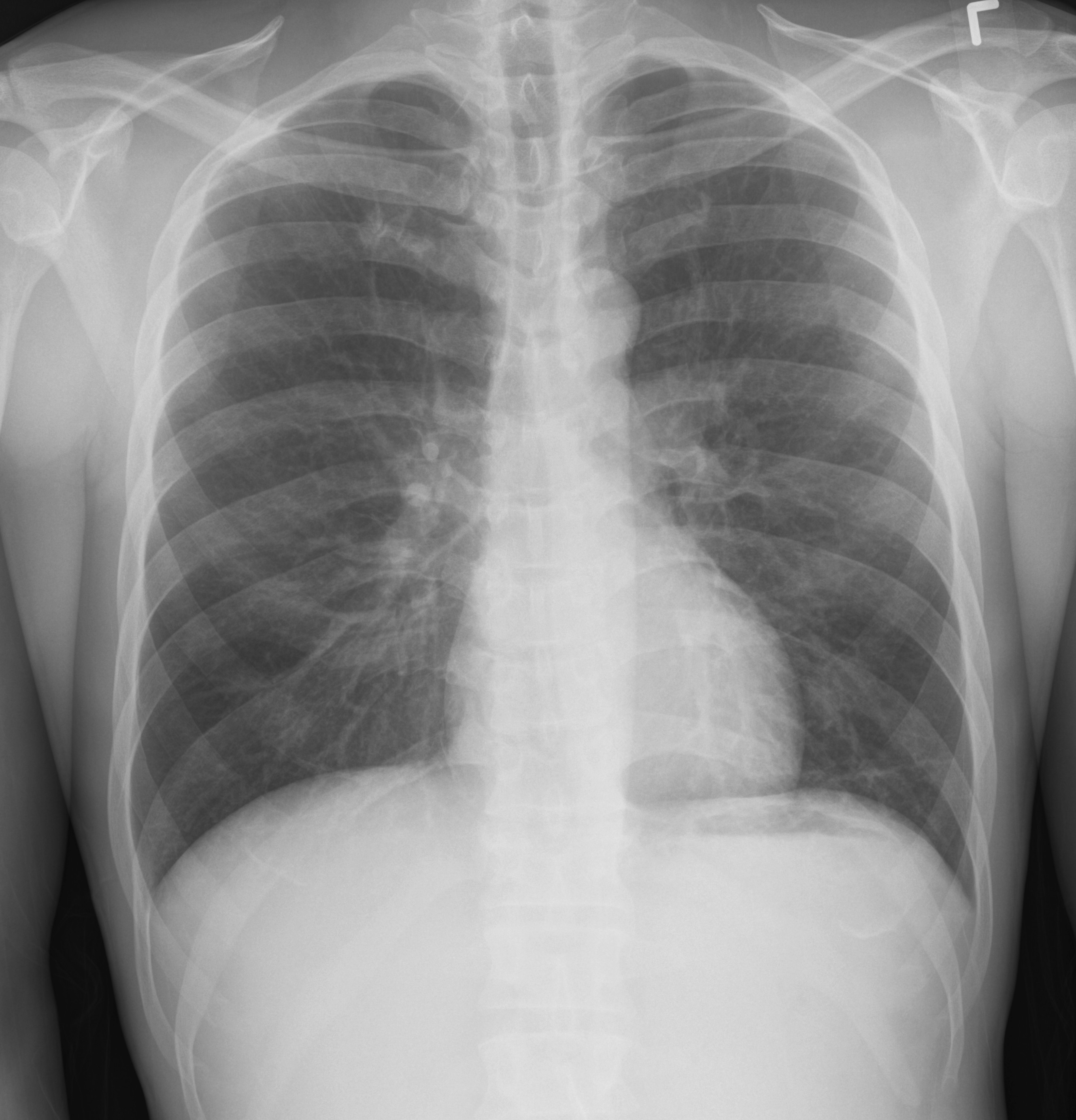
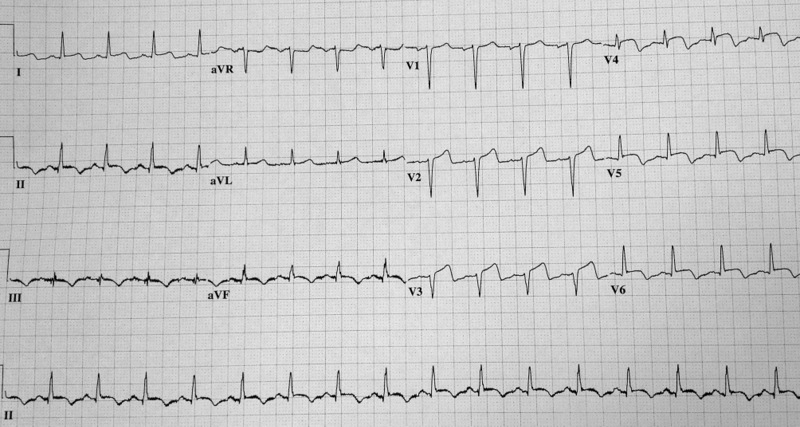
64 year-old female presents with chest pain following an argument with her husband. Her echocardiogram (apical four-chamber view) and ECG are shown. Her initial troponin is 10. What's the diagnosis?
Recent advances in resuscitation science have enabled emergency physicians to identify factors associated with good neurologic and survival outcomes. Cases of persistent ventricular dysrhythmia (VF or VT) present a particular challenge to the critical care provider. The evidence base for interventions in shock refractory ventricular VF mainly consists of case reports and retrospective trials, but such interventions may be worth considering in these difficult resuscitation situations:
1. Double sequential defibrillation
-For shock-refractory VF, 2 sets of pads are placed (anterior/posterior and on the anterior chest wall). Shocks are delivered as "closely as possible."1,2
2. Sympathetic blockade in prolonged VF arrest
-"Eletrical storm," or incessant v-fib, can complicate some arrests in the setting of VF. An esmolol bolus and infusion may be associated with improved survival.3 Left stellate ganglion blockade has been identified as a potential treatment for medication resistant VF.4
3. Don't forget about magnesium!
-May terminate VF due to a prolonged QT interval
4. Invasive strategies
-Though resource intensive, there is limited experience with intra-arrest PCI and extracorporeal membrane oxygenation. Preestablished protocols are key to selecting patients who may benefit from intra-arrest PCI and/or ECMO. 5
