A Cochrane review of 37 studies concluded that Succinylcholine (SUC) is superior to Rocuronium (ROC) during rapid sequence intubation.
The authors claim that compared to ROC, SUC has a faster onset of action (45 vs. 60 seconds) and overall a shorter duration of action (10 vs. 60 minutes).
Dr. Reuben Strayer wrote a letter to the journal editors and stated that these findings should be interpreted carefully; he highlighted that most of the studies in the review used doses of ROC less than 0.9 mg/kg (most studies used 0.6mg/kg).
Dr. Strayer asserted that ROC’s onset of action is dose dependent; when using doses of 1.2 mg/kg, ROC’s onset is indistinguishable from that of SUC. He also stated another major benefit of ROC is the lack of adverse effects that SUC possesses (hyperkalemia and malignant hyperthermia).
What are your thoughts on this? Go to http://www.facebook.com/Criticalcarenow and take the poll (there are 5 choices). Results will be posted next week.
56 year-old male presents with chest pain. You perform an ultrasound of the heart and see the clip below. What's the diagnosis? Thanks to Dr. Ken Butler for the case.
Arrhythmogenic right ventricular dysplasia (ARVD) is a heritable form of cardiomyopathy, characterized by the replacement of myocytes with adipose and fibrous tissue leading to arrhythmias, right ventricular failure, and sudden cardiac death (SCD)
ECG findings include T-wave inversions in V1–V3 (85% ), epsilon waves (in 33%), as well as a QRS duration >110 ms in V1-V3 (64%)
Apprehension test for shoulder dislocation
Tests for chronic shoulder dislocation
Similar to the patellar apprehension test
Designed to place the humeral head in a position of imminent subluxation or dislocation
http://www.maitrise-orthop.com/corpusmaitri/orthopaedic/112_kelly/kelly-fig11.jpg
ABduct and externally rotate arm to a position where the shoulder may dislocate
If the shoulder is about to dislocate, the patient will experience apprehension due to the familiar pattern of dislocation, report the laxity and resist further motion.
Types:
- Uniphasic anaphylaxis: occuring immediately after exposure to allergen, resolves over minutes to hours and does not recur
- Biphasic anaphylaxis: occuring after apparent resolution of symptoms typically 8 hours after the first reaction. Occur in up to 23% of adults and up to 11% of children with anaphylaxis
Treatment:
1. First line: IM epinephrine 1:1000 solution
- vasoconstrictor effects on hypotension and peripheral vasodilation; bronchodilator effects on upper respiratory obstruction
- NO absolute contraindication for use in anaphylaxis
- Dosage: Adult: 0.3 - 0.5mg; Peds: 0.01mg/kg (max 0.3mg)
- can be repeated every 5-15 minutes
2. Adjunctive therapy:
- H1 Blocker: diphenhydramine 1-2mg/kg up to 50mg IV
- H2 Blocker: ranitidine 1-2mg/kg
- Corticosteroid: 1-2 mg/kg for prevention of biphasic reactions
- Bronchodilator: Albuterol for bronchospasm
- Glucagon: for refractory hypotension or if patient is on beta blocker
- Dosage: Adult: 1-5 mg; Peds 20-30microgm/kg
- Dose may be repeated or followed by infusion of 5-15 mg/min
- place patient in recumbent position if tolerated with lower extremities elevated
- supplemental O2
- IV fluids for hypotension
Fatalities: typically seen with peanut or treenut ingestions from cardiopulmonary arrest. Associated with delayed or inappropriate epinephrine dosing
Disposition:
- Mild reaction with symptom resolution: observe for 4-6 hrs (ACEP, AAP)
- Recurrent symptoms or incomplete resolution: admit
Reference:
1. World Allergy Organization Guidelines for the Assessment and Management of Anaphylaxis, Feb 2011
2. Guidelines for the Diagnosis and Management of Food Allergy in the United States: Report of the NIAID-Sponsored Expert Panel Oct 2010
Patients that experience altered mental status (specifically lethargy) and are on valproic acid - check a serum ammonia level regardless if it is an overdose or just therapeutically on VPA.
If the ammonia is elevated in combination with the mental status change consider administration of L-carnitine either po or IV. It will lower the ammonia and improve the mental status within hours.
High risk patients for hyperammonia who therapeutically take VPA are certain pediatric patients that experience malnutrition, have seizure disorder and are on multiple seizure medications.
