This winter season has brought a rise in influenza and RSV activity in Maryland and in many parts of the country. It is also important to remember other potentially lethal infections that are prevalent in the winter and early spring months, such as Neisseria meningitidis. In fact, a recent study2 showed a potential increase in meningococcal disease when influenza and RSV activity is high.
What:
Encapsulated, gram-negative diplococcus
Where:
Found in nasopharyngeal secretions, carrier rates 2-30% in normal populations
Who:
Age of incidence has 2 peaks: children < 2 years old, teens 15-19 years old
Young adults who live in shared housing, such as college dorms and military recruits
Clinical Presentation:
Early non-specific symptoms of URI, fever, malaise, myalgias
Meningitis: non-specific prodrome + headache, stiff neck (not found in younger children who often present atypically with irritability and/or vomiting)
Meningococcemia: above symptoms + hypotension + petechial rash (>60% of patients)
Treatment:
Early (!) antibiotics: 3rd generation cephalosporins (<3mo: cefotaxime; older infants, children, and teens: ceftriaxone); PCN G is antibiotic of choice for susceptible isolates
Early and aggressive management of shock
Prevention:
Tetravalent vaccine, MCV4 (Menactra, Menveo), available for serogroups A, C, Y and W-135 is given routinely at age 11-12 years old with an additional booster at 16-17 years old. MCV4 does not protect against serogroup B which accounts for 30% of infections.
There have been many attempts to reduce the incidence of contrast-induced nephropathy. Mechanism usually centers around antioxidant properties or free radical scavengers that prevent the acute kidney injury that may result after intravenous contrast. IV Fluid hydration, sodium bicarbonate and acetycysteine have been studied with only some evidence. There is also some controversial data that is beginning to surface regarding the use of atorvastatin with a recent article in Circulation 2012 that showed high dose atorvastatin (80mg) 24 hrs prior to angiography prevented contrast-induced acute kidney injury in patients with mild to medium risk. Link to article has been provided:
http://circ.ahajournals.org/content/126/25/3008
Case Presentation:
A 43 year old diabetic woman presents with dyspnea and a dry cough. Her vital signs are: BP 84/42, HR 135 RR 37 T 38.5. Lobar consolidation is seen on chest xray. She decompensates and is intubated, a central line is placed, and IV fluids are started. Her husband reports that they had just returned from a vacation in Thailand one week earlier.
Clinical Question:
Does the recent travel change your choice of empiric antibiotics?
Answer:
The patient should also be covered for melioidosis, and infection caused by Burkholderia pseudomallei.
Bottom Line:
Patients presenting with severe infections and recent travel to an endemic area should receive emperic antibiotics with ceftazidime or a carbapenem until another source is identified.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
The updated Surviving Sepsis Guidelines have been released (click here) and here are some recommendations as they pertain to hemodynamic management (grades of recommendations in parenthesis).
Fluid therapy
Vasopressors (targeting MAP of at least 65 mmHg)
Corticosteroids
Inotropic Therapy
40 year-old female drove into a ditch. Right sided chest pain and stable vitals. Here's the CT but what do you think the initial CXR showed (Hint: it's a trick)?
Hematoma Block
Provides good aesthesia for reduction of fractures. Onset in approximately 5 minutes
Benefits: No need for NPO, simple and easy to perform & can be done without additional personnel (unlike w/ procedural sedation)
Contraindications: Open fractures, dirty or infected overlying skin
1) Identify fracture site with x-ray and palpation
2) Clean skin w/ Betadine
3) Insert needle into the hematoma. * Confirm placement by aspirating blood *
4) Inject anesthetic (lidocaine 1 or 2%) into the fracture cavity and adjacent periosteum
http://www.youtube.com/watch?v=tjnsdjfwMmY
Cyclophosphamide-induced hemorrhagic cystitis is a well known to oncologists. This unique complication of this chemotherapeutic drug has a defined mechanism and could be seen in your Emergency Department.
- Hemorrhagic cystitis occurs in 46% of patients that receive cyclophosphamide
- Can occur even months after administration
- 5% can actually die from the hemorrhage
- Treatment: Bladder irrigation, hydration, supportive. Oral adminsitration of MESNA (2mercaptoethan sulfonate) and bladder irrigation with prostaglandins and even methylene blue have been attempted.
A 38 year old man is brought in by ambulance for a seizure. His medical history is not known. On exam he is post-ictal and otherwise has a non-focal neurologic exam. He has an abrasion above the right eye, a small tongue laceration, and was incontinent of urine. A head CT was done and is shown below. What was the cause of this man's seizure?