5. Utilization of mechanical CPR devices
-Though mechanical CPR devices were not officially endorsed by the AHA/ECC 2010 guidelines, there's little question that mechanical compression devices address the complication of provider fatigue during ongoing resuscitation.
A new recommendation in the 2013 Ischemic Stroke Guidelines provides guidance on what to do in patients taking new oral anticoagulants who are deemed eligible for IV fibrinolysis. Here is what the guidelines say:
Until further data are available, a history consistent with recent use of new oral anticoagulants generally precludes use of IV tPA.
Children frequently present with "pink eye" to the ED. When they do, parents often expect antibiotics. How many of these kids actually need them? Previous studies have shown approximately 54% of acute conjunctivitis was bacterial, but antibiotics were prescribed in 80-95% of cases.
A prospective study in a suburban children's hospital published in 2007, showed that 87% of the cases during the study period were bacterial. The most common type of bacteria was nontypeable H. influenza followed by S. pneumoniae.
Topical antibiotic treatment has been shown to improve remission rates by 6-10 days.
Spring is in the air... and so is rotavirus.
Area of the world affected:
· Diarrheal illnesses were responsible for 1.6 million deaths for children under 5 globally in 2002.
· This number has improved over the years, in part due to oral rehydration salts (ORS) which were developed for cholera.
