A recent review identified 5 key points to consider when prescribing fluids.
Definition: An episode that is characterized by some combination of apnea, color change, change in muscle tone, choking, gagging, or a fear in the observer that the infant has died.
DDx: VAST!
- GERD is by far the most common underlying etiology
- Do NOT forget about child abuse
Workup: Dependent on your Hx/PE (Take into account the child’s age (<30 days or h/o prematurity), existence of prior ALTE episodes, general appearance, etc.)
One study showed the concordance of initial working to discharge diagnosis of GERD was 96%, and non-concordant diagnoses evolved within 24 hours
Dispo: The easy part! ADMIT!
Even well-appearing children with a “benign” diagnosis like GERD have been shown to benefit from admission. And there is a high likelihood that ALTE’s from a serious cause are likely to recur within 24hours.
A recent study looked at 176 infants who presented to the ED with an ALTE over a 5 year period. Essentially all were admitted.
Conclusion: The risk of subsequent mortality in infants presenting ALTE is substantial, and we should consider routine admission for all of these patients.
A recent article was published in the Journal of Medical Toxicology reviewing the use of sodium acetate for treatment of overdoses and poisonings.
Acetate is metabolized to bicarbonate, causing a net increase in cations; this increased strong anion difference leads to alkalemia.
It has been used to treat acidosis in uremia, diarrhea, and in trauma patients.
Although no studies have been conducted using sodium acetate as an antidote, if bicarbonate is unavailable this is a viable option for management of salicylate overdose, and for qrs widening or arrhythmias due to overdoses.
Sodium acetate, if given rapidly (in animals and hemodialysis patients), causes myocardial depression, hypotension, and hypopnea.
The bolus dose should be given as 1-2 mEq/L given over 15-20 minutes. For the maintenance infusion, dilute 150 mEq diluted to 1 L in dextrose 5%, infuse at 2X the maintenance rate.
It must be diluted in dextrose 5% and NOT normal saline.
General Information:
As of July 30th, 2013, there have been 378 cases of Cyclospora infection from multiple states in the US. Cyclospora is most common in tropical and sub-tropical regions, and is spread via fecal-oral route. While the cause of the most recent outbreak is unknown, outbreaks in the US are generally foodborne.
Clinical Presentation:
- Symptoms usually begin 7 days after exposure
- Watery diarrhea, cramping, bloating, nausea, fatigue, increased gas, vomiting, low grade temperature
- Can persist several weeks to > 1 month
Diagnosis:
- Concentrated Stool Ova and Parasites— viewed under modified acid fast or fluorescence microscopy (labs can submit photos to the CDC for “telediagnosis”)
Treatment:
- TMP-SMX DS one tab po bid x7-10 days
- No effective alternate for failed treatment or sulfa allergy
- Most will recover without treatment but S/S can persist for weeks to months
Bottom Line:
Consider Cyclospora as a cause of prolonged diarrheal illness, treat with TMP-SMX.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Elderly patient who originally presented for severe pancreatitis now intubated for worsening hypoxemia. CXR is shown below, what's the diagnosis?

