Keep Immune Thrombocytopenic Purpura (ITP) in your differential for patients with thrombocytopenia and evidence of bleeding. Although ITP has classically been described in children, it can occur in adults; especially between 3rd- 4th decade.
Thrombocytopenia leads to the extravasation of blood from capillaries, leading to skin bruising, mucus membrane petechial bleeding, and intracranial hemorrhage.
ITP occurs from production of auto-antibodies which bind to circulating platelets. This leads to irreversible uptake by macrophages in the spleen. Causes of antibody production include:
Suspect ITP in patients with isolated thrombocytopenia on a CBC without other blood-line abnormalities. Abnormality in other blood-line warrants consideration of another diagnosis (e.g., leukemia).
ITP cannot be cured; treatments include:
Stanford type A (proximal) aortic dissection accounts for ~60% of all aortic dissections
Classic treatment includes direct surgical replacement of the ascending aorta w/prosthetic graft (+/- AV aortic repair/replacement)
~20-30% of these patients (*institutional dependent) are considered poor candidates for surgery and receive only medical management, which innately results in substandard outcomes
In this study those who were considered poor candidates for surgical repair underwent novel endovascular treatment
Endovascular repair in this study was considered both appropriate and improved traditional medical outcomes in patients who were considered poor candidates
Trapezium Fractures
Suspect the Diagnosis when you note
If you are suspected the diagnosis oblique radiographs or a CT scan of the wrist will note the fracture the best.
Treatment consists of placing the patient in a thumb spica splint.
In the treatment of acetaminophen poisoning with N-acetylcysteine (NAC), the PT/INR can be slightly elevated even in the absence of hepatotoxicity. Considering Prothombin Time (PT) is one of the criteria used to assess severity of liver damage in this setting, it is important to know how much the PT/INR can be affected by NAC and if it has an actual effect on coagulation factor levels.
Clinical Practice Pearls
General Information:
-Listeria can cause serious infections in vulnerable groups: adults >65 years old, pregnant women, newborns, immunocompromised
-In a recent CDC report, infection with Listeria was associated with a 20% mortality rate.
Clinical Presentation:
- History of cantaloupe, soft cheese, or raw produce ingestion
- Non-specific symptoms: fever, myalgias, occasionally preceded by GI symptoms
-Can have headache, stiff neck, confusion, AMS, miscarriage or stillbirth in pregnant women
Diagnosis:
- Blood, CSF, or amniotic fluid culture showing Listeria monocytogenes
- Listeria is a reportable disease
Treatment:
- Ampicillin and Penicillin G are the drugs of choice
- Add gentamycin in CSF infection, endocarditis, the immunocompromised, and neonates.
Bottom Line:
Listeria infections have a high mortality rate and can be found worldwide. Suspect in patients who have febrile syndromes and travel to areas where they may consume unpasteurized cheese.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Rhabdomyolysis in the Critically Ill
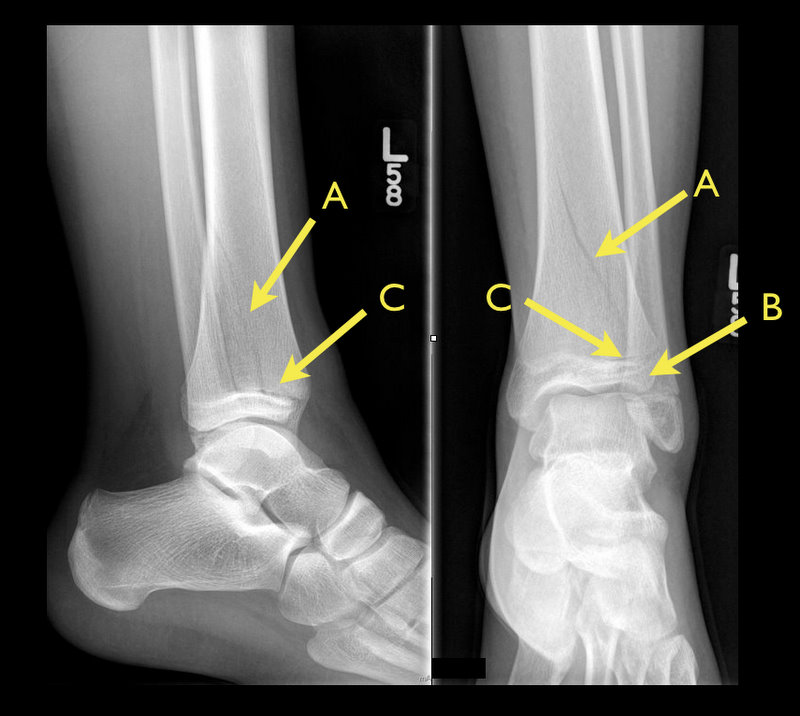
13 year-old female with ankle pain following fall down escalator. What's the diagnosis?

The adolescent brain has not yet reached full maturation and is in a period of rapid development from ages 14 - 16.