Relevance to the US physician:
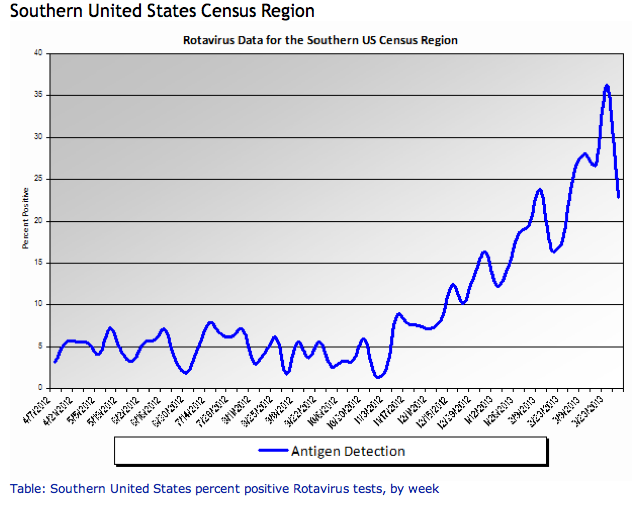
http://www.cdc.gov/surveillance/nrevss/rotavirus/region.html#top
· ORS are also important for rotavirus treatment and uncomplicated gastroenteritis in children and adults.
· Commercially prepared solutions have different concentrations of ingredients, but all will work as better treatment and rehydration than common household products like sports drinks and juice.
Bottom line:
Consider ORS in patients with uncomplicated acute gastroenteritis.
University of Maryland Section of Global Emergency Health
Author: Jennifer Reifel Saltzberg, MD, MPH
Hormonal Dysfunction in Neurologic Injury
Knee Pain Injuries are Radiographs needed?
Many people know that the folks in Ottawa have come up with a rule to determine whether radiographs are needed in patients complaining of knee pain. The Ottawa Knee rules that that radiographs are only required for knee injuries with any of the following:
• Age 55 years or older
• isolated tenderness of patella
• tenderness at head of fibula
• inability to flex to 90'
• inability to bear weight both immediately and in the emergency department (4 steps)
Well another group in Pittsburgh have their own set of rules that were recently shown to be more specific with equal sensitivity. The Pittsburgh decision rules state that radiographs are only needed if
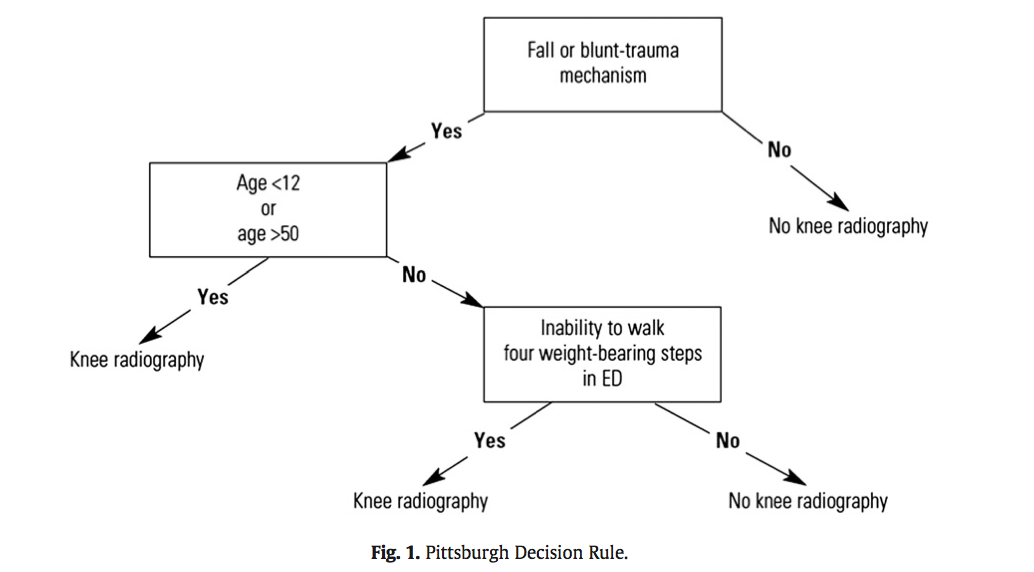
So consider using the Pittsburgh or Ottawa Knee rules the next time you have a patient with knee pain to determine if those radiographs are really needed.
