Just before you upgraded your old computer, recall what happened when you had Excel, Word and PowerPoint all open at the same time. In the concussed state, the brain is essenatially functioning like your old computer... and the more tasks it must perform, the slower it will work and slower it will recover. Hence the concept of cognitive rest. Below is taken from the AMSSM position statement of concussion in sport.
Return to school
There are no standardized guidelines for returning the injured athlete to school. If the athlete develops increased symptoms with cognitive stress, student athletes may require academic accommodations such as a reduced workload, extended test-taking time, days off or a shortened school day.
Some athletes have persistent neurocognitive deficits following a concussion, despite being symptom free. Consideration should be made to withhold an athlete from contact sports if they have not returned to their ‘academic baseline’ following their concussion (level of evidence C).
The CDC developed educational materials for educators and school administrators that are available at no cost and can be obtained via the CDC website. Additional resources for academic accommodations should be developed for both clinicians and educators (level of evidence C).
Adam Friedlander shared the practical application of this which I found amusing:
" I always recommend what Peds neuro called "a brain holiday" - my favorite part. All of our nurses look at me like I'm nuts, but it is now on our official concussion/CHI DC instructions. I always say to the kiddo: "You'll love this part. No homework, no reading." Then I turn to mom and dad and tell them they'll love the next part: "No TV, no video games."
Thank you for sharing Adam!!
Luu JL, Wendtland CL, Gross MF, et al. Three percent saline administration during pediatric critical care transport. Ped Emerg Care 2011;27(12):1113-1117
Typical opioid withdrawal include clinical symtpoms of piloerection, nausea, vomiting and diarrhea. If you were to see seizure, another etiology other than opioid withdrawal should be investigated.
Except in the case of neonates borne to women who have been taking opioids chronically such as a methodone patient. Once the child is born, symptoms of withdrawal may take days to weeks to materialize though seizures typically occur <10 days. The child is at increased risk of SIDS as well.
Japanese Encephalitis
Managing Traumatic Hemorrhagic Shock
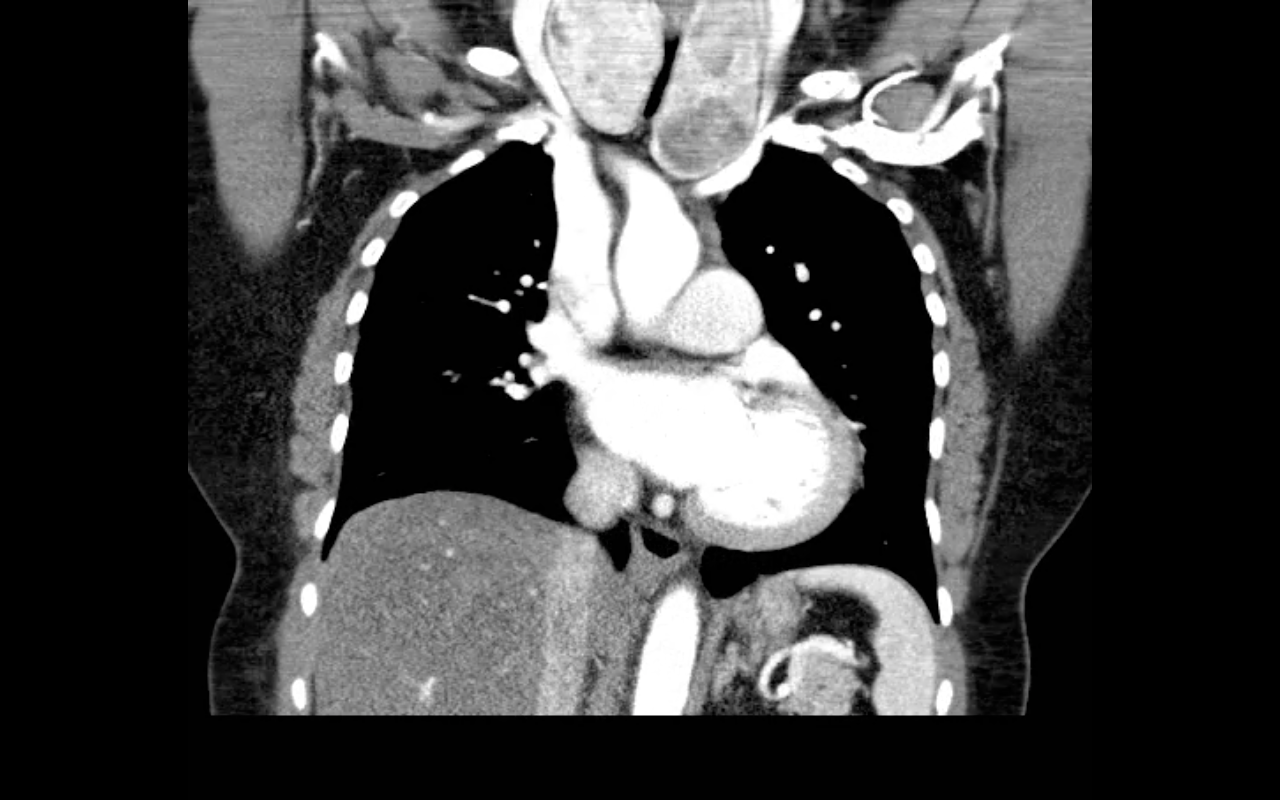
68 year-old female presents with stridor and palpable goiter. Here's a clip from CT of the chest. What's the diagnosis?