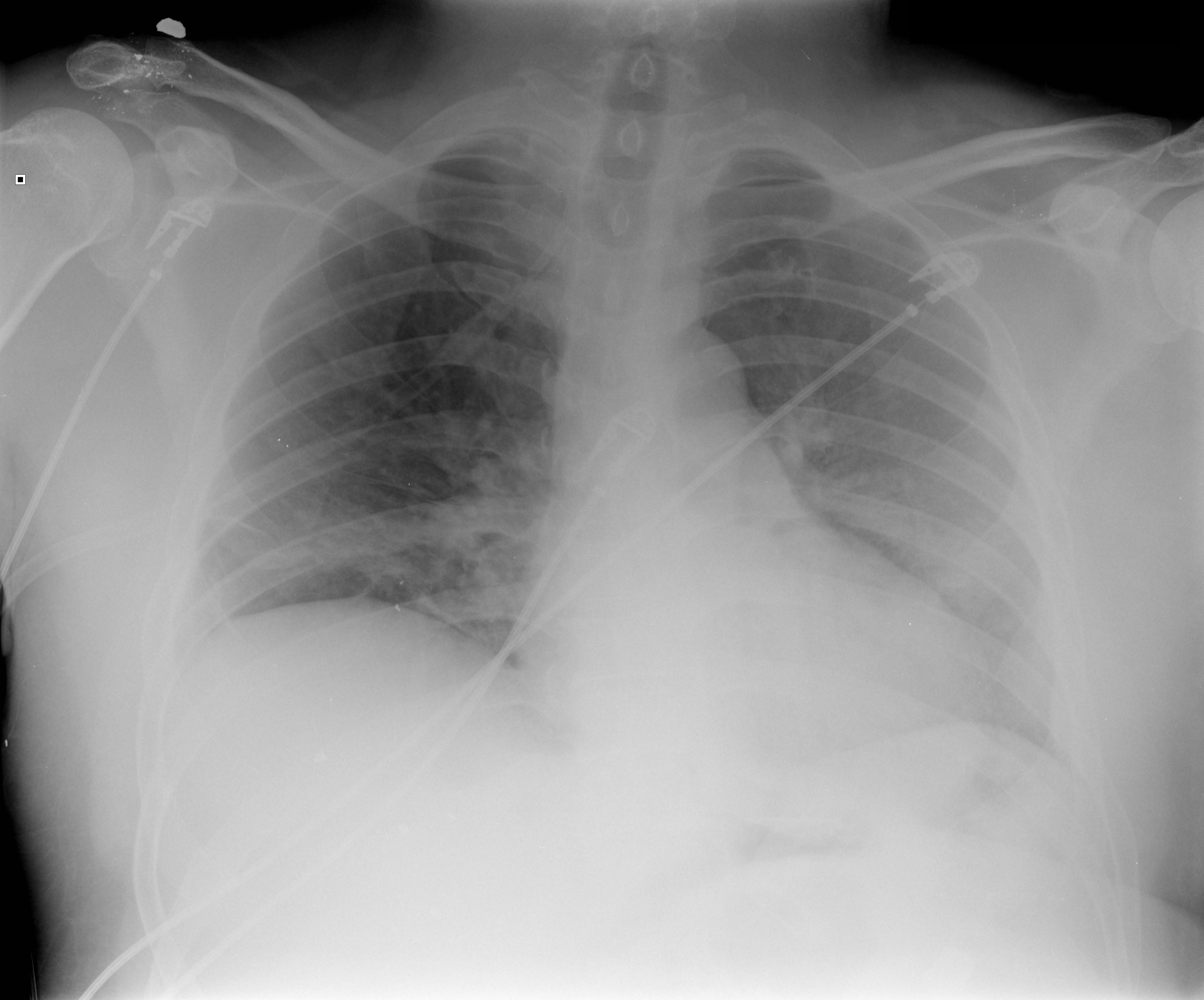
Postintubation Hypotension
45 year-old male complains of chest pain and cough. He also tells you, "...oh, and by the way doc, I just smoked something." What's the diagnosis?
· Cyanosis in the newborn is defined as an arterial saturation <90% and a PO2 <60 torr
· To help differentiate between cardiogenic and non-cardiogenic causes initially obtain an arterial saturation on room air and obtain a subsequent measurements on 100% oxygen
· Infants w/neurogenic or pulmonary causes of cyanosis will demonstrate increases in arterial blood saturation on 100% oxygen while infants with congenital heart disease show minimal elevation
· There are 3 general sources of arterial desaturation in neonates with structural heart disease:
1.) Lesions with decreased pulmonary blood flow (tetralogy of Fallot, severe pulmonary stenosis/atresia, and tricuspid atresia)
2) Admixture lesions, in which desaturated systemic venous blood mixes with intracardiac blood, and then enters the aorta (transposition of great vessels, partial anomalous pulmonary venous drainage)
3) Lesions with increased pulmonary blood flow and pulmonary edema, in which diffusion barriers and intrapulmonary shunting prevent proper oxygenation (truncus arteriosus)
Patient: A 10 year old female is brought to the ED after swallowing 2 beads (see image). Based on the findings, what are your concerns and what is the disposition?

SSRIs and SNRIs like venlafaxine and sertraline are well known to cause hyponatremia. Usually considered safe, this adverse drug event can lead to weakness, confusion, seizure and even cerebral edema. Elderly are more susceptible to this adverse effect.
