General Information:
• Millions of people around the world (including our patients who travel and victims of disasters like Hurricane Sandy) are exposed to non-potable water.
• How to treat contaminated water:
♦ Filter cloudy water through a clean cloth or allow to settle prior to treatment
♦ The safest method is boiling water vigorously for 1 minute (or, at least 3 minutes at altitudes >6,000ft)
♦ Chemical disinfection is not as effective but, if boiling is not possible, use either:
• 2 drops of unscented bleach (5.52% Cl) per quart/liter of water. (Unknown strength? Add 10 drops per quart/liter.)
-Or-
• 5 drops of tincture of 2% iodine per quart/liter.
- If the water is cloudy or cold, double the chlorine or iodine.
- Notes: Pregnant women or people with thyroid conditions should not use iodine
♦ UV decontamination can be accomplished by leaving clear bottles of water in direct sun for >6 hours or special equipment, but requires clear water
• Boiling, Chlorine/Iodine, and UV will kill viruses, bacteria, and Giardia
• Only Boiling kills Cryptosporidium
Bottom Line:
• If bottled water is available, use it.
• If not, boil your water.
• In order to treat for a wide variety of pathogens, it is best to combine available methods.
University of Maryland Section for Global Emergency Health
Author: Andi Tenner
Managing Critically Ill Patients with AKI
2 year-old male with past medical history of asthma presents with fever and respiratory distress. CXR is shown below. What’s the diagnosis? (Hint: ...look beyond the obvious)

Hematoma blocks for distal radius fractures
Hematoma blocks provide safe, effective analgesia without an increased risk of post procedural infections when compared with other regional blocks
Provide equal reduction quality AND pain control as procedural sedation with Propofol.
However, mean time to reduction (0.9 vs. 2.6 hours) and time to discharge post procedure (0.74 vs. 1.17 hours) were reduced with hematoma blocks.
Consider this option next time the department is busy or the patient is not an ideal procedural sedation candidate.
University of Maryland Section for Global Emergency Health
Author: Emilie J.B. Calvello, MD, MPH
A low-tidal volume (or protective) strategy of mechanical ventilation (i.e., tidal volume of 6-8cc/kg of ideal body weight) has previously been demonstrated to be beneficial in patients with acute respiratory distress syndrome (ARDS).
A meta-analysis was recently performed to determine whether this strategy of mechanical ventilation is also beneficial for patients without lung injury prior to initiation of mechanical ventilation.
Dr. Neto, et al. performed a meta-analysis of 20 studies (total of 2,822 mechanically ventilated patients) comparing a conventional ventilation strategy (average tidal volume was 10.6 cc/kg) to a protective ventilation strategy (average tidal volume was 6.4 cc/kg) of mechanical ventilation.
The authors concluded that patients ventilated with a protective lung-strategy had reductions in:
Bottom-line: This meta-analysis supports the notion that a strategy of low-tidal volume ventilation may have benefits for patients without ARDS, however prospective studies are needed.
Do you like placing ultrasound-guided IV catheters? Check out this trick for covering the probe during the procedure.
http://ultrarounds.com/Ultrarounds/The_Vascular_Probe_Protector.html
or
https://www.youtube.com/watch?v=ZuOq6Ea_FbA&feature=plcp
Tarsal Tunnel Syndrome (TTS)
Prior pearls have addressed Carpal Tunnel Syndrome and Cubital Tunnel Syndrome, which affect the median and ulnar nerves, respectively. Tarsal tunnel syndrome, is a similar compression neuropathy of the tibial nerve as it transverses through the tarsal tunnel of the foot.
The tarsal tunnel is located behind the medial malleolus, and is where the posterior tibial artery, tibial nerve and several tendons transverse. Patients will present complaining of numbness of the foot radiating into Digits 1-4, pain, burning , and tingling of the base of the foot and heel. TTS has many causes and is more common in athletes.
