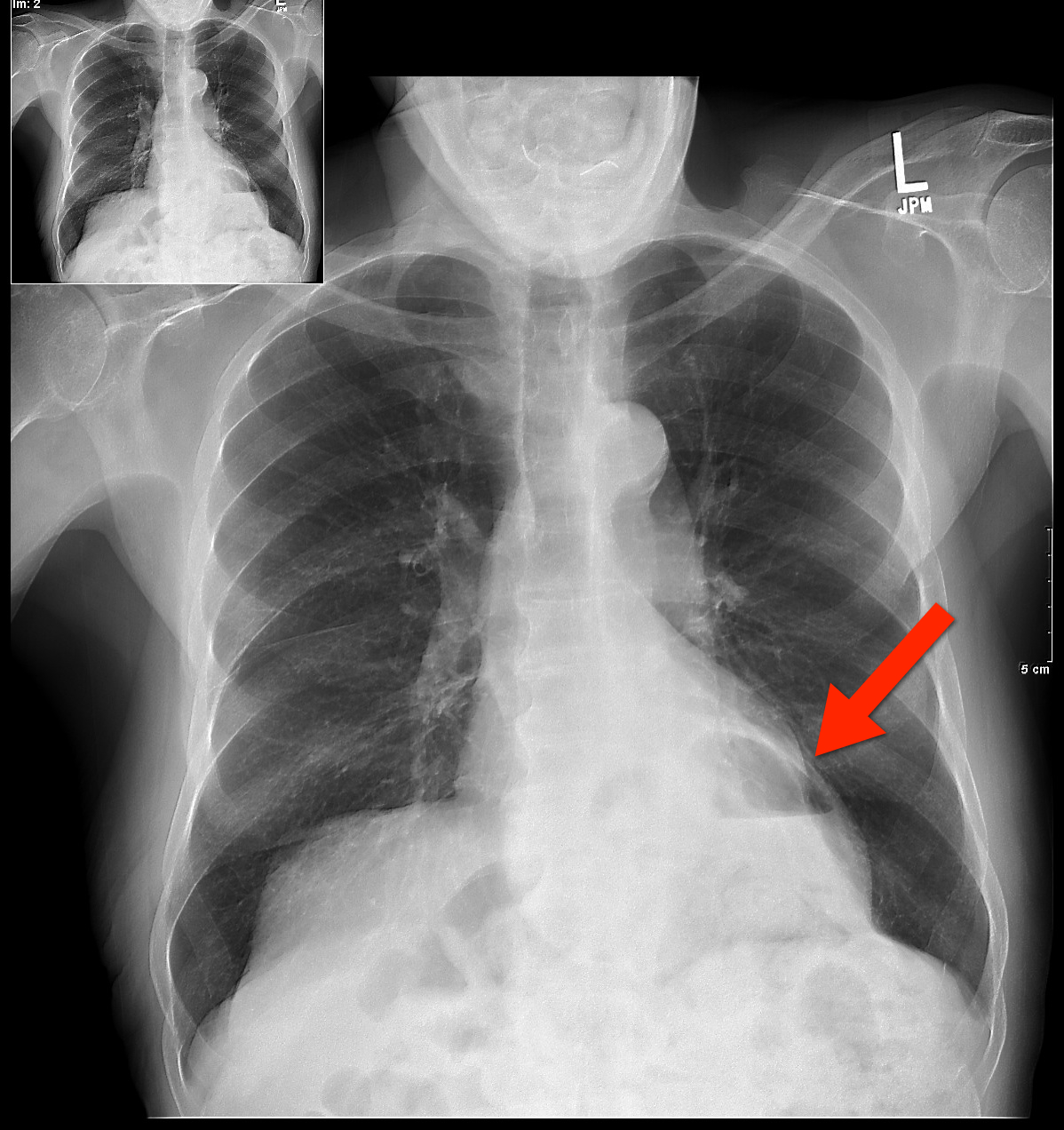
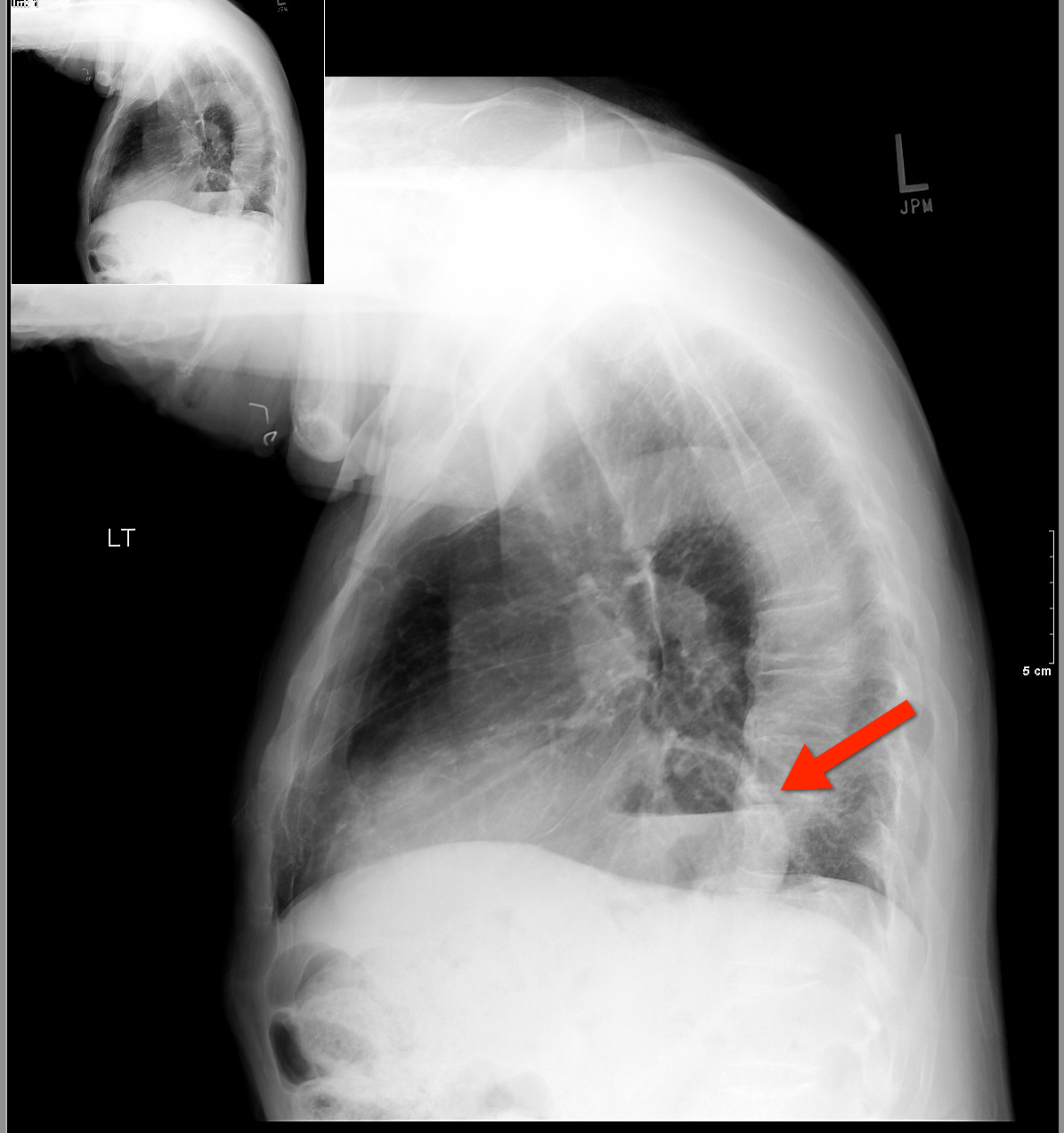