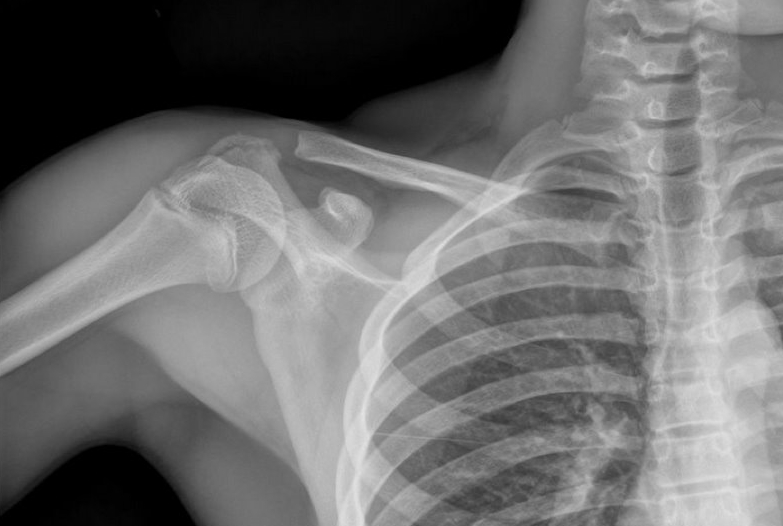
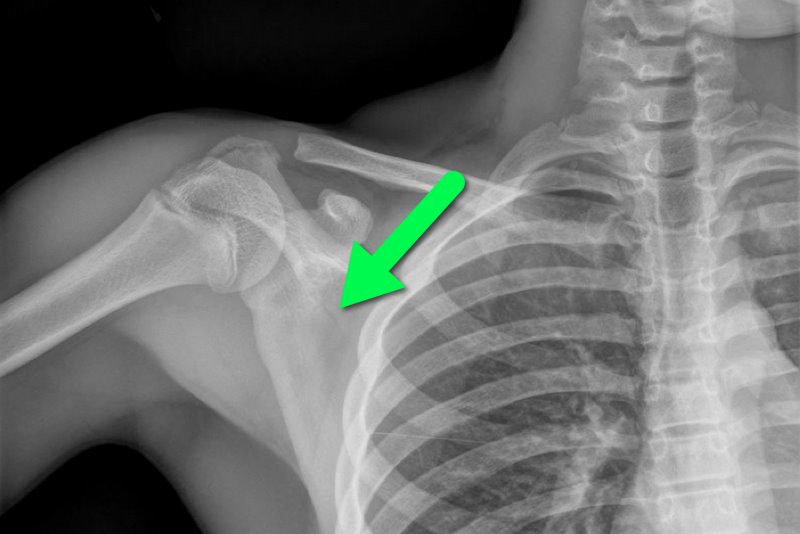
13 year-old female fell on right shoulder while catching a rebound during a basketball game. The patient is holding her arm in adduction and has exquisite scapular tenderness on exam. What’s the next step in management? …oh, and what’s the diagnosis?
Tight glycemic control (HbA1C<7%) has previously been recommended in CAD based on data from the United Kingdom Prospective Diabetes Study (UKPDS)
A recent study (JACC) evaluated the relationship between glycemic control, cardiovascular disease (CVD) risk, and all-cause mortality
Patients with a mean HbA1C 7-7.4% were compared to those with mean HbA1C <6%; tight glycemic control had a 68% increased risk of CVD hospitalization
Lenient HbA1C>8.5% also had significantly higher risk
CVD risk and all-cause mortality is greater with both aggressive and lax glycemic control and the optimal reference range may lie between 7-7.4%
Dupuytren disease is a nodular thickening and resultant contraction of the palmer fascia.
Increased in those of Northern European dissent.
One or more painful nodules located near the distal palmer crease.
Over time may result in flexion at the MCP joint.
Most commonly affects the ring finger.
Sensation is normal.
Over time affects ADLs
Tx: night splints and surgery
Cringing at the thought of sewing up another screaming 2 year old?
Consider intranasal fentanyl.
Who: Young, otherwise healthy pediatric patients undergoing minor procedures (laceration repair, fracture reduction/splinting, etc...)
What: Fentanyl (2mcg/kg)
When: 5 minutes pre-procedure
Where: Intranasal
Why: More effective than PO, less invasive than IV while being equally efficacious.
How: Use an atomizer, splitting the dose between each nostril.
General Information:
· Caused by the ameboflagellate Naegleria Fowleri
· Case fatality rate is estimated at 98%
· Commonly found in warm freshwater environments such as hot springs, lakes, natural mineral water, especially during hot summer months
· Incubation period 2-15 days
Relevance to the EM Physician:
· Clinical presentation: resembling bacterial meningitis/encephalitis
· Final diagnostic confirmation is not achieved until trophozoites are isolated and identified from CSF or brain tissue
· Treatment: Amphotericin B
Bottom Line:
· History of travel to tropical areas or exposure to warm or under-chlorinated water during summer time should raise the suspicion for Naegleria Fowleri. The amoeba is not sensitive to the standard meningitis/encephalitis therapy and amphotericin B must be added to the treatment regimen.