The full article can be found at http://www.ajemjournal.com/article/S0735-6757%2812%2900566-9/abstract
You have diagnosed an infant or child with pneumonia. How do you decide if they need admission?
The Pediatric Infectious Disease Society and the British Thoracic Society each have guidelines from 2011 to help with this decision.
Background Information:
Combination antiretroviral therapy (cART) reduces HIV-associated morbidities and mortalities but cannot cure infection. Recent literature has suggested that early initiation of cART with primary infection can lead to “functional cure” for HIV infected patients with suppressed viremia and delayed progression to clinical symptoms.
Pertinent Study Design and Conclusions:
- Researchers studied 14 patients whose treatment with combination antiretrovirals began soon after exposure to HIV. The patients' viral loads became undetectable within roughly 3 months, and treatment was interrupted after about 3 years.
- The patients were found to have very low viral loads and stable CD4-cell counts after several years without therapy. The researchers estimate that about 15% of those treated early could achieve similar results.
Bottom Line:
Have a high suspicion of acute anti-retroviral syndrome in the ED (fever, rash, pharyngitis, lymphadenopathy) and test properly (viral load NOT ELISA) to identify patients who may benefit from early, rapid initiation of cART.
University of Maryland Section of Global Emergency Health
Author: Emilie J. B. Calvello, MD, MPH
There are several reasons why a mechanically ventilated patient may decompensate post-intubation. Immediate action is often needed to reverse the problem, but it can be difficult to remember where to start as the vent alarm is sounding and the patient is decompensating.
Consider using the mnemonic “D.O.P.E.S. like D.O.T.T.S.” to assist you in first diagnosing the problem (D.O.P.E.S.) and then fixing the problem (D.O.T.T.S.). You can view an entire lecture on the Crashing Ventilated Patient here.
Step 1: Could this decompensation be secondary to D.O.P.E.S.?
Step 2: Fix the problem with D.O.T.T.S.
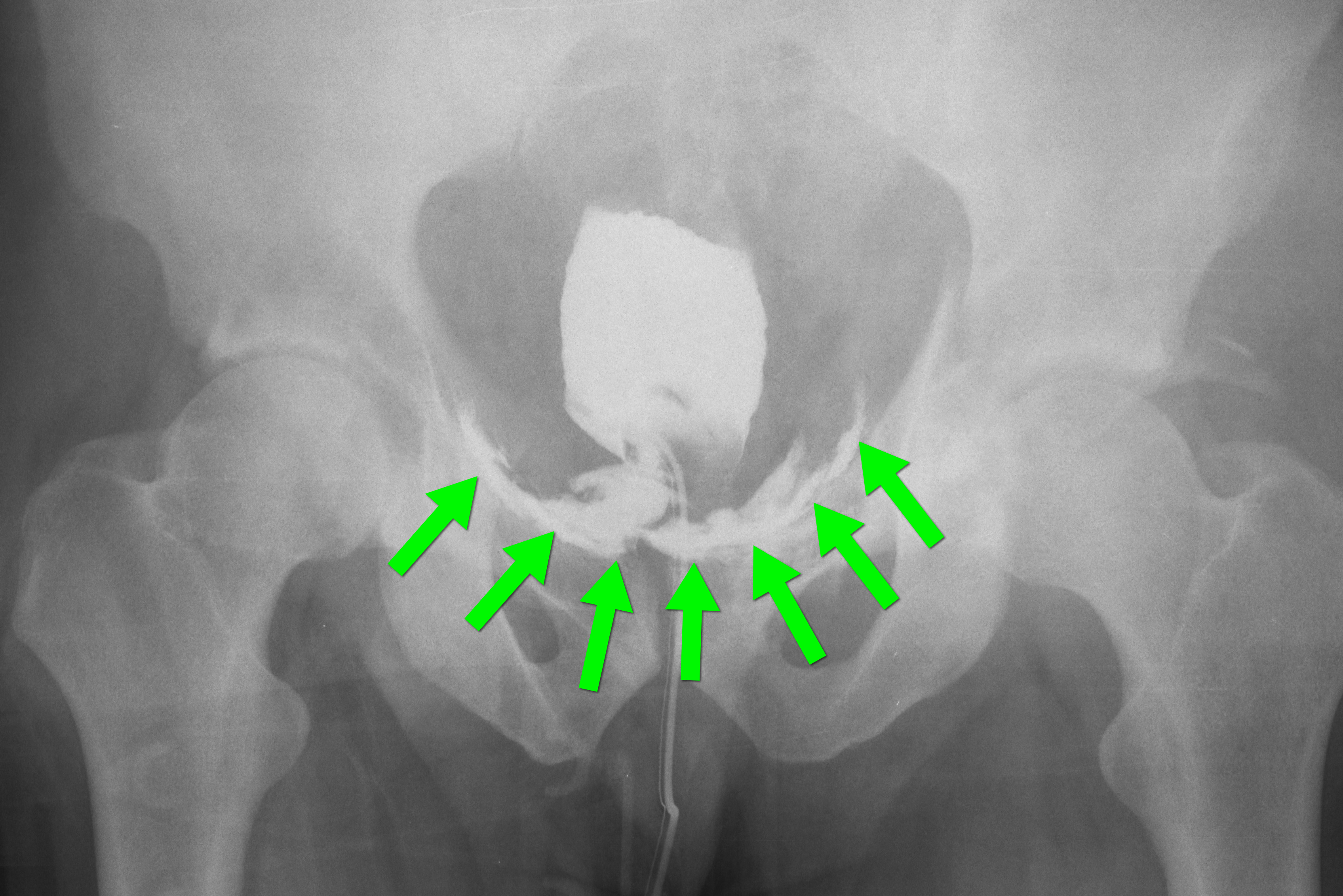