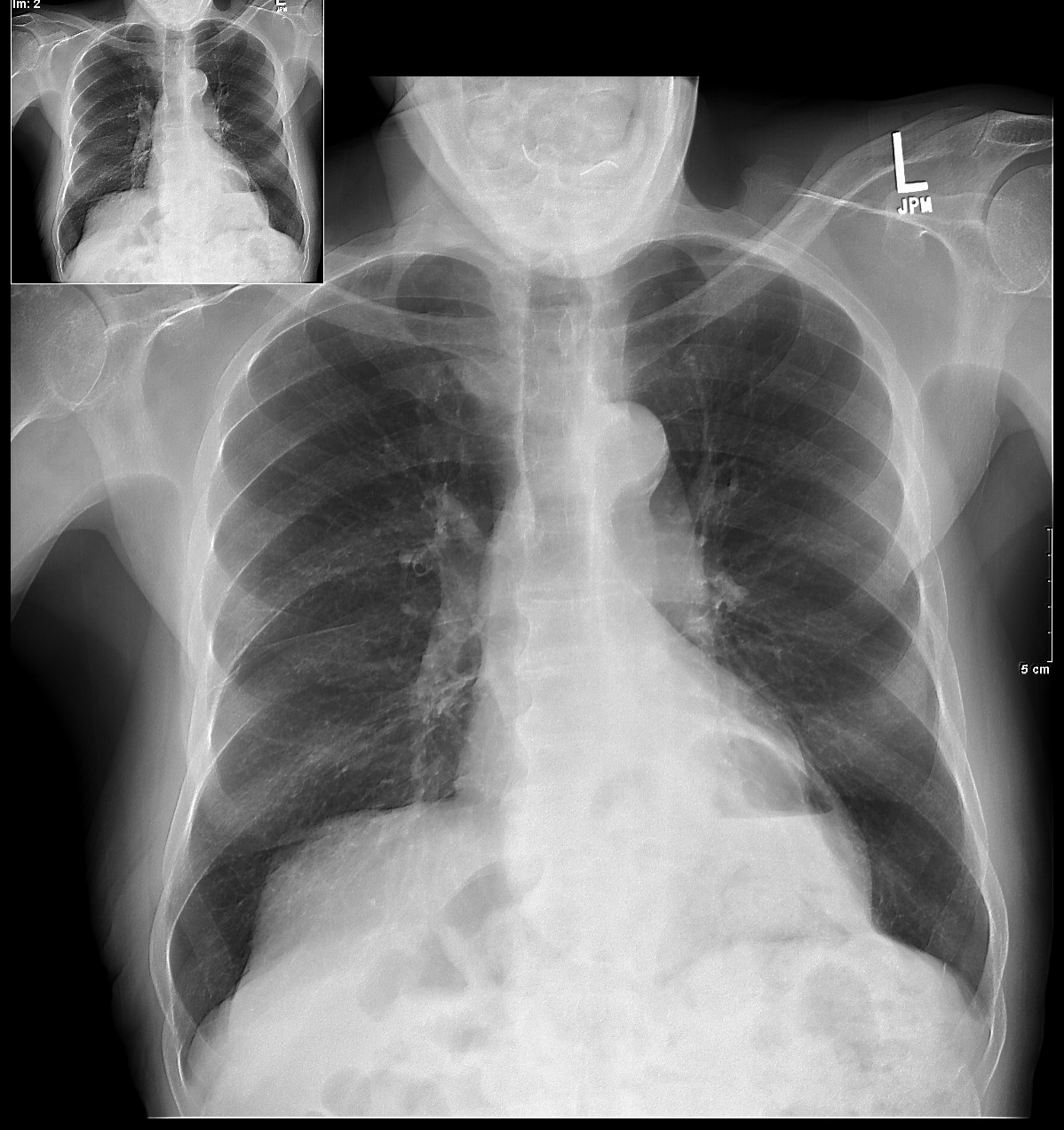
67 yo male presents with burning substernal chest pain; worse with meals and when supine. What's the diagnosis?