University of Maryland Section of Global Emergency Health
HIV, ART, and the ICU
A 3 year-old boy was attacked by a dog and sustained the injury below. Name one injury that should be strongly considered (Hint: there are several)

Treatment of Severe Hypothyroidism
We do not see patient's with severe hypothyroidism often, but it is important that they be treated aggressively. Some treatment pearls are
Lactate is commonly used in the adult ED when evaluating septic patients, but there is a lack of literature validating its use in the pediatric ED. Pediatric studies have suggested that in the ICU population, elevated lactate is a predictor of mortality and may be the earliest marker of death.
A retrospective chart review over a 1 year period showed that one elevated serum lactate correlated with increased pulse, respiratory rate, white blood cell count and platelets. Serum lactate had a negative correlation with BUN, serum bicarbinate and age. Elevated lactate levels were higher for admitted patients. However, the mean serum lacate level was not statistically different between those diagnosed with sepsis and those that were not.
The study included 289 patients less then 18 years who had both blood cultures and lactate drawn. This community hospital had a sepsis protocol in place that automatically ordered a lactate with blood cultures. Only previously healthy children were included.
The study is limited by its small sample size and overall low lactate levels. Despite having a protocol in place, only 39% of patients who had blood cultures drawn had lactate levels available for analysis. The mean serum lacate in this study was 2.04 mM indicating that the study population may not have been sick enough to determine mortality implications. There were no serial measurements.
Bottom line: Consider measuring serum lacate in your pediatric patient with suspected sepsis. Pediatric ICU literature does suggest that an serum lactate as low as 3mM is associated with an increased mortality in the ICU.