AKI and Fluid Balance
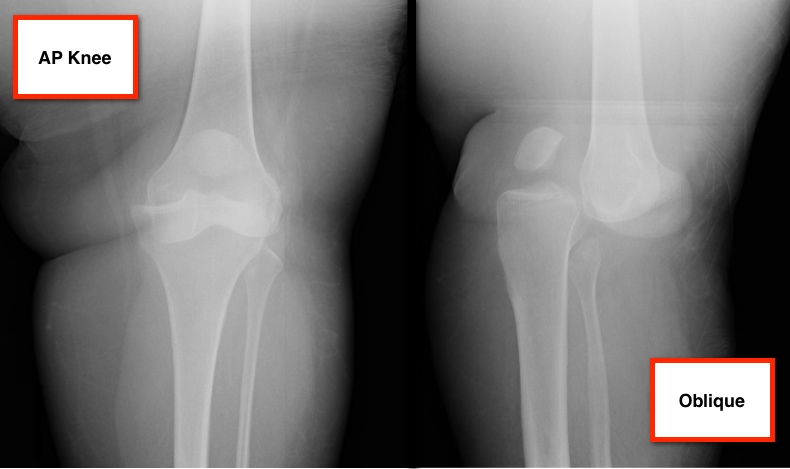
36 year-old female presents with left knee-pain following a motor vehicle crash (XRs are shown). What's the diagnosis AND what is the first test that should be performed to assess for vascular injury?
Pulmonary P waves (S1Q3T3 pattern + clockwise rotation) are specific for PE, but not sensitive.
This study examines if an ECG can discriminate between ACS vs. PE
- 40 patients with PE & 87 patients with ACS
- All had negative T waves in the precordial leads (V1-V4) on the admission ECG
The PE group had negative T waves commonly present in leads II, III, aVF, V1, V2, but less frequent in leads I, aVL, and V5 to V6 (p <0.05).
The ACS group had negative T waves in leads III and V1 in 1% compared with 88% of patients with PE (p <0.001).
Sensitivity, specificity, positive predictive value, and negative predictive value for Dx of PE were 88%, 99%, 97%, and 95%, respectively.
Negative T waves in both leads III and V1 may suggest PE can be differentiated from ACS in patients with negative T waves in the precordial leads.
The Analysis of Synovial Fluid Analysis
When trying to diagnosis a septic joint, it is common to order the following labs on the synovial fluid:
Unfortunately, there is no value of glucose or protein that has enough sensitivity and specificity to make the tests diagnostically helpful. Gram stains are only postive in culture positive septic joints in approximately 50% of the cases. Cultures take too long to be helpful in the ED. The synovial WBC count can be helpful if very high, but a low value does not ensure that the patient does not have a septic joint.
The one test that has been shown to have a Positive Likelihood ratio of Infinity is a synovial lactate level >10. A synovial lactate should be sent on all synovial fluid as a level of 10 and greater makes the diagnosis of septic arthritis, regardless of the gram stain or synovial WBC level.
If you have a patient who meets (or has had close exposure to someone meeting) the clinical case definition of pertussis (a cough lasting at least 2 weeks with one of the following: paroxysms of coughing, inspiratory “whoop,” or post-tussive vomiting) here are some important points to keep in mind:
Vaccination
Testing
Treatment
References:
Altunaiji SM, Kukuruzovic RH, Curtis NC, Massie J. Antibiotics for whooping cough (pertussis). Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD004404. DOI: 10.1002/14651858.CD004404.pub3
http://www.cdc.gov/vaccines/pubs/surv-manual/chpt10-pertussis.html
Femoral venous access is typically limited to the acute resuscitation of critically-ill patients. Several practice-guidelines recommend avoiding the femoral site, or removal once admitted to the ICU, because of the risk of catheter-related bloodstream infection (CRBI) and deep-vein thrombosis (DVT).
A recent systematic review and meta-analysis (including two randomized-control trials and eight cohort-studies) evaluated the risk of CRBI and DVT for catheters placed in either the internal jugular, subclavian, or femoral-venous sites. No difference in the rate of CRBI or DVT was found between the three sites, although the DVT data was less robust (i.e., contained heterogeneous data).
The authors hypothesized that improvements in sterility during central-line placement (e.g., full-barrier precautions), improved nursing care (e.g., central-line site care), and ultrasound guidance may have led to a reduction in femoral site complications.
Although a prospective randomized-control trial is necessary to confirm these results, this meta-analysis challenges the traditional teaching that femoral central-access should be avoided.
Placement of central-lines through the subclavian (SC) route has several advantages over other sites of venous cannulation:
• Lower rates of infection
• Lower rates of deep vein thrombosis
Placing a central-line through the "blind" SC approach increases the risk of non-compressible vessel injury and pneumothorax as compared to other approaches (e.g. internal jugular).
Ultrasound can help place central-lines in the SC vein while reducing the risk of complications; this video demonstrates the technique: http://ultrarounds.com/Ultrarounds/Subclavian_Ultrasound.html
Hypertrophic cardiomyopathy (HCM) is characterized by left ventricular hypertrophy (typically asymmetric) that occurs in the absence of pressure overload or storage/infiltrative disease.
HCM demonstrates remarkable diversity in disease course, age of onset, pattern and extent of LVH, degree of obstruction, and risk for sudden cardiac death.
Patients with HCM are at increased risk for sudden death, annual rate of SCD is ~1%. ICDs are recommended for all patients with prior arrest/sustained ventricular tachycardia (class I recommendation).
