Just when you think buying organic protects you from chemicals and pesticide, along comes the studies detecting arsenic in rice products and specficially in organic foods with brown rice organic sweetener. An organic toddler milk formula reportedly had 6x EPA standards for safe drinking water limit.
The more toxic arsenic is the inorganic arsenic which can cause neuropathy but after chronic exposure can cause a classic arsenic keratosis - see attached pic. The inorganic is seen commonly in seafood and is more easily excreted by the body. Unfortunately, in the study referenced here, inorganic As was the predominant type.
The Lung Transplant Patient in Your ED
27 year-old woman with AIDS presents complaining of a painful, puritic, and papular rash. What's the diagnosis?

Pericarditis is based on clinical diagnosis; typically two of four criteria are found (pleuritic chest pain, pericardial rub, diffuse ST-segment elevation, and pericardial effusion).
Treatment of pericarditis should be targeted at the cause.
Most causes of pericarditis have a good prognosis and are self-limited.
Lactate levels help to confirm septic arthritis but what about bacterial meningitis. As reported in the daily electronic ACEP newsletter a small study of 45 patients showed that all patients with a confirmed diagnosis of bacterial meningitis had a CSF lactate level > 3.5 mmol/L. Therefore, it might be true that viral meningitis will only have CSF lactate levels < 3.5 mmol/L.
With only 45 patients, this finding is clearly not ready for Prime Time but consider adding it to your next CSF study so more data can be collected on the utility of this test.
The story as seen in ACEP eNews on September 14th, 2012 is:
MedPage Today (9/14, Gever) reports, "Cerebrospinal fluid (CSF) levels of lactate were a perfect marker of viral versus bacterial meningitis in a small study, a researcher reported" at the Interscience Conference on Antimicrobial Agents and Chemotherapy. Researchers found that, "among 45 adults in whom the etiology of meningitis was microbiologically confirmed, all those with CSF lactate levels above 3.5 mmol/L had the bacterial form, whereas every patient with lower levels had viral meningitis."
Carbon monoxide (CO) and hydrogen cyanide (HCN) are two of the main gases causing injury and death from smoke inhalation in fire victims. During the first phase of a fire, and prior to depletion of oxygen reserves and subsequent production of CO, formation of HCN from the thermal breakdown of nitrogen-containing materials may be the primary cause of lethal poisoning in an enclosed-space fire.
A recent, retrospective, observational study from Poland assessed the prevalence of toxic HCN exposure in victims of enclosed-space fires.
Important findings:
Conclusion: The high prevalence of coincident HCN concentrations and COHb levels in victims of enclosed-space fires emphasises the need to suspect HCN as a co-toxin in all persons rescued from fire who show signs and symptoms of respiratory distress.
40 year-old male with severe uncontrolled hypertension presents with altered mental status (head CT below). The CXR is from the same patient. What's the connection?
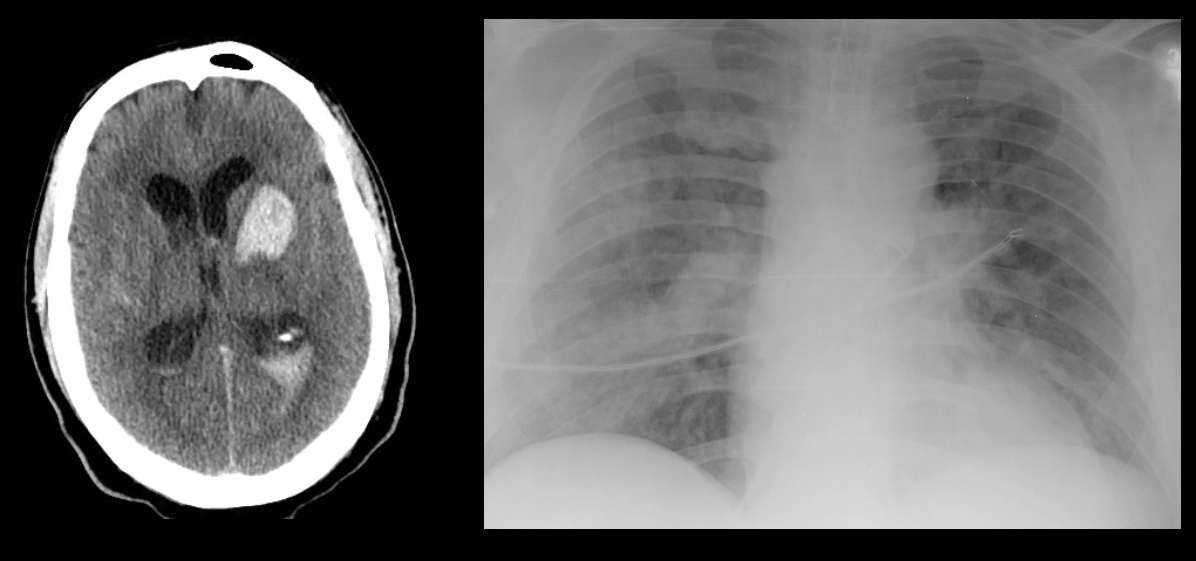
40 year-old male with severe uncontrolled hypertension presents with altered mental status. Head CT is shown here. Name three common anatomic locations generally seen for non-traumatic intracerebral hemorrhage.
