Balloon Tamponade for Variceal Bleeding
This week's visual pearl is an interesting ultrasound of a psoas abscess submitted by Dr. Sa'ad Lahri. He is an Attending physician in the Emergency Department of the Khayelitsha Hospital in Cape Town, South Africa. The video quality is grainy, but it automatically replays so you can watch it a few times.
http://ultrarounds.com/ultrarounds.com/Visual_Pearl_May_14,_2012.html
[pearl provided by Dr. Semhar Tewelde]
Peripartum cardiomyopathy (PPCM) is a relatively rare idiopathic form of heart failure that occurs during the last months of pregnancy or the first months after delivery
Panner's disease refers to osteochondrosis of the capitellum.
Affects the dominant elbow of boys between the ages of 5 and 10
Associated with the repetitive trauma of throwing
Must be differentiated from osteochondrosis dissicans (occurs in the older child >13yo)
Hx: Intermittent pain and stiffness of the elbow. Better w rest, worse w activity.
PE: tenderness over capitellum w/ slight effusion. Loss of 20 degrees full extension
The articular surface of the capitellum appears irregular with areas of radiolucency.
Tx: Symptomatic treatment with rest. In severe cases a long arm splint/cast may be applied for 2-3 weeks.
http://www.ultrasoundcases.info/files/Jpg/org_34277-Afbeelding1.jpg
Ethylene glycol can result in elevated lactate concentrations secondary to hypotension and organ failure in severely poisoned patients. However, lactate production by these mechanisms tends to result in serum concentrations less than 5 mmol/L.
Unfortunately, higher lactate levels don't necessarily rule out ethylene glycol. The glycolate metabolite causes a false-positive lactate elevation when measured by some analyzers, particularly with whole blood arterial blood gas analyzers. Specific models implicated include: ABL 625, Radiometer ABL 700, Beckman LX 20, Chiron 865, Bayer (formerly Chiron) 860, Rapidlab (Bayer) 865, Integra and to a lesser extent, Hitachi 911 analyzers, but not the Vitros 950 or Vitros 250.
The degree of lactate elevation directly correlates with the concentration of glycolate present, and the artifact probably results from the lack of specificity of the lactate oxidase enzyme used in these machines.
Severe acute pancreatitis (SAP) is a life-threatening form of pancreatitis, with up to 30% mortality.
SAP may lead to hypovolemic shock (secondary to vasodilation and capillary leak), hypoxemia (from acute respiratory distress syndrome), and multi-organ failure.
Suspect SAP with signs and symptoms of pancreatitis plus any of the following:
Treatment of SAP should focus on:
Increasing literature over recent years has demonstrated that young women (1) DO have MIs, (2) present more atypically than men, and (3) are more often misdiagnosed than men. Two recent trials have now also confirmed that young women have a higher in-hospital mortality compared to men, even when properly diagnosed. They may be due to lack of aggressive workups or treatment, or perhaps other as-yet unidentified factors.
The takeaway points are simple: be very wary when women (incuding young women) present with any cardiopulmonary complaints or anginal equivalent-type symptoms; and treat them aggressively.
The American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults is now available.
The update differs in several ways from the 2003 edition. Medications that are no longer available have been removed, and drugs introduced since 2003 have been added. Research on drugs included in earlier versions has been updated and new information is provided about appropriate prescribing of medications for an expanded list of common geriatric conditions.
Here is an abbreviated list of medications/classes on the list that we may use in the ED. Use caution.
If vancomycin resistance is suspected with MRSA infections, there are several other antibiotic choices. They are all extremely expensive.
| Antibiotic | ORAL | Indication | Precaution |
| Telavancin | N | SSTI | May cause QT prolongation: Caution with azole antifungals, class III antiarrhythmics, antidepressants, antipsychotics. Interferes with coagulation tests. |
| Daptomycin | N | SSTI Bacteremia Endocarditis | Not for pneumonia. May cause rhabdomyolysis; Discontinue statins. |
| Linezolid | Y | VAP SSTI | Not for bacteremia. May cause serotonin syndrome; Caution with antidepressants, antipsychotics, tramadol, methadone. |
| Tigecycline | N |
Intrabdominal infections SSTI | Not for bacteremia. Inhibits clearance of warfarin. Reserve for polymicrobial infections. |
Skin and soft tissue infection (SSTI); ventilator acquired pneumonia (VAP)
SBP, HRS, and Albumin
68 yo man presents with new-onset seizures; his CT is shown below. What is your differential diagnosis?
