Bottom line: In the 2023 updated Clinical Practice Guideline, the American Burn Association recommends 2ml/kg/%TBSA (for burns >20% TBSA)as initial starting point for fluid administration in the first 48 hours, guided by clinical factors with consideration of supplemental albumin to limit fluid administration. Fresh frozen plasma should be considered in the context of a clinical trial. Vitamin C and advanced hemodynamic monitoring are not recommended as they have not demonstrated improved outcomes.
Summary: Burn care has a paucity of high-quality research about some of the fundamental questions for resuscitation. The American Burn Association since 2010 has endorsed fluid volumes for patients with >20% TBSA (i.e. those predicted to develop burn shock) from 2ml/kg/%TBSA to 4ml/kg/%TBSA as a starting point for fluid resuscitation. Further clinical studies since then have demonstrated that lower volumes of fluid targeting urine output and other physiological variables are effective without demonstrating clear improvement in patient centered outcomes. Further adjuncts such as albumin or fresh frozen plasma have demonstrated reduced fluid administration but no improvement in patient-centered outcomes. While “fluid creep” is increasingly recognized, demonstrating benefits in clinical trials will likely remain elusive as overall practice continues to shift towards less fluids and the adjunctive use of colloid will likely continue to expand. In addition to ABA CPGs and resources, the Joint Trauma System also has several useful resources for burn care.
Sources:
https://doi.org/10.1093/jbcr/irad125
https://jts.health.mil/assets/docs/cpgs/Burn_Care_11_May_2016_ID12.pdf
Here are three good resources to learn about a soft tissue injury seen in high velocity blunt trauma patients called Morel-Lavallee lessions.
“Morel Lavallee lesions are soft tissue injuries seen in high-velocity trauma and are usually associated with underlying fractures of the pelvis, acetabulum, or proximal femur. Often these injuries are not immediately diagnosed due to the distracting concomitant bony injuries. However, identification of such injuries is important as they may pose as an independent risk factor for surgical site infection. The clinical findings include soft tissue swelling, bruise/ ecchymosis, fluctuance, and compressibility in the swelling. The diagnosis is usually established on physical examination, however, radiological investigations including ultrasonography and CT might help. The management options include nonoperative treatment, percutaneous aspiration, and open debridement.” 1
“Morel-Lavallée lesions are often the result of skin and subcutaneous tissue quickly tearing away from the underlying fascia. This allows a range of fluids to fill the space in the form of hemolymphatic masses. The two most common sites are the prepatellar plate of the knee and the lateral fascia of the hip.” 2
“ML lesion is often undiagnosed during initial presentation of a trauma patient, and emergency physicians and trauma surgeons should be aware of the possibility of occurrence of this injury. MRI is the imaging modality of choice, and the presence or absence of a capsule is an important imaging finding that guides appropriate therapy. Early diagnosis and management will help prevent long-term morbidity and complications in these patients.”3
BACKGROUND
EMS systems differ in staffing and composition. The Japanese model utilizes “doctor cars” which bring a physician and nurse to the scene of a critical patient encounter. Personnel on the “doctor cars” are able to perform advanced therapies such as REBOA, finger thoracostomy, and chest tube thoracostomy. As physician EMS fellowships continue to expand in the United States, it is helpful to examine the utility of physician response incorporated into prehospital emergency care.
THE STUDY
A nationwide retrospective cohort study including over 370,000 patients examined the impact of Japan “doctor cars” upon in hospital survival. Doctor cars responded to 2361 trauma patients, and traditional Ground Emergency Medical Services (GEMS) units cared for 46,783 trauma patients. The study’s primary outcome was survival to discharge.
The adjusted odds ratio for survival was significantly higher in the exposure group served by the doctor cars. The study suggests that there may be a role for augmenting ground EMS personnel in the response to critical injuries. Via logistic regression, the study controlled for multiple other variables such as age, sex, prehospital vital signs, out of hospital time, and injury severity score (ISS).
BOTTOM LINE
This study is far from definitive but contributes to a growing body of literature addressing how EMS physicians integrate into prehospital systems.
Settings: systemic review and meta-analysis
Participants: 2 RCTs, 21 observational studies. Fifteen studies were published between 2020-2023.
There was a total of 25721 patients with septic shock
Outcome measurement: Primary outcome was short-term mortality (ICU, hospital, 28-day, 30-day). Secondary outcomes included ICU LOS, Hospital LOS, time to achieve MAP > 65 mm Hg,
Study Results:
Composite outcome of short term mortality:
Secondary outcome:
Discussion:
Conclusion:
More and more studies, although a RCT is still necessary, are showing that early initiation of vasopressor within 1-6 hours of septic shock would be more beneficial to patients with septic shock.