Apologies for the long pearl, I did not want to split this into 3 parts)
Disruptions in sleep and circadian rhythms (from travel across time zones and jet lag) are known to alter cognitive functions. Mood and complex mental performance tasks deteriorate faster than do simpler mental performance tasks.
An athlete’s circadian rhythms are believed to be optimal for performance in the early evening (reaction time to light and sound in the fastest). Interestingly, the evening is the time of day when most world records have been broken. However, activities that require fine motor control and accuracy (hand steadiness and balance) are best in the morning.
In the normal population, travel effects are seen in inattention and an increase in errors and injuries in the workplace.
Athletes who perform in international competitions immediately after time zone transitions demonstrate a decline in performance involving complex mental activities, with an associated feeling of lethargy and a general loss of motivation.
British Olympic athletes demonstrated a decrease in leg and back strength in addition to reaction time when traveling westward across 4 time zones. In the NFL, west coast teams consistently beat east coast teams in evening games.
Of course, this type of outcome data is multifactorial and travel effects likely are only one of many complex factors.
Treatment:
Full adaptation to the new time zone is NOT recommended for short trips (1 – 2 days), only for longer stays (> 3 days).
Nonpharmacologic:
Preadaptation and bright light therapy: Remember that exposure to light is the primary cue for circadian rhythms. Bright light exposure in the mornings (after eastward travel) will advance the body clock, while exposure in the evenings (after westward travel) will delay it (Level B).
Shifting the sleep schedule 1 - 2 hours towards the destination time zone in the days preceding departure may shorten the duration of jet lag (Level B).
Strategic napping: Napping in the new time zone during typical sleep times in the destination time zone will delay adaptation. Power naps (20 minutes) may be helpful in decreasing daytime sleepiness in those with jet lag (Level B). The best time to nap (in flight or post flight) is nighttime in the destination time zone (Level B).
Pharmacologic:
Melatonin: Cochrane review concludes that it is safe and effective in both treating and preventing jet lag. It is recommended for adults traveling across 5 or more times zones; and may be effective for travel across 2 to 4 time zones. Take melatonin in the morning when traveling westward, and at the local bedtime when traveling eastward (Level B). Doses of 0.5 to 5mg were similarly effective. Melatonin taken in the evening and at higher doses are effective at inducing sleep (Level A).
Sleep aids: Hypnotic sleep aids reliably induce insomnia secondary to jet lag. Benzodiazepines improve sleep quality but may cause a “hangover” effect the next day, possibly impairing performance.
Ambien (zolpidem) and Lunesta (zopiclone) can be effective while limiting the hangover effect especially in those who have previosly tolerated the medication (Level A). Zolpidem may be more effective than melatonin and placebo at countering jet lag symptoms. Note: the use of both medicines together was not more effective than zolpidem alone but did cause daytime somnolence.
Stimulants: Care should be used in the athlete as most of these medications are banned in competition. There is a potential off label use for Provigil (modafinil) for improving daytime sleepiness associated with jet lag (currently approved for narcolepsy).
Caffeine, while not banned for the World Anti-Doping Agency, is a monitored substance. It increases daytime alertness and may accelerate entrainment in new time zones when consumed in the morning (later ingestion may interfere with sleep induction) (Level A).
There is a growing recognition of patients who have a subtoxic acetaminophen level at the 4-hour mark, but then still go on to have a toxic level later.
This is concerning in that we usually can exclude the chance for toxicity if the 4-hour, post-ingestion level is < 150 mcg/mL following an acute ingestion (plotted on Rumack-Matthew nomogram).
It still is not clear exactly what subset of patients need to have a second level drawn, but a recurring theme seems to be ingestion of acetaminophen in combination with agents that slow GI motility, such as diphenhydramine or opioids. It may be worth ordering a second APAP level (possibly at 8 hours) in patients ingesting these prodcuts.
Lung Protective Ventilator Settings Still Underutilized

Takotsubo cardiomyopathy a.k.a. stress cardiomyopathy is an acute reversible disorder characterized by left ventricular (LV) dysfunction most commonly affecting postmenopausal women
The LV adopts the shape of an octopus trap (“takotsubo”) describing the narrow neck and broad base globular form during systole
Symptoms include precordial chest pain, dyspnea, or heart failure presenting with pulmonary edema mimicking ACS
Mayo Clinic Diagnostic Criteria
- Suspicion of AMI based on symptoms and STEMI on ECG
- Transient hypokinesia or akinesia of the middle and apical regions of LV
- Functional hyperkinesia of the basal region of LV
- Normal coronary arteries (luminal narrowing <50%)
- Absence of recent head injury, ICH, HCOM, myocarditis, or pheochromocytoma
Treatment is symptomatic and determined based on complications during the acute phase; occasionally requiring IABP or ECMO
Prognosis is better than those with ACS, however initial LVEF is similar to those seen with ischemic heart disease