identified, especially in life-threatening situations. The patient must have the ability to:
communicate a consistent choice
understand (and express) the risks, benefits, alternatives and consequences
appreciate how the information applies to the particular situation
reason through the choices to make a decision
There are numerous tools that may help with this assessment, but none has been validated in the ED. Be careful of determining that the patient lacks capacity just because of the diagnosis they carry.
BONUS PEARLS:
Capacity is a fluid concept; a patient may have the capacity to make simple decisions but not more complex ones. Capacity may also change over time
Psychiatry consultation to determine capacity is not obligatory but may be utilized for a second opinion.
Volume Responsiveness, Carotid Ultrasound, and the PLR
ED visits for acute gout increased almost 27% between 2006 & 2014, a 26.8% increase
Presentation: Acute severe pain, swelling, redness, warmth.
Pain peaks between 12 to 24 hours and onset more likely at night
Quiet, calm period between flares vs other arthritic disorders
Signs of inflammation can extend beyond the joint
Normal to low serum urate values have been noted in 12 to 43% of patients with gout flares
Accurate time for assessment of serum urate is greater than 2 weeks after flare subsides
Most hyperuricemic individuals never experience a clinical event resulting from urate crystal deposition.
Gout flares may occasionally coexist with another type of joint disease (septic joint, psedugout),
A clinical decision rule has shown to be more accurate than clinical diagnosis (17 versus 36%)
*Male sex (2 points)
*Previous patient-reported arthritis flare (2 points)
*Onset within one day (0.5 points)
*Joint redness (1 point)
*First metatarsal phalangeal joint involvement (2.5 points)
*Hypertension or at least one cardiovascular disease (1.5 points)
*Serum urate level greater than 5.88 mg/dL (3.5 points)
Scoring for low (≤4 points), intermediate (>4 to <8 points), and high (≥8 points) probability of gout identified groups with a prevalence of gout of 2.2, 31.2, and 82.5 percent, respectively.
Consider supplementing your clinical decision with this in the future
Children with diabetic ketoacidosis (DKA) may have brain injuries ranging from mild to severe. The debate over the contribution from intravenous fluids towards poor neurologic outcomes has been ongoing for decades.
PECARN's large multicenter randomized, controlled trial examined the effects of the rate of administration and the sodium chloride content of intravenous fluids on neurologic outcomes in children with diabetic ketoacidosis may finally put the controversy to rest. There was no difference on significant neurologic outcomes based on the rate (fast vs slow) or concentration (0.9% vs 0.45%) of IV fluid administration.
Clinically apparent brain injury occurred in 12 of 1389 episodes (0.9%) of children in DKA.
Any change in the mental or neurological status of the patient should be concerning for life threatening edema and should be treated with mannitol 1g/kg IV bolus or hypertonic saline (3%) 5-10 mL/kg IV over 30 minutes.
Although not specifically a part of current recommendations due to lack of data, the AHA has previously recommended shifting upward on the sternum during CPR in the pulseless pregnant patient in order to account for upward displacement of the heart by a gravid uterus. Should the same be done for our obese patients?
Lee et al. performed a retrospective study that reviewed chest CTs to determine the location on the sternum that corresponded to the optimal point of maximal left ventricular diameter (OPLV), in both obese and non-obese patients.
They found that the OPLV was higher (more cranial) on the sternum for obese patients than for patients with normal weight, although 96% of obese patients' OPLV fell within 2cm of where the guidelines recommend standard hand placement should be, compared to a notable 52% in non-obese patients.
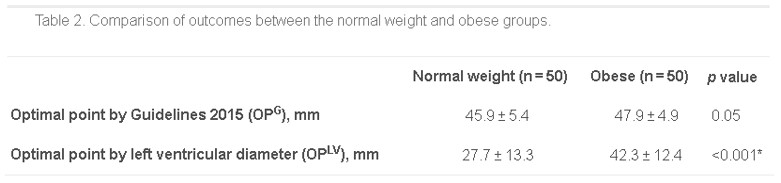
*as measured from the distal end of the sternum
Bottom Line: Radiographically, the location on the sternum that corresponds to optimal compression of the LV is more cranial in obese patients than in non-obese patients. It remains to be seen whether the recommendations for hand placement in CPR should be adjusted, but we may want to consider staying within 4cm of the bottom of the sternum in patients of normal weight.
Bottom Line:
Less than 1/2 of patients presenting to EDs and being diagnosed with concussion receive mild traumatic brain injury educational materials, and less than 1/2 of patients have seen a clinician for follow up by 3 months after injury.
In order to improve long term outcomes in patients with concusions please remember to provide the patient with approriate discharge instrucitons and strict instructions to follow up on their injury.
Full details of the article in JAMA can be found at https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2681571
The rate of occult bacteremia in infants 3 months to 24 months with a temperature higher than 40.5C was slightly higher when compared to those with a temperature higher than 39C.