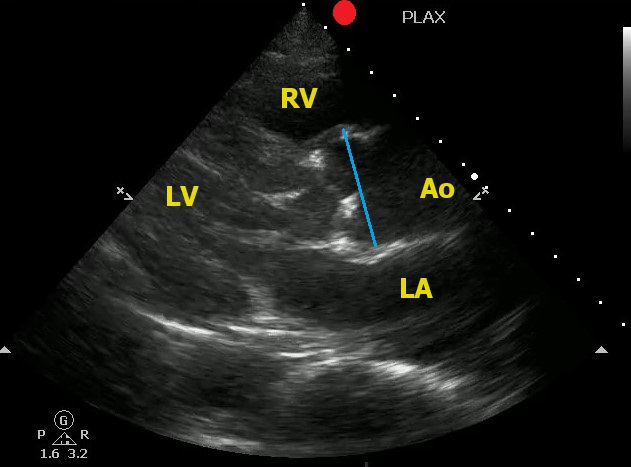
Point-of-Care Ultrasound can help to identify signs of thoracic aortic dissection.
One view to help in your assessment is the Parasternal Long Axis View.
To correctly measure the aortic root:
Here is an example of an aortic root aneurysm:
A retrospective study of 2 years of data from 24 trauma centers looking at end tidal CO2 as a predictor of mortality in trauma patients found:
"A total of 1,324 patients were enrolled. ETCO2 was better in predicting mortality than shock index (SI) and systolic blood pressure (SBP). Prehospital lowest ETCO2 , SBP , and SI were all predictive of Mass Transfusion."
Another data point to consider when setting up trauma triage protocols and looking for patients who will require intensive interventions early.
The Bottom Line: Investigators studying the use of a pre-intubation checklist versus "usual care" found no differences in important outcomes such as oxygen saturation and first pass success. However, the study was conducted as a part of a larger study, was unblinded, and not well controlled.
The investigators who conducted the multicenter CHECK UP trial, a study of head up intubation in ICU patients, reviewed the care of 262 ICU patients who were intubated. Some intubation attempts were guided by a pre-intubation checklist and some were not. The authors found no difference between the groups in lowest SPO2, number of intubation attempts, etc. However, the study was unblinded and largely observational. In many cases, the elements of a checklist had been incorporated into routine practice.
Take Home Point: While the authors found no differences in outcomes, this study does little to prove or disprove the value of pre-intubation checklists. Not only was the study essentially uncontrolled, the untoward events being studied are unusual in the hands of experienced clinicians.
Comment: Pre-procedural checklists make intuitive sense to me. They help us to avoid cultural drift. I am certainly not ready to abandon the use of a pre-intubation checklist based upon this study
Since Christmas is coming up, let's talk about Hemophilia A (factor VIII deficiency) and Hemophilia B (factor IX deficiency, also known as Christmas disease)
Deficiencies in Factors VIII and IX are the most common severe inherited bleeding disorders.
Pathophysiology:
Clinical Manifestations:
Lab findings and diagnosis
Genetics
Classification
trauma to induce bleeding
Treatment
Summary:
Since Christmas is coming up, let's talk about Hemophilia A (factor VIII deficiency) and Hemophilia B (factor IX deficiency, also known as Christmas disease)
Deficiencies in Factors VIII and IX are the most common severe inherited bleeding disorders.
Pathophysiology:
Clinical Manifestations:
Lab findings and diagnosis
Genetics
Classification
trauma to induce bleeding
Treatment
Summary:
Hot off the NEJM press, published November 11, 2023:
Restrictive or Liberal Transfusion Strategy in Myocardial Infarction and Anemia (Carson, Brooks, Hebert, et al Myocardial Ischemia and Transfusion (MINT) Investigators)
3504 pateints were included in this study. A primary-outcome event occurred in 295 of 1749 patients (16.9%) in the restrictive-strategy group and in 255 of 1755 patients (14.5%) in the liberal-strategy group. More specifically, death occurred in 9.9% of the patients with the restrictive strategy and in 8.3% of the patients with the liberal strategy; myocardial infarction occurred in 8.5% and 7.2% of the patients, respectively.
Conclusions from the study: Liberal transfusion strategy did NOT significantly reduce the risk of recurrent MI or death at 30 days.