Most antidotes have not been adequately studied in pregancy and hold a Pregnancy Risk Category 'C' by the FDA. However, there are a few antidotes that hold a category 'D' or 'X' rating (contraindicated).
In most cases, the benefits of short-term use probably outweigh the risk, especially when accounting for the health and prognosis of the mother.
- The most common disease producing enzymopathy in humans
- Affects 400 million people worldwide
- Highest prevalence is among persons of African, Asian, and Mediterranean descent
- Patients can be asymptomatic but may present with symptoms of acute hemolytic anemia, which may be precipitated by certain medications (Oxidative medications) or foods (some types of beans)
- Avoid oxidative drugs (consult your PharmD when your patient has G6PDd)
- Diagnosis: Measure the actual enzyme activity of G6PD rather than the amount of the enzyme. A more practical test is the presence of Indirect hyperbilirubinemia, but it is non specific
- Treatment consists of oxygen and bed rest in minor cases. However, severe cases may require PRBC transfusion
Propofol is generally a well-tolerated sedative / amnestic but occasionally it can lead to the propofol infusion syndrome (PRIS); a metabolic disorder causing end-organ dysfunction.
Suspect PRIS in patients with increasing lactate levels, worsening metabolic acidosis, worsening renal function, increased triglyceride levels, or creatinine kinase levels. End-organ effects include:
The true incidence of PRIS is unknown, however, certain risk factors have been identified:
Prevent PRIS by using adequate analgesia (with morphine or fentanyl) post-intubation, which may reduce the overall dosage of propofol ultimately reducing the risk.
If PRIS develops, stop propofol and provide supportive care; IV fluids, ensuring good urine output, adequate oxygenation, dialysis (if indicated), vasopressor and inotropic support.
A 25 year-old female presents complaining of a "net-like" rash bilaterally on her medial thighs. She denies any pain but states that the rash looks “pretty scary” What's the diagnosis?

-Common life-threatening cardiovascular effects of cocaine intoxication include tachydysrhythmias, ventricular fibrillation, myocardial ischemia, and infarction.
-Emergency management of acute cocaine intoxication relies mainly on supportive and symptomatic treatment, w/liberal use of gamma-aminobutyric acid receptor agonists such as benzodiazepines.
-Intravenous lipid emulsion (ILE) therapy has been used successfully to treat cardiac toxicity associated with a variety of lipid-soluble drugs, such as local anesthetics, calcium/beta-blockers, tricyclic anti-depressants, and cocaine.
-The current hypothesis, called the “lipid sink” hypothesis, suggest that ILE infusion creates an expanded lipid phase in the plasma that absorbs the circulating lipophilic toxin and decreases the amount of free unbound toxin available to bind to the myocardium.
-When life-threatening cardiac arrhythmias (e.g. wide-complex tachycardia/prolonged QT) are not amenable to standard therapy (e.g. sodium bicarbonate/magnesium) consider ILE as a potential option to the current algorithm.
Estimated 3.8 million sport-related concussions per year (likely significantly higher due to underreporting)
Most patients recover within a 7-10 day period
** Children and teenagers require more time than college and professional athletes
This "accepted" time for recovery is not scientifically established and there is a large degree of variability based on multiple factors including age (as above), sex & history of prior concussions
Approximately 10% of athletes have persistent signs and symptoms beyond 2 weeks (which may represent a prolonged concussion or the development of post-concussion syndrome)
During this time the patient should have complete rest from all athletic activities, close follow-up with PCP and be educated re concussions.
If practical, "cognitive rest" should also be prescribed. This is one of the most frequently neglected aspects of post-concussion care and will be discussed in a future pearl.
Just a quick clarification to last week's melioidosis pearl:
An astute reader noted the typo: "The patient should also be covered for melioidosis, and infection caused by Burkholderia pseudomallei." The sentence should read "...meliodosis, an infection caused by Burkholderia pseudomallei."
Just to clarify, melioidosis is caused by the bacteria Burkholderia pseudomallei.
Many apologies for any confusion this might have caused.
Thanks for reading!
Andi Tenner, MD, MPH
Background Information:
Active tuberculosis (TB) develops in 5-10% of individuals who become infected with M. tuberculosis, typically after a latency period of 6-18 months (but sometimes decades later). Compliance with the 9 month self-supervised isoniazid (INH) regimen has been porr with completion rates <60%. Until recently, daily rifampin for 4-6 months has been the only alternative when the bacterium is resistant or INH cannot be used.
Pertinent Study Design and Conclusions:
Bottom LIne:
A substantially shorter course of therapy with INH-RPT is now the recommended treatment for latent TB.
University of Maryland Section of Global Emergency Health
Author: Emilie J. B. Calvello, MD, MPH
Needle Decompression - Are we Teaching the Right Location?
40 year-old male presents with fever, chills, & cough. What’s the diagnosis and the MOST likely cause?
Intraosseus (IO) access has become quite popular in critically ill patients requiring immediate resuscitation. In a patient responsive to pain, however, pain and discomfort is associated with the force of high-volume infusion through the established line.
Before flushing the line, consider administering preservative-free 2% lidocaine (without epinephrine) for patients responsive to pain prior to flush.
The suggested dose is 20-40 mg (1-2 mL) of the 2% lidocaine, followed by the 10 mL saline flush.
If preservative-free 2% lidocaine is not stocked in your ED, now is the time to consider adding it.