A recent paper reviewed 53 articles to assess the utility of vasopressors in cardiac arrest. The authors aimed to determine if vasopressors improved ouctomes in this patient population. Here are their conclusions:
Although these conclusions don't support the use of vasopressors in cardiac arrest, we should not abandon these therapies. Most of the trials were completed before wide-spread recognition of the post-cardiac arrest syndrome, implementation of therapeutic hypothermia protocols, and early cardiac catheterization.
Henoch-Schonlein Purpura (aka. Anaphylactoid purpura) is a small vessel vasculitis.
Background:
Clinical Features:
Etiology:
Diagnosis:
Treatment:
Acute, uncomplicated cystitis (in the non-pregnant female):
· The drug of choice is SMX/TMP (provided the resistance rate is <20%) X 3 days.
· An alternative is nitrofurantoin X 5 days.
Acute, uncomplicated pyleonephritis (in the non-pregnanct female) may be treated with:
· Levofloxacin X 5 days, or ciprofloxacin X 7 days (provided resistance rate is <10%).
· Alternatively, SMX/TMP may be used X 14 days.
Crystalloids (i.e., 0.9% saline and lactated ringers) have been used during resuscitation for more than a century. Their invention, however, was more accidental than intentional.
Crystalloids were first used during the European Cholera epidemic of 1831. Hartog Hamburger later modified this solution in 1896 to the solution we know today as "normal" saline. Hamburger's solution was only intended for in vitro study of RBC lysis and was never intended for clinical use.
Around this time, Sydney Ringer was testing several fluids to use for physiologic studies. Ringer's lab assistant was erroneously substituting tap water for distilled water when preparing these solutions. Ringer later discovered that this tap water contained minerals making the solution "physiologic", isotonic, and safe for human use; Alexis Hartmann later added sodium lactate to create Ringer's Lactate.