Consider the diagnosis in patients with foot pain and numbness. If interested in more information about TTS please consider reading this eMedicine article, http://emedicine.medscape.com/article/1236852-overview
A 1 year old gets sent from their pediatrician’s office for rule out meningitis. They presented with fever for 2 days and neck rigidity. Your LP results are normal. What additional test should you consider?
· Explosions can cause a complex series of injuries, which may include subtle or delayed findings. Repeated evaluations, such as serial abdominal exams, may be required.
· Blast injuries are divided into 4 categories:
o Primary blast injuries: Injury from blast wave over-pressure. Found in gas filled structures (ear, lung, hollow organs)
o Secondary blast injuries: Injury from thrown objects (primarily penetrating trauma, but may blunt)
o Tertiary blast injuries: Injuries from patient being thrown by blast wave (blunt trauma)
o Miscellaneous (quaternary) blast injuries: Injuries from other causes, such as burns, crush injuries, rhabdomyolysis, and toxic chemicals.
· The most common primary blast injury is tympanic membrane rupture.
University of Maryland Section for Global Emergency Health
Author: Jon Mark Hirshon
Burn Patients and Antibiotic Dosing
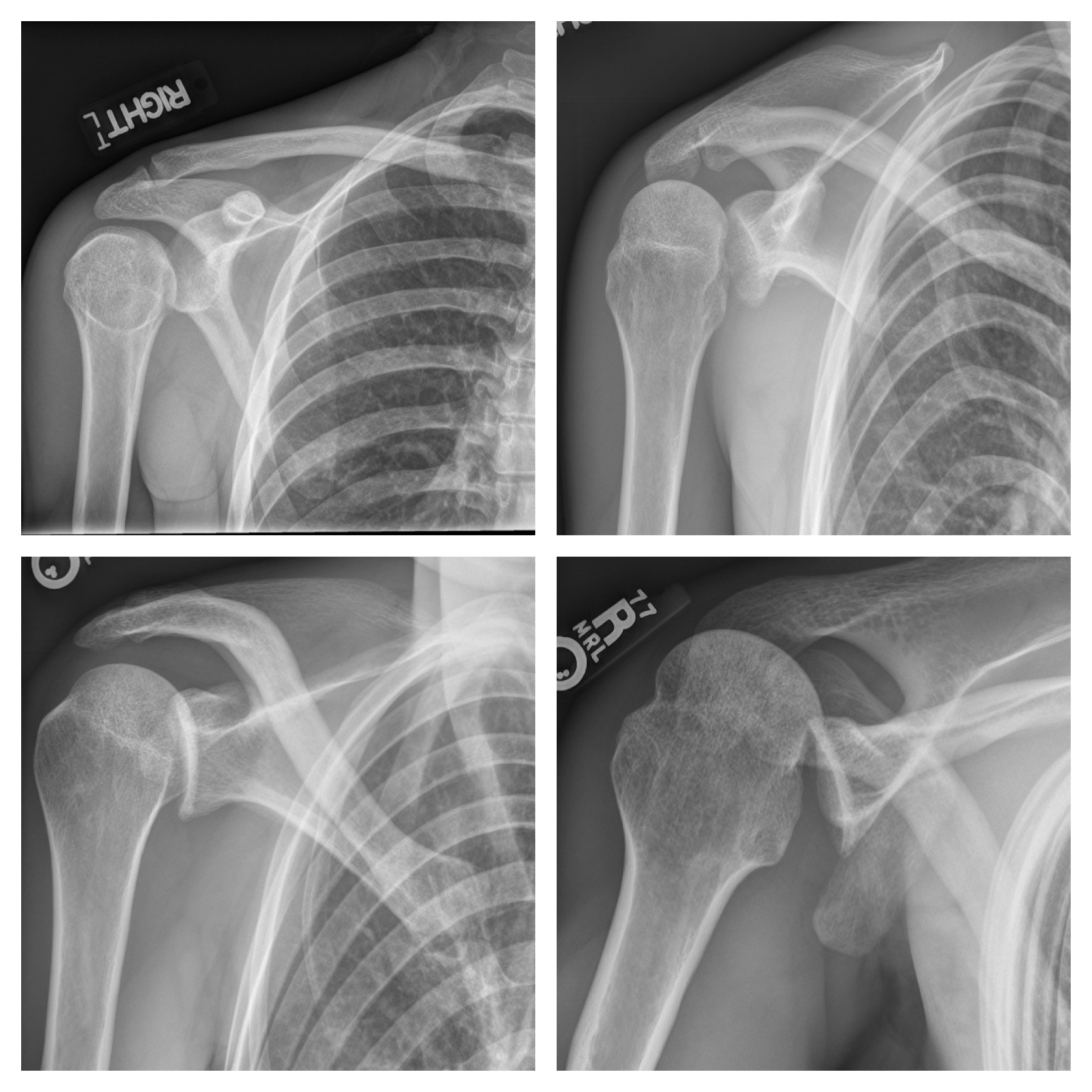
33 year-old male found unconscious by EMS and complains of right shoulder pain upon waking up in the ED. Diagnosis?