Here's some numbers to consider regarding typical radiation exposre associated with cardiac imaging tests relative to naturally occurring background radiation exposure:
Test type Relative exposure
Naturally occurring annual background radiation
exposure for a person living in the US (~ 3 mSv) 1
Coronary artery calcium score 0.5
Cardiac CT angiography 1-4
Nuclear stress test (single-photon emission CT) 3-4
Exercise treadmiil testing (with no imaging) 0
Cardiac MRI/echocardiogram 0
[above estimates are typical, but may vary between individuals and among different centers]
Luxatio erecta, aka inferior shoulder dislocation, is an uncommon form of shoulder dislocation (0.5-2%)
2 Mechanisms: 1) Forceful, direct axial loading of an ABducted arm.
2) Hyperabduction of the arm leads to impingement of the humeral head against the acromion, If forceful enough, this leverage can rupture the capsule and drive the humeral head downward, resulting in an inferior dislocation. This mechanism is more common.
Classic presentation: Arm locked in marked ABduction with the flexed forearm lying above the head.
http://uconnemig.files.wordpress.com/2011/11/emimages-8c.jpg
http://img.medscape.com/pi/features/slideshow-slide/sdrt/fig1.jpg
http://www.mypacs.net/repos/mpv3_repo/viz/full/76563/3828172.jpg
One may palpate the humeral head against the lateral chest wall
Bony injuries include fractures to surrounding structures such as the coracoid process, acromion, glenoid rim, clavicle, greater tuberosity and humeral head.
Nerve injuries include damage to the brachial plexus/axillary nerve (usually reversed with reduction)
Vascular injuries: Axillary artery thrombosis
Submersion injuries are the 2nd leading cause of accidental death in children with 1/3 of survivors sustaining significant neurologic sequelae. 50% of drownings occur from May to August.
40% of all drowning victims are children under age 4, with males affected 3 times as often as females. Most drownings occur with 10 feet of safety. Infants and toddlers drown most often in bathtubs (especially if <1 year old), buckets, toilets, pools and hot tubs (most often the pools are in-ground). Those with seizure disorders have a 10-14 fold higher likelihood of drowning.
Aspiration of as little as 1-3ml/kg of fluid may cause pulmonary edema, surfactant inactivation or washout, pulmonary shunting with resulting V/Q mismatching, or direct injury to the alveolar membrane.
Immediate and adequate resuscitation, including intubation, is the single most important factor determining survival. Always check body temperature as hypothermia is common. In general, prophylactic antibiotics and steroids are not indicated unless drowning occurred in grossly contaminated water/sewage.
Dexmedetomidine is an alpha2-agonist that has a similiar mechanism of action to clonidine. Short half-life and no respiratory depression make it possibly more effective than propofol in procedural sedation. Cost/Availability are the biggest barriers. Transient bradycardia is also possible but the actual incidence of clinically significant bradycardia is not yet elucidated.
I am still awaiting the first emergency department study looking at dexmedetomidine for procedural sedation.
A recent article actually brought up the possibility of utilizing it intranasally which could have some tantalizing pediatric applications.
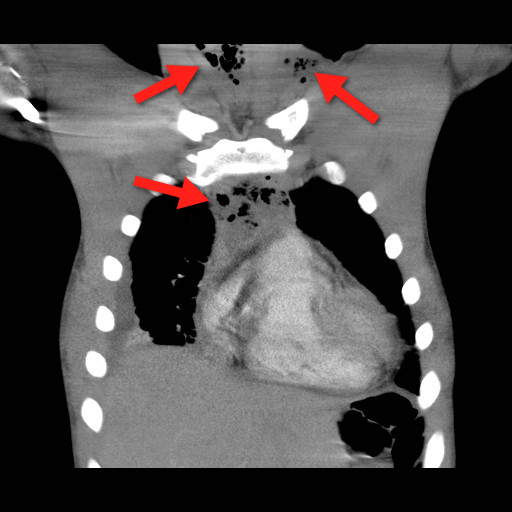
Mediastinitis is an infection of the mediastinum; a rapidly fatal surgical emergency if not recognized and treated early.