Since the invention of crystalloids, many types of resuscitation fluids have been created and studied (i.e., albumins, gelatins, and starches); all have been shown to be more expensive, with no more benefit, and with possibly more harm when compared to crystalloids.
The "perfect" resuscitation fluid still alludes us today, but of all of the solutions marketed crystalloids are arguably the best...despite their accidental history.
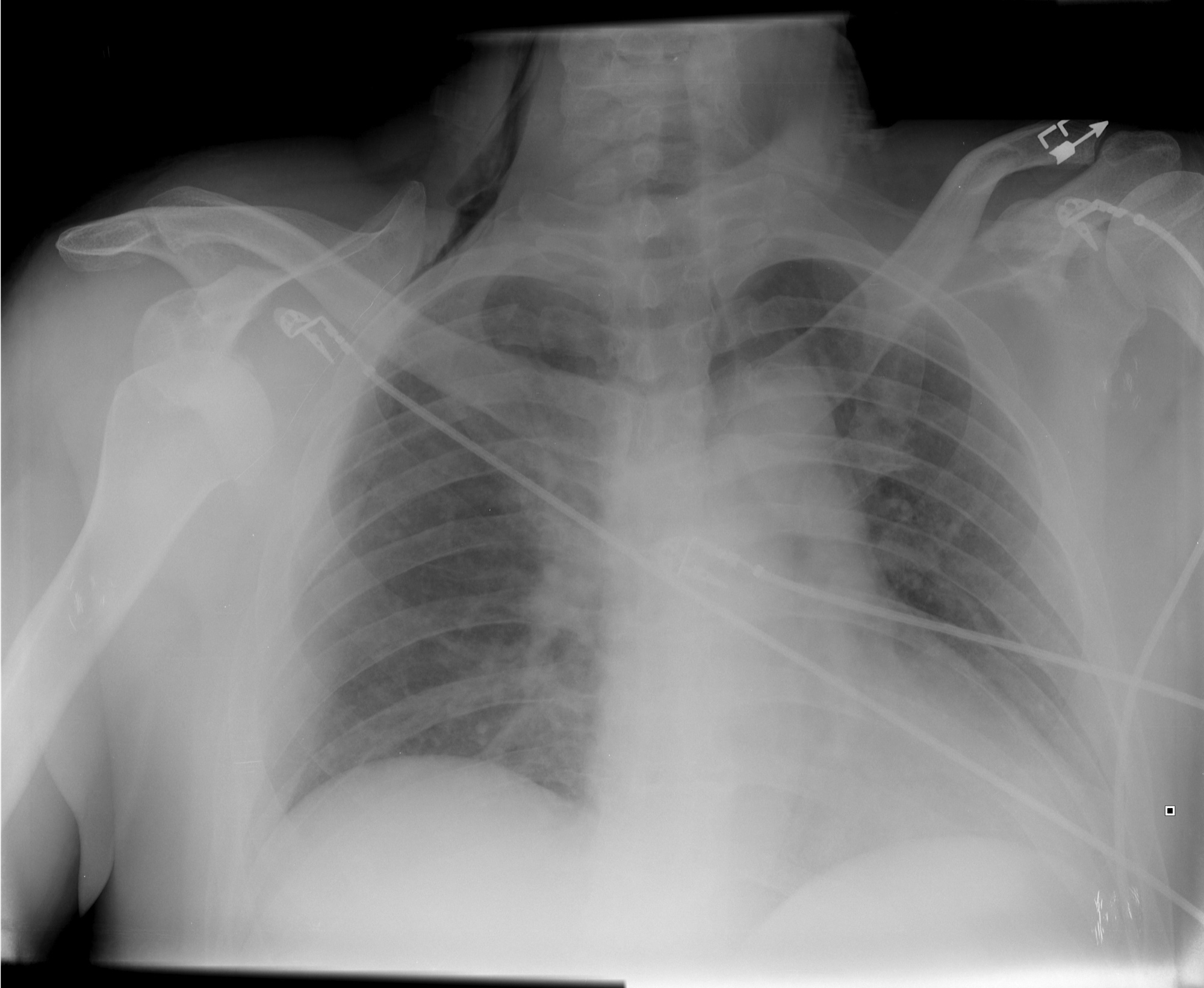
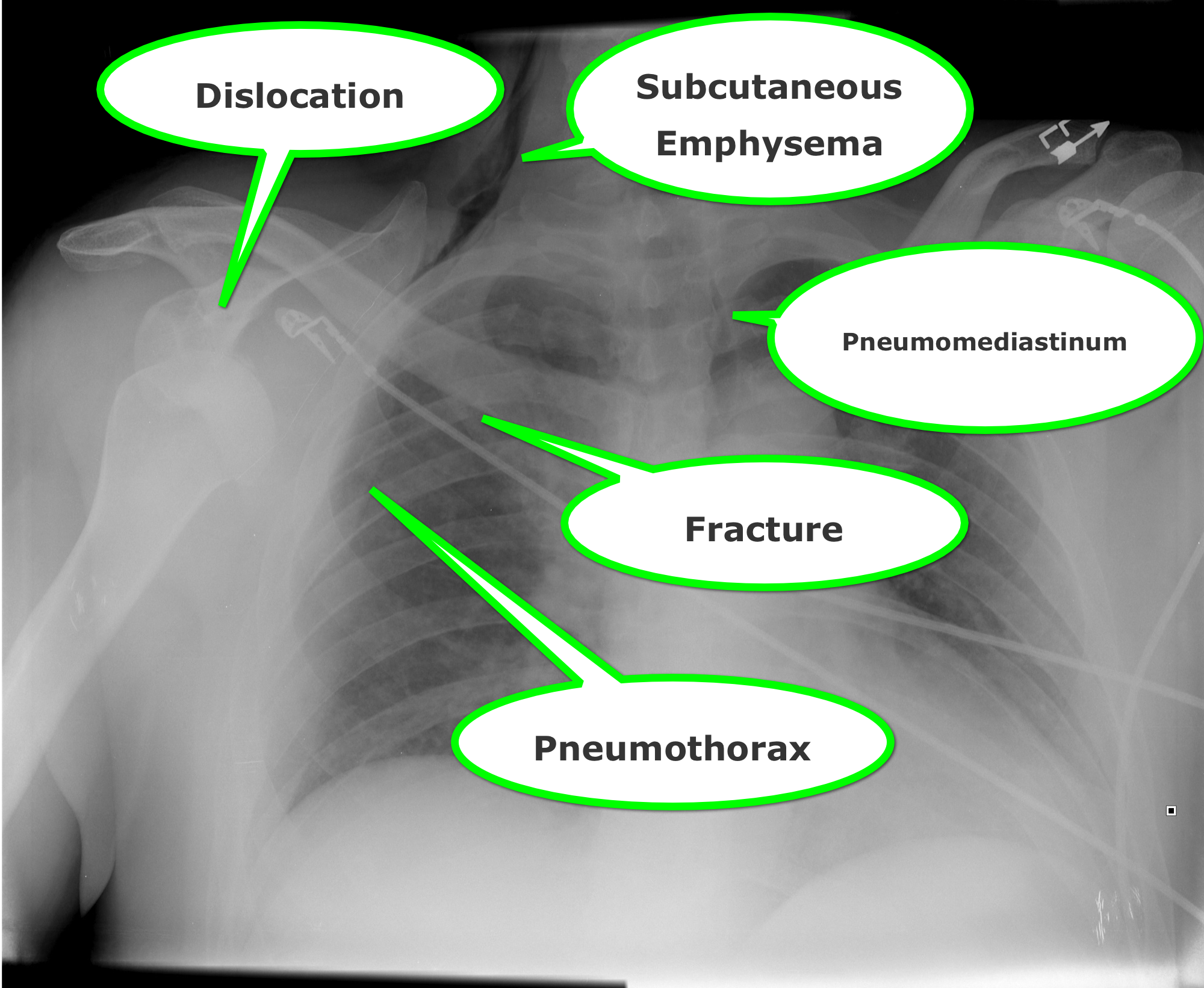
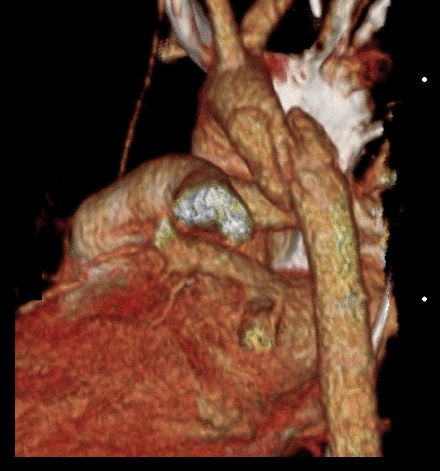
25 year-old male was struck by a car while crossing the street. Chest X-ray and CT Chest with 3D reconstruction are shown below. What's the diagnosis?

Yamaguchi Cardiomyopathy
Yamaguchi cardiomyopathy a.k.a. apical hypertrophic cardiomyopathy (AHCM) was first described 1976 in Japanese patients.
AHCM is a variant of hypertrophic cardiomyopathy that is nonobstructive with predominant involvement of the apex of the heart.
AHCM is frequently misdiagnosed as ACS or STEMI since the typical ECG abnormalities include giant inverted T waves or ST elevation in the mid precordial leads, however coronaries are characteristically clean on cardiac catheterization.
Echocardiography classically used to diagnosis HCM may frequently miss AHCM because hypertrophy is only localized to the apex.
Nuclear magnetic resonance imaging or angiography reveals the pathognomonic "ace of spades" configuration of the left ventricle with systolic obliteration of the apical region.
Unlike HCM sudden cardiac death is very uncommon.
Travel across time zones is regularly required of profession and collegiate athletes (in addition to the some of us professionally)
Jet lag is defined as insomnia or excessive daytime sleepiness/malaise following travel across at least 2 time zones