Injury is often caused by sudden dorsiflexion on a plantar flexed foot w/ the knee in extension or similarly sudden knee extension with the ankle in a dorsiflexed position.
Injury has a predilection for the poorly conditioned middle-aged athlete, with "thick calves" who are engaged in strenuous activity
Strains are treated with ice, analgesics, and compression (decreases hematoma size and facilitates healing)
Also, consider casting/splinting as dictated by injury severity, such as with a night splint or a CAM boot.
Severe strains and ruptures can be splinted in plantar flexion for 3 weeks.
Background
Patients who are intoxicated with, or emerging from, phencyclidine (PCP) highs present with acute agitation that can be challenging to treat
Risks of physical restraints for combative patients include injury, hyperthermia, rhabdomyolysis, and increased agitation or excited delirium
Haloperidol is an option for chemical restraint that is typically safe and rapid acting
Some concerns related to haloperidol use in PCP-intoxicated patients include worsened PCP-induced hyperthermia, dystonic or anticholinergic reactions, lower seizure threshold, and hypotension
Data
A recent retrospective case series assessed the frequency of adverse effects from the combination of PCP and haloperidol
Of 59 cases, only two patients experienced an adverse reaction, and neither could be conclusively linked to haloperidol administration
This analysis had several major limitations including retrospective design for identifying adverse reactions, potential for false positive PCP screens, and possible haloperidol administration more than 24 hours after PCP intoxication
Bottom Line
While haloperidol may be safe for agitated PCP-intoxicated patients, this paper adds nothing to refute or support its use. Benzodiazepines and calm environment are still first-line therapy.
It should be noted that no data exist showing poor outcomes in PCP-intoxicated patients administered haloperidol, which begs the question "Is there even an issue?" Dr. Leon Gussow, author of The Poison Review, provides a nice answer and summary of the article here.
University of Maryland Section for Global Emergency Health
Author: Andi Tenner
Previous pearls have described the increasing evidence against colloid (e.g., hydroxyethyl starch) use during resuscitation. Now it appears that the crystalloid 0.9% normal saline (NS) may be under fire.
The use of large volumes of NS has been associated with hyperchloremic metabolic acidosis and harm in animal studies. The risk of harm in humans, however, has been less clear.
Bellomo et al. conducted a prospective observational study in which patients being resuscitated in the control group received NS at the clinicians' discretion; i.e., chloride-liberal strategy. The use of NS was restricted in the intervention group, where other less chloride containing fluids were used for resuscitation (e.g., Ringer's Lactate); i.e., a chloride-restrictive strategy.
The authors found that when compared to patients in the chloride-liberal group, the chloride-restrictive group had significantly less rise in baseline creatinine, less overall AKI, and a reduced need for renal replacement therapy.
Bottom line: Although this was only an observational study, the liberal use of normal saline during resuscitation may increase the risk of AKI and renal replacement therapy.