35 year-old male presents after a motor vehicle crash. No blood seen at the meatus of the penis and a Foley catheter is placed (see photo below). What's the next diagnostic step?

In children, it is important to consider the maximum doses of local anesthetics when performing a laceration repair or painful procedure like abscess drainage. If there are multiple lacerations, or large lacerations, it may be possible to exceed those doses if one is not careful.
Max doses of common anesthetics
For example, in a 20 kg child (an average 5-6 year old), the maximum doses would be:
Pearls:
Cocaine toxicity is characterized by the sympathomimetic toxidrome: tachycardia, hypertension, hyperpyrexia, diaphoresis as well as sodium channel blocking effects that can cause local anesthesia topically, QRS widening and even seizure.
Usual treatment for a cocaine toxic patient is benzodiazepines and cooling. Be wary of end organ damage, trauma and seizures.
There was a recent study that looked at dexmedetomidine to treat the sympathomimetic effects. Placebo-controlled trial used cocaine-addicted volunteer and applied intranasal cocaine. Measuring skin sympathetic nerve activity and skin vascular resistance, this study, unfortunately, showed as the dose increased MAP did not fall further and increased paradoxically in 4 of 12 subjects.
This highlights the incredible physiologic mechanism of catecholamine release from the CNS with cocaine. This mechanism overlaps some with the centrally acting alpha agonist - dexmedetomidine and was shown in the study by Kontak et al.
General Information:
14 cases of lower respiratory infection caused by a new coronavirus (not the original SARS virus, but with a similar picture) occurred in the past year. Mortality rate of this virus is >50%.
Area of the world affected:
Relevance to the US physician:
Bottom Line:
Consider this infection in patients with a lower respiratory tract infection who have traveled to or had contact with someone who traveled to the above regions in the past 10 days.
ASK ABOUT RECENT TRAVELS IN PATIENTS PRESENTING WITH SYMPTOMS OF SEVERE LOWER RESPIRATORY TRACT INFECTION!
University of Maryland Section of Global Emergency Health
Author: Veronica Pei MD, MPH
Extubating in the ED