Causes include esophageal perforation, oropharyngeal infections (e.g., Ludwig’s angina), prevertebral or carotid space infections, and iatrogenically (endoscopy, hypopharyngeal perforations during intubation, etc.).
Plain films (neck / chest) may serve as a screening tool, but CT best defines the source and extent of disease; the CT below demonstrates gas within the soft-tissues and the mediastinum (red arrrows).
Infections may be polymicrobial and broad-spectrum antibiotics with anaerobic coverage (e.g., pipercillin-tazobacam) should be started initially.
Immediate treatment should also include:
Bonus Pearl
Can't keep up with all the great educational stuff in Emergency Medicine and Critical Care? Let the professionals at Life in the Fastlane do it for you (http://lifeinthefastlane.com). These guys scour the web and blog about the best educational pearls, podcasts, and radoiolgic finds...and they're also quite the laugh. Check them out today!
[Pearl provided by Dr. Semhar Tewelde]
Who are the experts at deciphering ECG's
Authors looked at 240 ECGs which activated the cath lab activation for STEMI. They excluded patients with LBBB or paced rhythms. Retrospective chart reviews were used to determine if there was actually a STEMI. The ECGs were then shown to 7 experienced interventional cardiologists and interpreted for acute STEMI.
Of 84 subjects, there were 40 patients with a true STEMI and 44 without (13 of whom had NSTEMI) Recommendations for immediate PCI varied widely, from 33%-75%. Sensitivities were 53%-83%, specificities 32%-86%, PPV 52%-79%, and NPV 67%-79%. When the cardiologist chose non-ischemic ST elevation, LVH was thought to be the cause in 6% to 31% and old MI/aneurysm in 10% to 26%.
Moral, even cardiologists can be wrong... EM physicians must scrutinize every ECG and challenge ourselves to be the best at interpreting ECG's.
Some quick board review pearls. Remember these fractures/dislocations and the neurologic injury that is associated with them
Children are at higher risk for complications related to the transfusion of blood products compared with adults. So when should we consider transfusion?
Normal hemoglobin values:
- highest at birth (14 - 24 g/dL),
- decreasing to 8 to 14 g/dL at 3 months,
- increasing to 10 to 14 g/dL at age 6 months to 6 years, 11 to 16 g/dL at age 7 to 12 years, and 11.5 to 18 g/dL in adulthood.
- Although the number of platelets are in the normal range at birth, their function is impaired.
For infants younger than 4 months, thresholds for red blood cell transfusions:
- hemoglobin levels are 12 g/dL for preterm infants or term infants born anemic,
- 11 g/dL for chronic oxygen dependency,
- 12 to 14 g/dL for severe pulmonary disease,
- 7 g/dL for late anemia in a stable infant,
- 12 g/dL for acute blood loss exceeding 10% of estimated blood volume.
For infants older than 4 months, thresholds for red blood cell transfusions:
- hemoglobin levels are 7 g/dL in a stable infant,
- 7 to 8 g/dL in a critically unwell infant or child,
- 8 g/dL in an infant or child with perioperative bleeding,
- 9 g/dL in an infant or child with cyanotic congenital heart disease (increased oxygen demand).
- 9 g/dl in children with thalassemia major (to slow bone marrow stimulation)
For children with sickle cell disease (SCD):
- threshold is 7 to 9 g/dL, or more than 9 g/dL if the child has previously had a stroke.
- perioperatively for major surgery: 9 to 11 g/dL, and sickle hemoglobin should be less than 30%, or less than 20% for thoracic or neurosurgery.
Bottom line:
A threshold of 7 g/dL is indicated for the transfusion of packed red blood cells in most children.
Reference:
1) Transfusion guidelines in children. Anasethesia and Intensive Care Medicine. 2012;13(1);20–23.
2) Medscape clinical education briefs
Cuff Pressures and the Prevention of VAP
{kind=link}
{kind=link}
{kind=link}