Adolescents have been found to be more sensitive to the effects of concussion than adults
Concussed adolescents have deficits in attention and executive function lasting up to 2 months post injury.
Be aware that the adolescent brain will require extended recuperation time following injury
In the future, discharge instructions might need to say more than "don't get hit in the head till your headache goes away." Because of deficits in attention and executive function, physicians should consider recommendations about adolescents and jobs, school work and driving an automobile.
Infant lumbar puncture is often difficut and may require repeated attempts. The traditional body positioning is lateral decubitus. Previous studies have examined the saftey of having the patient in a sitting position, and neonatal studies have suggested that the subarachnoid space increases in size as the patient is moved to the seated position. A study by Lo et al published last month looked to see if the same held true in infants.
50 healthy infants less then 4 months old had the subarachnoid space measured by ultrasound between L3-L4 in 3 positions: lateral decubitus, 45 degree tilt and sitting upright.
This study found that the size of the subarachnoid space did not differ significantly between the 3 positions. Authors postulated that a reason for increase sitting LP success rate that had been reported in anestesia literature with tilt position could be due to other factors such as increased CSF pressure, intraspinous space widening or improved landmark identification.
General Information:
-The global health world is faced with an unprecedented challenge of a trio of threats:
1. Infections, undernutrition, reproductive health issues
2. Rising global burden of non-communicable diseases and risk factors
3. Challenges arising from globalization (climate change and trade politics)
-Definitions of global health are variable and can emphasize anything from types of health problems, populations of interest, geographic area or a specific mission. This makes governance and analysis difficult.
-During the past decade there has been an explosion of more than 175 initiatives, funds, agencies, and donors. Health is increasingly influenced by decisions made in other global policymaking areas.
-The major governance challenges for global health are:
1. Defining national sovereignty in the context of deepening health interdependence
2. Maximizing cross-sector interdependence
3. Developing clear mechanisms of accountability for non-state actors
Relevance to the US physician:
The Global Health System and its governance affects our ability to work effectively within the US and how we structure efforts to expand the reach of timely, effective emergency care worldwide.
Bottom Line:
The Global Health System has become more complex. Any development of Emergency Care Systems must take into account the complexity of actors in the field of global health.
The University of Maryland Section of Global Emergency Health
Author: Emilie J. B. Calvello, MD, MPH
Therapeutic hypothermia (TH) following out-of-hospital cardiac arrest (OHCA) has increasingly been utilized since it was first described. TH following in-hospital cardiac arrest (IHCA), on the other hand, is not as commonplace or consistent despite a recommendation by the American Heart Association (AHA).
A recent prospective multi-center cohort-study demonstrated that of 67,498 patients with return of spontaneous circulation (ROSC) following IHCA only 2.0% of patients had TH initiated; of those 44.3% did not even achieve the target temperature (32-34 Celsius).
The factors found to be most associated with instituting TH were:
Bottom-line: Hospitals should consider instituting and adhering to local TH protocols for in-house cardiac arrests.
Ever wonder how to place a pigtail catheter?
Check out this video to learn how, click here
Background
In the current era of community-acquired MRSA (CA-MRSA), most of our outpatient treatment options for cellulitis aim to cover MRSA. Choices include sulfamethoxazole/trimethoprim (SMZ-TMP), doxycycline, linezolid, and clindamycin (depending on local susceptibility patterns).
A New Study
Take Home Clinical Points
Hyperglycemia in the setting of antipsychotic use has been reported mostly with olanzapine (Zyprexa) but does occur with other antipsychotics. A recent study from the NYC medical examiner's office details 17 deaths of DKA due to antipsychotics and found that (from highest to lowest incidence) quetiapine > olanzapine > risperidone were the atypical antipsychotics found with these deaths.
Remember hyperglycemia occurs with patients on antipsychotics and can lead to hyperglycemia hyperosmolar coma or DKA. Both can be lethal.
Background Information:
Each year, an estimated 50 million travelers from Western countries visit tropical regions all over the world.
Given the potentially serious consequences for the patients and, their close contacts and healthcare workers it is important that life threatening tropical diseases are swiftly diagnosed.
Pertinent Study Design and Conclusions:
- Descriptive analysis of acute and potentially life threatening tropical diseases among 82,825 ill western travelers reported to GeoSentinel from June of 1996 to August of 2011.
- Of these travelers, 3,655 (4.4%) patients had an acute and potentially life threatening disease.
- The four most common conditions being falciparum malaria (76.9%), typhoid fever (11.7%), paratyphoid fever (6.4%), and leptospirosis (2.4%).
Bottom Line:
Western physicians seeing febrile and recently returned travelers from the tropics need to consider a wide profile of potentially life threatening tropical illnesses, with a specific focus on the most likely diseases described in this case series.
University of Maryland Section of Global Emergency Health
Author: Walid Hammad, MB ChB
End-expiratory Occlusion Test