363 infants (3 months to 24 months) with a fever > 40.5C who were well appearing were evaluated in this study. 4 were diagnosed with occult bacteremia (1.1%). 3 of these were caused by S. pneumoniae and 2 were fully immunized.
A larger sample size is needed to see if reconditions to include empiric blood cultures on this subgroup of patients is warrented.
Acutely agitated patients in the emegency room receive single or combination of benzodiazepine (lorazepam vs. midazolam) and antipsychotic (e.g. haloperidol) agents. Recently, use of ketamine has also been advocated to sedate agitated patients.
A recently published article compared IM administration several medications to treat acutely agitated patients in the ED. According to established protocol, each medication was administered in predetermined 3 week blocks:
Results
N=737 with median age of 40 years, 72% men.
Midazolam resulted in greater proportion of patients with "adequate" sedation (altered mentatl status scale <1) compared to antipsychotics at 15 min post administration. Among antipsychotics, olanzapine resulted in greater proportion of patient with sedation.
Adverse effect were limited
Conclusion:
Midazolam 5 mg IM achieve more effective sedation at 15 min in agitated ED patients than antipsychotics.
Bottom Line: Consider obtaining neuroimaging in patients presenting with syncope only if clinical features suggest probable neurological syncope.
Syndesmotic sprain aka a “high ankle sprain”
Ankle injuries make up almost 30% of the injuries in professional football
High ankle injuries make up between 16 and 25% of these injuries in the NFL (lateral most common)
10% in general population
In comparison to lateral ankle sprains, high ankle sprains result in significantly more missed games, missed practices and required a longer duration of treatment
Anatomy: The syndesmosis comprises several ligaments and the interosseous membrane
Mechanism: External foot rotation with simultaneous rotation of the tibia and fibula.
Can lead to a Maisonneuve fracture
Injuries 4x more likely in game setting than practice
A positive proximal squeeze test significantly predicts missed games and practices compared to those without.
https://www.youtube.com/watch?v=ThiW_9m7cFM
Although conjuncitivitis outside of the neonatal period is commonly caused by viruses, there are times when antibiotics are warranted due to bacterial infections, such as conjuncitivits-otitis syndrome.
Bottom line: Every patient with conjunctivitis should have an examination of his/her TMs, as your management may change.
Older patients are less likely than their younger counterparts to mount a fever in response to an infection. One explanation is that their basal temperature is lower. Some experts suggest redefining fever in older patients to match this decrease of 0.15C per decade. Therefore, your 80 year old patient would be considered “febrile” if their temperature is above 37.3C, rather than the traditional 38C.
Steroids induce leukocytosis through the release of cells from bone marrow and the inhibition of neutrophil apoptosis. This effect typically occurs within the first two weeks of steroid treatment.
Leukocyte elevation is commonly used in the diagnosis of septic patients; however, this can be hard to discern in patients on concomitant steroid therapy.
A retrospective cohort study of adult patients presenting with fevers and a diagnosis of pneumonia, urinary tract infection, bacteremia, cellulitis, or COPD exacerbation was conducted to determine the maximal level of WBC within the first 24h of admission between patients on acute, chronic, or no steroid treatment.
Results: maximal WBC levels (p< 0.001)
· Acute steroid therapy: 15.4 ± 8.3 x 10 9/L
· Chronic steroid therapy: 14.9 ± 7.4 x 10 9/L
· No steroid therapy: 12.9 ± 6.4 x 10 9/L
An increase in WBC of 5 x 10 9/L can be found in acute and chronic steroid use when presenting with an acute infection and fever.
Exertional rhabdomyolysis (ER)
The warm weather is here and with it comes an increased risk of ER
Risks include the intensity, duration and types of exercises performed
One of the biggest risks is the exercise experience of the participants, both in those with little to no experience and in those experienced athletes less trained than their counterparts.
Multiple case reports find that intense novel exercises early in the preseason before getting acclimatized and “in shape” carry great risk to the participant. These can be summarized as “too much, too soon, too fast.”
Coaches need to be educated about this and be prepared to detect and effectively handle ER through an emergency action plan.
-Conditioning workouts need to be phased in rather than start at maximum intensity on day one.
Eccentric exercises appear worse than concentric exercises.
Has been seen in almost all sports, ranging from swimming to golf.
It’s not just preseason football!
High humidity and high temperature environments increase the likelihood of ER
Males are more vulnerable to ER than females
Increased risk with sickle cell trait and glycogen storage diseases
Multiple drugs may increase individual risk including alcohol, cocaine, amphetamines, MDMA and caffeine.
Implicated medicines include, salicylates, neuroleptics, quinine, corticosteroids, statins, theophylline, cyclic antidepressants and SSRIs