The internet has become a wealth of information and some books have now gained internet noteriety. A chemist and author of the book - TIKHAL: Tryptamines I Have Known and Loved is an excellent example.
Tryptamines include drugs like LSD and alpha-methyltryptamine (AMT). Vivid visual hallucinations and serotonin agonism, these drugs were glamorized by this author. He would synthesize a tryptamine and then "taste it". Take a look at the link below where he first describes the biochemical synthesis he performed then describes his dose response effect when he tried the drug.
If you run into a drug or slang term in the ED you are not familiar with, the website www.erowid.org will likely have the translation.
http://www.erowid.org/library/books_online/tihkal/tihkal48.shtml
COPD treatment guidelines (e.g., GOLD) recommend 10-14 days of steroid therapy following a COPD exacerbation to prevent recurrences; the supporting data is weak.
A recent noninferiority trial (here) compared patients with a severe COPD exacerbation who received either a 5-day course (n=156) or 14-day course (n=155) of prednisone 40mg.
The results were:
What you need to know:
Bottom-line: 5 days of prednisone may be as effective as 14-days for COPD exacerbations.
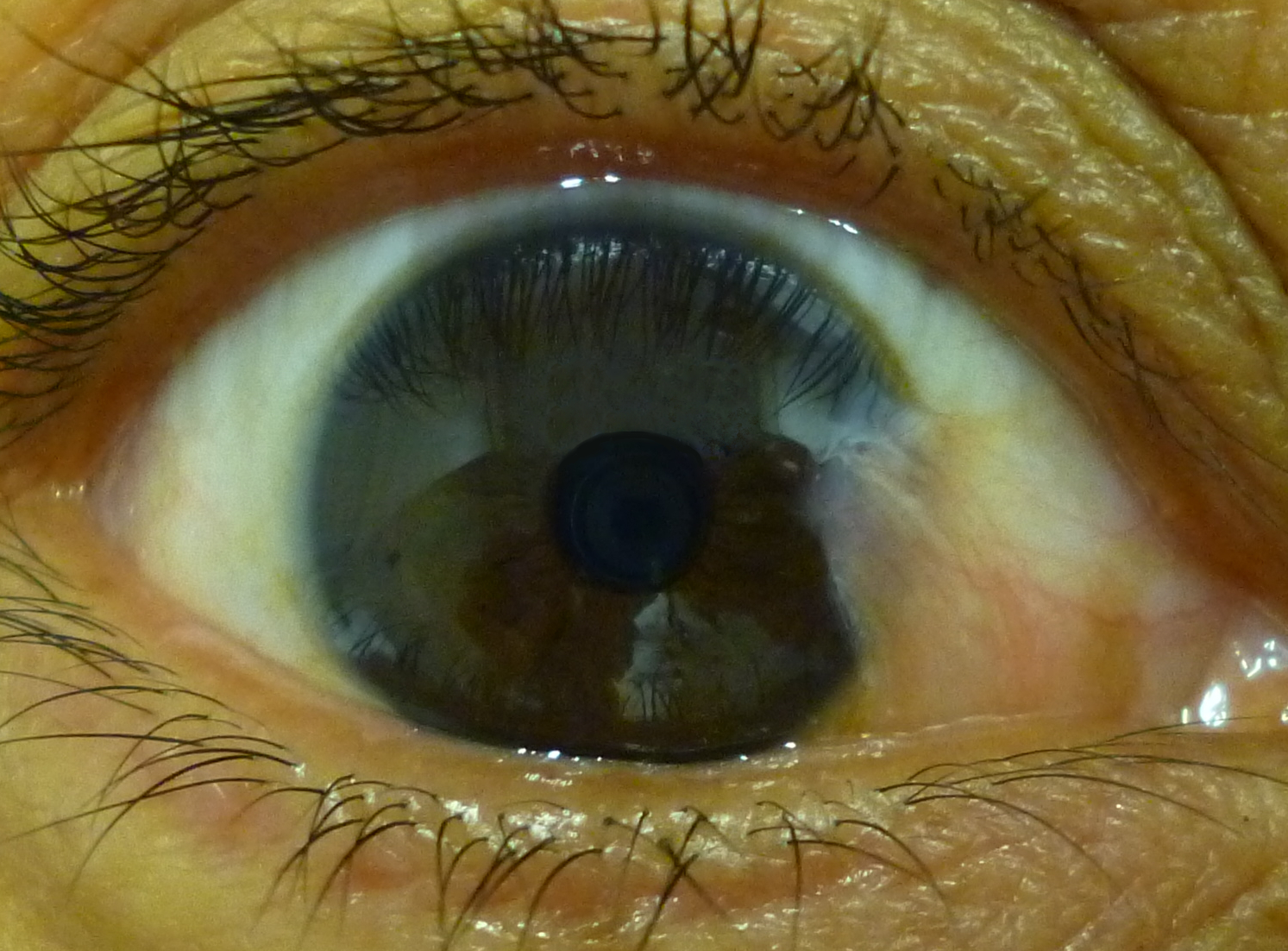
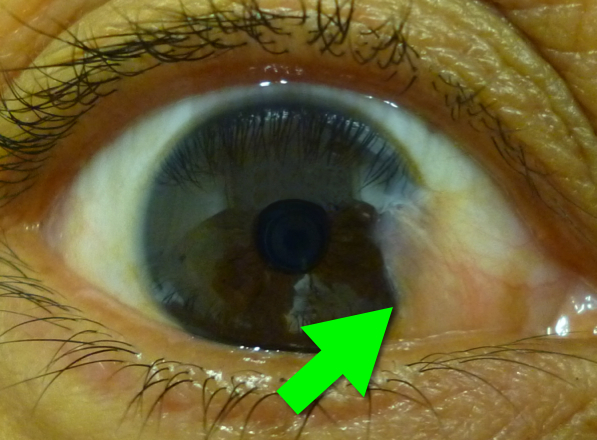
46 year-old female presents with a headache. The following is seen on visual inspection of the eye. What's the diagnosis?
Radiation therapy is frequently utilized in the management of numerous thoracic malignancies
Cardiovascular disease is now the leading cause of nonmalignancy death in radiation-treated cancer survivors
The spectrum of radiation-induced cardiac disease is broad
The relative risk of CAD, CHF, pericardial/valvular disease, and conduction abnormalities is particularly increased
Early identification of potential cardiac complications w/cardiac MR and echocardiography provides an opportunity for regular assessment and potentially improved long term mortality

{kind=link}