(from Dr. Semhar Tewelde)
Stress testing is one modality used to screen for CAD. The goal is to identify a fixed obstruction to coronary blood flow (typically plaque > 50%) such as in stable angina. However, in ACS, both USA and AMI, the underlying pathophysiology is plaque rupture (typically plaque < 50%) and thrombus formation that may not have been significant enough to cause a positive stress test.
The use of a prior negative stress test to determine the disposition of ED chest pain patients is questionable. The history of present illness should dictate patient disposition. In one study 20.7% of patients presenting to the ED with a negative stress test within three years of presentation still had significant CAD defined as a positive cardiac markers, subsequent positive stress test of any type, cardiac catheterization requiring intervention, or death due to medical cardiac arrest within 30 days of ED presentation.
Chronic exertional compartment syndrome (CECS)
An overuse injury common in young endurance athletes
In athletes with lower leg pain, CECS was found to be the cause in 13.9% - 33%.
*This is likely under diagnosed as most recreation athletes will discontinue or modify their activity level at early symptom onset
Common in runners and most often involves the anterior compartment
Occurs due to increased pressure within the fascial compartments, primarily in the lower leg
Symptoms are bilateral 85 - 95% of the time
Exercise increases blood flow to leg muscles which expand against tight surrounding noncompliant fascia. This, in turn, increases compartment pressures and eventually reduces blood flow which leads to ischemic pain. Pain usually begins within minutes of starting exercise and experienced athletes can often pinpoint the time/distance required for symptom onset.
Symptoms are primarily pain (tightness, cramping, squeezing) but may also include paresthesias and numbness. Symptoms gradually abate with cessation of activity.
Diagnosis: Although some physicians’ make a clinical diagnosis based on Hx and exam, definitive diagnosis requires measurement of compartment pressures both at rest and post exercise.
Nonsurgical treatment: activity modification and rest
Surgical treatment: >80% success with anterior and lateral compartments vs. 50% with deep posterior compartment.
Over the last few decades, the rate of breastfeeding has increased steadily in the developed countries of the world. During this time, opioid use in the general population has steadily increased as well. Despite this, clinicians remain unclear whether opioid use is safe during breastfeeding.

Sepsis is one of the top 10 causes of death in the U.S. and its incidence is on the rise.
The financial burden of sepsis is also growing; it is estimated that between 2000 and 2005 the overall cost of ICU hospitalization rose from $56.6 billion to $81.7 billion per year with severe sepsis accounting for $16.7 billion.
Although we may not be able to immediately modify the incidence of community-acquired sepsis, hospital-acquired sepsis can be reduced; for example, many cases of nosocomial sepsis are associated with catheter blood stream infections secondary to central-lines.
There are several simple strategies to prevent catheter-related blood-stream infections:
Remember: We play a large role in reducing nosocomial sepsis; be vigilant about your sterile techniques during central catheter insertions and question the need for every single line.
Bonus pearl (only for iPhone): MDRNTools is a FREE app (that’s right, FREE!) with lots of ED and ICU applications such as an IV med calculator, an RSI handbook, a Stroke Scale calculator, and more.
Download http://itunes.apple.com/us/app/mdrntools/id505794224?mt=8&ls=1

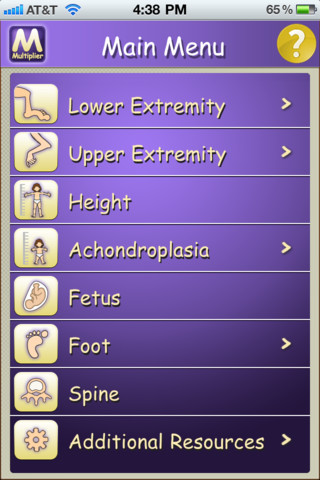
Well, here is a cool little app that has recently been released. It's an app that can predict what a child's height will be as a mature adult. This is not a joke.