Symptoms usually persist 1 day for each time zone crossed
The sleep schedule is primarily modulated by light and melatonin
Secretion of melatonin helps induce sleep
Exposure to light stimulates arousal and inhibits melatonin secretion
Who is at risk?
Those with more rigid sleep habits have more symptoms
“Morning” people have less difficulty flying eastward
“Evening” people have less difficulty flying west
However, overall, eastward travel causes the most severe symptoms which persist for up to 7 days (versus <3 days with westward travel)
(The length of the day gets shortened and the circadian system must shorten to reestablish a normal rhythm. The human body demonstrates a natural tendency toward periods longer than 24 hours)
Those with higher levels of physical fitness adjust more quickly
Effects similar in men and women
Midday arrivals experience fewer symptoms than morning arrivals
Symptoms are less in those who have traveled the journey previously
Symptoms are less in those who had a shorter interval their last full nocturnal sleep in the departure city and their first full nocturnal sleep in the destination city
Bonus pearl: Types of Jaundice by Age
- < 24 hrs: hemolyis, TORCH, bruising from birth trauma (ie- cephalohematoma), acquired infection
- Day 2-3: Physiologic
- Day 3-7: infection, congenital diseases, TORCH
- >1 week: Breast Milk Jaundice, breast feeding jaundice, drug hemolysis, hypothyroidism, biliary atresia, hepatitis, red cell membrane disorders (SS, HS, G6PD deficiency)
CIWA-Ar (Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised)
The use of a scoring system for the disposition of an ethanol withdrawal patient can be helpful. The CIWA-Ar Score can guide both treatment in the ED as well as admission versus discharge. Most studies have verified that a score of <8 can be treated outpatient; 8-15 requires treatment and >15 wil require admission/IV benzodiazepines.