A chart review of 1300 patients over age 65 admitted to the trauma service, arrived as a trauma activation, or had an injury severity score over 12 over a 6 year period looking at 30 day mortality found:
"five factors associated with increased 30-day mortality in older trauma patients: GCS < 15, ISS > 15, age ≥ 85 years, anticoagulation, and multimorbidity."
Fall from standing was the leading cause of trauma
Again, fragility is the index we should be using, not age alone. This study is limited in its retrospective chart review nature. Prospective research in the area of geriatric trauma is needed. Until then, assess those over age 65 for risk factors associated with fragility and treat accordingly.
This retrospective study looked at trauma patients over age 65 and divided them into age ranges 65-80 (geriatric) and 80 plus (super-geriatric). They then looked at mechanusm of injury, mortality, interventions,etc. What they found was ages 65-80 were more likely to be injured in motor vehicle crashes vs. falls for those over 80. Those over 80 received less interventions including hemmorhage control surgery and had much higher levels of withdrawal of care.
This study highlights that the geriatric population is not as a monolithic group over age 65, but more nuanced by various age ranges over 65. Research going forward should be adjusted to these nuanced age ranges. Out treatment approaches should be adjusted in geriatric vs. super-geriatric patients as well.
A recently published study of ED APPs, residents, attendings, and nurses attempted to assess clinician's perspectives on how ED boarding impacts ED staff and patients. Authors performed a survey followed by focus group sessions to obtain qualitative insignts from participants.
All respondents associated boarding with feelings of burnout and self-reported poor satisfaction with communication and the process of boarding care.
Several key themes emerged which are outlined below:
This publication highlights the negative workforce and patient safety effects of ED boarding. It amplifies the voices of our colleagues who work towards change to improve both the health of our wrokforce as well as that of our patients and the communities that we serve.
Acute bronchiolitis (AB) is a common cause of respiratory tract infections in infants. A recent study looked at the application of Point-of-Care Lung Ultrasound (LUS) in infants <12 months who presented with symptoms of AB.
They scored infant lungs using a cumulative 12-zone system. With the below scale:
0 - A lines with <3 B lines per lung segment.
1 - ≥3 B lines per lung segment, but not consolidated.
2 - consolidated B lines, but no subpleural consolidation.
3 - subpleural consolidation with any findings scoring 1 or 2.
They found that infants with higher LUS scores had increased rates of hospitalization and length of stay.
Here are some tips for ultrasounding a pediatric patient:
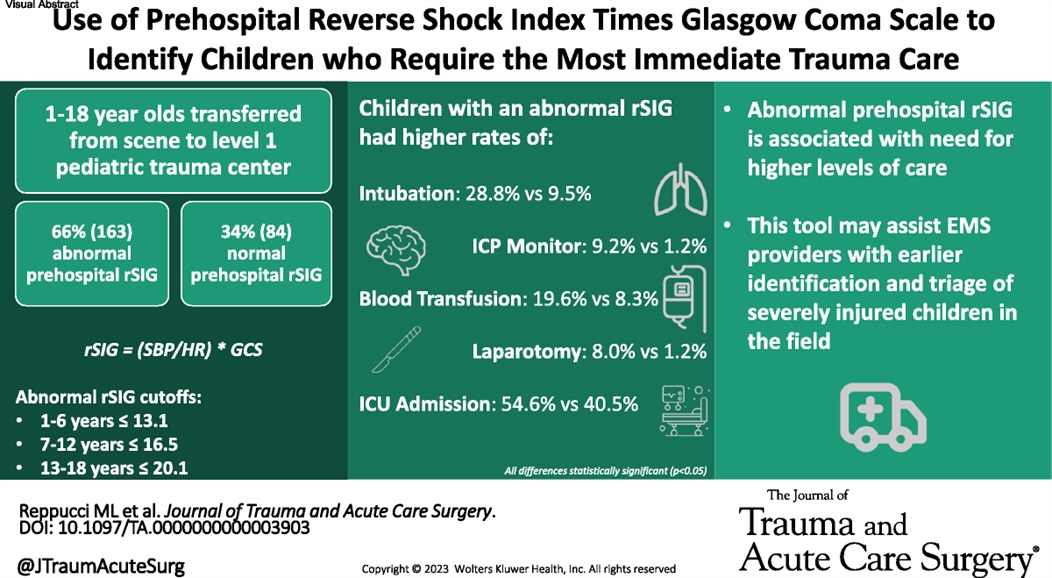
This small study suggests using reverse shock index times the Glasgow Comma Scake score may give a prognostication on pediatric trauma severity and resource utilization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}