A free mobile application developed by the International Center for Limb Lengthening (ICLL) at the Rubin Institute for Advanced Orthopedics (RIAO) of Sinai Hospital (right in our very own Baltimore) can predict the future mature height and bone lengths of children with the input of basic information.
That's right people. The formula has amazing accuracy and has been studied in many different centers. It's supposedly 97%+ accurate in predicting height.
The Multiplier App, available for Android, iPhone and iPad devices, is based upon the Multiplier Method, a series of formulas used to calculate and predict height and bone length in children. These formulas were developed by a team that included members of the ICLL.
Here is what it looks like. Just click on "Height" (see enclosed jpg image of the app) and then type in the child's birthday and current height in either inches or cm. The formula will then calculate what there predicted height will be.
Very, very cool ( at least I think)
(Pearl provided by Dr. Semhar Tewelde)
Physiological LV hypertrophy in trained athletes is defined by an isolated increase in QRS amplitude, normal axis, normal atrial and ventricular activations patterns, and normal ST-segment T-wave replorization; athletes of African/Caribbean descent have prominent cardiovascular remodeling leading to pronounced voltage criteria for LV hypertrophy and BER
Despite the presence of voltage criteria for LVH, pure QRS voltage criteria for LVH in an asymptomatic athlete without family hx of cardiovascular diseases or SCD, and lack of non-voltage ECG criteria does not warrant systematic evaluation with echocardiography.
In other words, young patients, especially men, especially those of African/Caribbean descent, will be expected to have large voltage QRS complexes and sometimes abnormal repolarization, and this is not necessarily a pathologic finding.
Exertional leg pain in the athlete carries a wide range of possible etiologies. In a recent review article, etiologies included, stress fracture (25%), exertional compartment syndrome (33%), medial tibial stress syndrome (13%), nerve entrapment (10%), and popliteal artery entrapment syndrome.
Medial Tibial Stress Syndrome (MTSS) is also known as shin splints. It is a repetitive-stress overuse injury.
Risk factors include: hyperpronation, higher BMI, increased hip internal rotation, and hyperplantar flexion.
While MTSS may be on a stress reaction spectrum that includes fracture, the causes are likely to also include tendinopathy and muscle dysfunction (tibialis anterior, posterior and soleus).
Radiographs will be normal with this condition. MRI and bone scan may show signal abnormality along the posterior medial tibial surface.
Treatment: In most cases participation in sports may continue. Also consider, rest/activity modification, ice, NSAIDs, physical therapy for calf stretching and strengthening, and rigid orthotics (to correct foot hyperpronation). Semi rigid and neoprene orthotics may be considered for prevention in those with a prior history.
In a recent multicenter, double-blind, randomized, non-inferiority trial, vancomycin was compared to fidaxomixin for Clostridium difficile infection.
Location: 45 sites in Europe and 41 sites in the USA and Canada
Patients: Age 16 years or older with acute toxin-positive C difficile infection.
Treatment: Oral fidaxomicin (200 mg every 12 h) or oral vancomycin (125 mg every 6 h) for 10 days.
Endpoint: Clinical cure, defined as resolution of diarrhea and no further need for treatment.
Results: 198 (91.7%) of 216 patients in the per-protocol population given fidaxomicin achieved clinical cure, compared with 213 (90.6%) of 235 given vancomycin (one-sided 97·5% CI -4·3%). Occurrence of treatment-emergent adverse events did not differ between groups.
Author conclusions: Fidaxomicin could be an alternative treatment for infection with C difficile, with similar efficacy and safety to vancomycin.
Funding: Optimer Pharmaceuticals.
It is likely that during ones career in Emergency Medicine, one will be faced with how to work up a child presenting to the ER following exposure to common house electrical current. The older recommendations were such that all children exposed, received a screening EKG and were admitted to telemetry for monitoring. However, a relatively recent article in the Annals of Emergency Medicine suggests otherwise.