ADH is regulated by serotonin and thus the mechanism for the Hyponatremia is SIADH.
Tolvaptan, a vasopressin receptor antagonist, has been a new treatment that has been used anecdotally in Europe. Waiting for the first US case report.
More than 1.2 billion people are infected with at least one species.
Most helminth infections are contracted by ingesting the eggs, except strongyloides and hookworm whose larvae penetrate bare skin when it is contact with the soil.
The roundworm (Ascaris lumbricoides) life cycle involves migration through the lung tissue which can cause pneumonitis. Patients can present with interstitial infiltrates, wheeze, and blood tinged sputum. Ascaris than migrates to the intestines where it can cause partial small bowel obstruction. In pediatric patients, the appendix may be invaded causing gangrene with symptoms indistinguishable from appendicitis. In adults, the worms can invade the biliary tract and cause biliary disease or pancreatitis. Fever causes this helminth to migrate and it can emerge from the nasopharynx or the anus.
Whipworms (Trichuris trichiura) present as colitis or symptoms similar to inflammatory bowel disease. Chronic illness can involve anemia and clubbing. In severe cases, trichuris can cause dysentery and rectal prolapse.
Hookworms (Necator americanus or Ancylostoma duodenale) also have a pulmonary phase, but with milder symptoms than Ascaris. Eventually hookworms cause iron deficiency anemia and malnutrition. They can be a primary cause of anemia in pregnancy in endemic areas.
Threadworm (Strongyloides stercoralis) can cause a wide spectrum of disease presentations. The infection can start with a rash, larva currens. The infection may be subclinical or may invade the lung, intestinal wall, or the nervous system. Eventually hyperinfection may develop which is a very large increase in worm burden and then the infection becomes disseminated.
Toxocara canis or toxocara cati have affected approximately 14% of the US population. These helminthes reproduce in dogs or cats, and human infection is not part of the normal life cycle. Most infections are subclinical but it can produce a mild pneumonitis that is very similar to asthma. There can be pain and inflammation as the helminthes travel through organs such as the liver or lung and is called visceral larva migrans. The helminth may also move through the eye and optic never causing an ocular form of the disease, ocular larva migrans.
Pinworms (Enterobius vermicularis) are the cause of most common helminth infection in US and can present with anal pruritus leading to trouble sleeping. When an infection is identified, everyone in the household should be treated, regardless of symptoms.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
Intra-aortic balloon pumps (IABP) are devices that provide hemodynamic support during cardiogenic shock; the balloon inflates during diastole (improving coronary artery perfusion) and deflates during systole (reducing afterload and improving systemic perfusion). Click here to see a 41 second video illustrating how it works.
Several guidelines recommend placement of an IABP for patients in cardiogenic shock secondary to acute myocardial infarction (AMI), if early revascularization (e.g., CABG) is planned (Class I recommendation). Data behind this recommendation, however, is limited.
The IABP-SHOCK II trial was a randomized, multi-center, open-label study that enrolled 600 patients (598 in the analysis) with cardiogenic shock secondary to AMI (STEMI or NSTEMI). Patients were randomized to the control group (receiving standard therapy; N=298) or the experimental group (receiving IABP; N=300).
No significant difference was found between groups with respect to 30-day mortality (primary end-point), secondary end-points (e.g., time to hemodynamic stabilization, renal function, lactate levels, etc.), or complications (e.g., major bleeding, peripheral ischemic complications, etc.).
Bottom line: Perhaps it is time to reassess the approach to cardiogenic shock secondary to AMI when early revascularization is planned. At this time consultation with local expertise is recommended.
"When can my child get back out on the field doc?"
Return to play
▸ Concussion symptoms should be resolved before returning to exercise.
▸ A RTP progression involves a gradual, step-wise increase in physical
demands, sports-specific activities and the risk for contact.
▸ If symptoms occur with activity, the progression should be halted and
restarted at the preceding symptom-free step.
▸ RTP after concussion should occur only with medical clearance from a
licenced healthcare provider trained in the evaluation and management
of concussions.
Short-term risks of premature RTP
▸ The primary concern with early RTP is decreased reaction time leading
to an increased risk of a repeat concussion or other injury and
prolongation of symptoms.
Long-term effects
▸ There is an increasing concern that head impact exposure and
recurrent concussions contribute to long-term neurological sequelae.
▸ Some studies have suggested an association between prior concussions
and chronic cognitive dysfunction. Large-scale epidemiological studies are
needed to more clearly define risk factors and causation of any long-term
neurological impairment.
Several medications can produce a false-positive result for methadone on the urine drug screen: diphenhydramine, doxylamine, clomipramine, chlorpromazine, quetiapine, thioridazine, and verapamil.
Add a new one to the list. Tapentadol, a relatively new opioid analgesic similar to tramadol, can also produce a false-positive result for methadone on certain immunoassays.
A separate study concluded that tapentadol does not affect the amphetamine screen.