N/V: 0-7 (None to Constant N/V)
Tremor: 0-7 (None to Severe even with arms not extended)
Sweats: 0-7 (None to Drenching Sweats)
Anxiety: 0-7 (None to panic attack/delirium)
Agitation: 0-7 (None to pacing/thrashing during interview)
Tactile Disturbance: 0-7 (Mild itching to Continuous Hallucinations)
Auditory Disturbances: 0-7 (None to Continuous Hallucinations)
Visual Disturbances: 0-7 (None to Continuous Hallucinations)
Headache: 1-7 (Miild to Extremely Severe)
Orientation: 0-4
Go to this website to see the actual tool and how it should be administered:
http://www.regionstrauma.org/blogs/ciwa.pdf
Steroids and Septic Shock
Humerus Fractures, Proximal
Wernicke encephalopathy (WE) is a neurologic disorder secondary to prolonged thiamine deficiency; it is characterized by confusion, ataxia, and ocular abnormalities.
Traditional medical teaching advises against the administration of glucose (or glucose containing fluid) in thiamine deficient patients, without first giving thiamine, as this may precipitate WE.
This teaching is problematic, however, in hypoglycemic patients who require the immediate administration of glucose while simultaneously being suspected of thiamine deficiency (e.g., malnourished alcoholics). Delays in treating hypoglycemia may be more harmful (e.g., seizures, permanent neurologic deficits, etc.) than the risk of WE.
Schabelman et. al performed a literature search to unearth the origins of this teaching. Nineteen papers related to this topic were found consisting of case reports, animal studies, and expert opinion; there were no randomized trials, cohort studies, or case-control studies.
Bottom-line: The available evidence does not support withholding glucose treatment until thiamine can be administered and educators should consider abolishing this dogmatic teaching until better evidence is available.
23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" pushups. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)

Atrial fibrillation is most commonly associated with cardiovascular disease
Non cardiac causes: pulmonary disease/PE, hyperthyroidism, sympathomimetics, drugs/ETOH
AFFIRM & RACE trials compared outcomes of a fib patients treated w/ rate vs. rhythm control
- No significant difference in survival between groups
Risk of thromboembolic CVA
- Rhythm control = Rate control + anticoagulation
New data challenges the need for strict heart rate control
- Resting heart rate should be <110 bpm
Use CHADS2 score to identify who requires anticoagulation based on %risk of emboli
- Chronic heart failure, HTN, Age>75, DM, Stroke/TIA
The median nerve is not the only compression neuropathy of the wrist
The ulnar nerve can become compressed at the level of the wrist as it 1) enters Guyon's canal or 2) or as the deep branch curves around the hook of the hamate
Compression can occur due to carpal bone fractures, local inflammation, ganglias, lipomas, anatomic abnormalities, etc
In sports medicine, the most common mechanism is injury is seen in cyclists (cyclist/handlebar palsy)
http://www.hughston.com/hha/b_15_3_2a.jpg
Also seen in those who participate in racquet sports, baseball, and golf
Symptoms can be isolated motor (claw hand = rare), sensory or both
http://en.academic.ru/pictures/enwiki/85/Ulnar_claw.jpg
Can be associated w/ median nerve compression
Tx: Activity modification such as wearing padded gloves, padding the object, or changing hand position on the handlebars
If above fails, surgical decompression is very effective.
Levamisole is a pharmaceutical with anthelminthic and immunomodulatory properties that was previously used in both animals and humans to treat inflammatory conditions and cancer.
It has been identified as a cocaine adulterant in the U.S. since 2003, with the DEA estimating that by 2009 up to 70% of cocaine seized contained levamisole.
Leukopenia, agranulocytosis, and vasculitis are well known complications of levamisole use.
One important complication to keep in mind is the possibility of multifocal inflammatory leukoencephalopathy (MIL). Although no formal case of leukoencephalopathy in the setting of cocaine use has yet been reported, various neurological side effects were described with levamisole therapy, the most concerning complication being MIL.
Anaphylaxis