In fact, after reviewing several studies the authors conclude that, although there is not enough literature to support evidence based practice “guidelines”, there appears to enough evidence to support that practice of “safely discharging these children without an initial EKG evaluation or inpatient cardiac monitoring after a common household current exposure.” This includes both 120V and 220 V exposures.
Clearly, some patients may require work up and/or admission based on other injuries or clinical presentation.
References:
Chen E H, Sareen A, Do Children Require ECG Evaluation and Inpatient Telemetry After Household Electrical Exposures? Ann Emerg Med. 2007;49:64-67.
Protamine for enoxaparin overdose
Transferring Multidrug-Resistant Organisms
Pearl provided by Dr. Semhar Tewelde
The Athlete's Heart and ECG Abnormalities
Up to 80% of athletes have common training related ECG changes/abnormalities including: sinus bradycardia, asymptomatic sinus pause, sinus arrhythmia, first degree AV block, incomplete right bundle branch block, benign early repolarization (BER), and isolated QRS voltage criteria for left ventricular (LV) hypertrophy.
Approximately 5% athletes exhibit uncommon training unrelated ECG changes/abnormalities including: T-wave inversions, ST-depression, pathological Q-waves, left axis deviation/left anterior fasicular block, right axis deviation/left posterior fasicular block, right ventricular hypertrophy, complete left or right bundle branch block, long or short QT interval, ventricular pre-excitation/WPW, Brugada pattern, and arrhythmogenic right ventricular dysplasia (ARVD).
Animal studies can pave the way for new clinical treatment modalities. In the setting of lung injury due to smoke inhalation, one of the problems (if you can get the ET tube in) are the elevated ventilatory pressures due to the massive edema. In this sheep model of smoke inhalation, nebulized epinephrine improved ventilatory pressures, PaO2/FiO2 ratio and pulmonary shunting.
We may have these sheep to thank for this new treatment.
The supine position during rapid sequence intubation may result in posterior lung atelectasis thereby reducing lung volumes, oxygenation reserve, and ultimately apnea time.
Several studies have shown that elevating the head of the bed by at least 20 degrees or placing a patient in reverse Trendelenberg position (for patients with contra-indications to elevating the head of the bed) during RSI may significantly increase apnea time.
Elevating the head of the bed may be especially helpful for patients with BMIs >35
26 year old male with pain when he extends his 4th finger as well as swelling of that digit. Diagnosis?

Cardiogenic shock pearls from Dr. Semhar Tewelde:
1. CS is most commonly secondary to a large MI where > 40% of the myocardium is involved; however mechanical, valvular, dysrhythmogenic, and infectious etiologies should also be considered: papillary or chordal dysfunction, free wall or septal defects disease, insuffiency of any valve, myopericarditis, endocarditis, Tako-tsubo, end stage cardiomyopathy, and tamponade.
2. Incidence of 5-10% STEMI and 2.5-5% NSTEMI
3. Mortality ~50%
4. Immediate coronary reperfusion is the best treatment (NNT 8). Medical therapy is a distant second choice in management, with reperfusion and pressors as needed. Early intra-aortic balloon pump use is key.
5. Recent case reports have shown imporved outcomes when induced hypothermia was used in patients refractory to traditional therapy with pressors/inotropes/IABP.
A recent study looked at the risk of sudden cardiac death during a marathon.
Many isolated reports of sudden death make headlines in the national news.
However, of nearly 11 million runners, only 59 went into cardiac arrest during a race. This equates to an incidence rate of 0.54 per 100,000 participants,
This rate appears to be on par with sudden death from other athletic endeavors such as triathlons and college athletics.
Median age was 42. Men affected more than women (men also more likely to die from the event).
71% of events were fatal.
Further, risk is greater for both cardiac arrest and sudden death for full marathons than half marathons.
Interestingly, older patients fared better (increased survival in those >40yo), thought to be due to an increased incidence of hypertrophic cardiomyopathy in younger aged runners.