Which patient has a better blood pressure, the patient with a blood pressure of 110/40 or the patient with a blood pressure of 90/60?
Mean arterial pressure (MAP) is generally considered to be the organ perfusion pressure in an individual. Because MAP requires an inconvenient calculation, we've all been taught...misled perhaps...into focusing on systolic blood pressure (SBP) as a marker of how well-perfused a patient is, and we tend to ignore the diastolic blood pressure (DBP).
It's important to remember, however, that we spend most of our lives in diastole, not systole. As a result, our organs spend more time being perfused during diastole than systole. The MAP takes this into account: MAP = (SBP + DBP + DBP)/3. DBP is more important than SBP!
So which patient is perfusing his vital organs better, the one with a BP of 110/40 or the one with a BP of 90/60? Do the MAP calculation...90/60 is better than 110/40!
Pay more attention to those diastolic BPs!
Apprehension test for patellar dislocation
Test is used to access for the possibility of a patellar dislocation, prior to evaluation, now spontaneously reduced.
Similar to the shoulder apprehension test
Designed to place the patella in a position of imminent subluxation or dislocation
http://mulla.pri.ee/Kelley%27s%20Textbook%20of%20Rheumatology,%208th%20ed./HTML/f4-u1.0-B978-1-4160-3285-4..10042-7..gr16.jpg
http://www.youtube.com/watch?v=9AJxcbd9g8A
Place the knee in 20 - 30 degrees of flexion with the quadripces relaxed. Grasp the patella and attempt to place lateral directed stress.
If the patella is about to dislocate, the patient will experience apprehension due to the familiar pattern of dislocation, report the laxity and resist further motion by contracting the quadriceps
Ligamentous laxity is increased in children and ligamentous injury is more common than fractures.
If fractures occur, they are more likely to be in the upper cervical spine in infants and the lower cervical spine in older children.
Pseudosubluxation: physiologic subluxation between C2-3 and C3-4 may exist until age 16 years
Screening Assessment/Clearance for Verbal Children
-Midline C-spine tenderness?
-Pain with active motion?
-Altered level of alertness?
-Evidence of intoxication?
-Focal neurological deficit?
-Distracting painful injury?
-High impact injury?
Screening Assessment/Clearance for Pre-Verbal Children
-Neurological assessment of basic reflexes
-Response to painful stimuli
-Equal movements of all extremities
-Response to sound (eye tracking)
-Extremity strength and resistance
-Palpate posterior C-spine (observe for facial grimace)
-Feel for step-offs, deformities
-Verify full range of motion of neck (may need to be creative)
-Repeat neurological assessment
If concern arises on screening assessment, keep child in hard cervical collar and image (may start with x-ray and progress to CT if still concerned and x-rays negative).
If imaging negative, but persistent suspicion based on neurological deficits consider SCIWORA (Spinal Cord Injury WithOut Radiographic Abnormality) which exists in up to 50% of children with cervical cord injury, and may require MRI to further identify injury.
Right Heart Failure in the Critically Ill
32 year-old female presents with 5 days of fever, chills, and flank pain. She is hypotensive on presentation and urinalysis shows pyuria. Click here for the non-contrast CT scan. What's the diagnosis and what type of antibiotics should be started empirically?
Lyme disease is the most prevalent arthropod zoonosis in the Northern hemisphere
Carbapenems (meropenem, ertapenem, doripenem, imipenem/cilastatin) are broad-spectrum antibiotics that have good gram-negative and anaerobic coverage and are used to treat resistant bacterial infections.
Early retrospective studies showed ~10% cross-reactivity in penicillin-allergic patients.
More recent prospective studies verified penicillin allergy by the accepted standard (ie, skin test to the major and minor penicillin determinants) and tested for carbapenem allergy by administering a full therapeutic dose to carbapenem skin test-negative patients.
The cross-reactivity between skin tests appears to be around 1%, with all carbapenem skin test-negative patients tolerating the challenge.
I was reading the biography of Steve Jobs looking for incredible insights into leadership and innovation. I have realized that you basically have to be a genuis and it doesn't matter what you do. His favorite drug was LSD which he believed was necessary to improve creativity and innovation. His description of the hallucinations confirm that he was taking this drug.
We describe LSD hallucinations as a crossing of the senses or "synesthesias" - you hear the color blue, you see the smell of roses.
Steve Jobs describes a moment in a wheat field while on LSD and (paraphrasing from the biography) ..." the wheat was playing Bach beautifully"
If you have a patient describing this type of hallucination you can almost be guaranteed that they have taken LSD or some other tryptamine.