These two Ethiopian boys present with “back problems”. What are the diagnoses and what do you need to worry about with each of them?

The Crashing Cardiac Transplant Patient
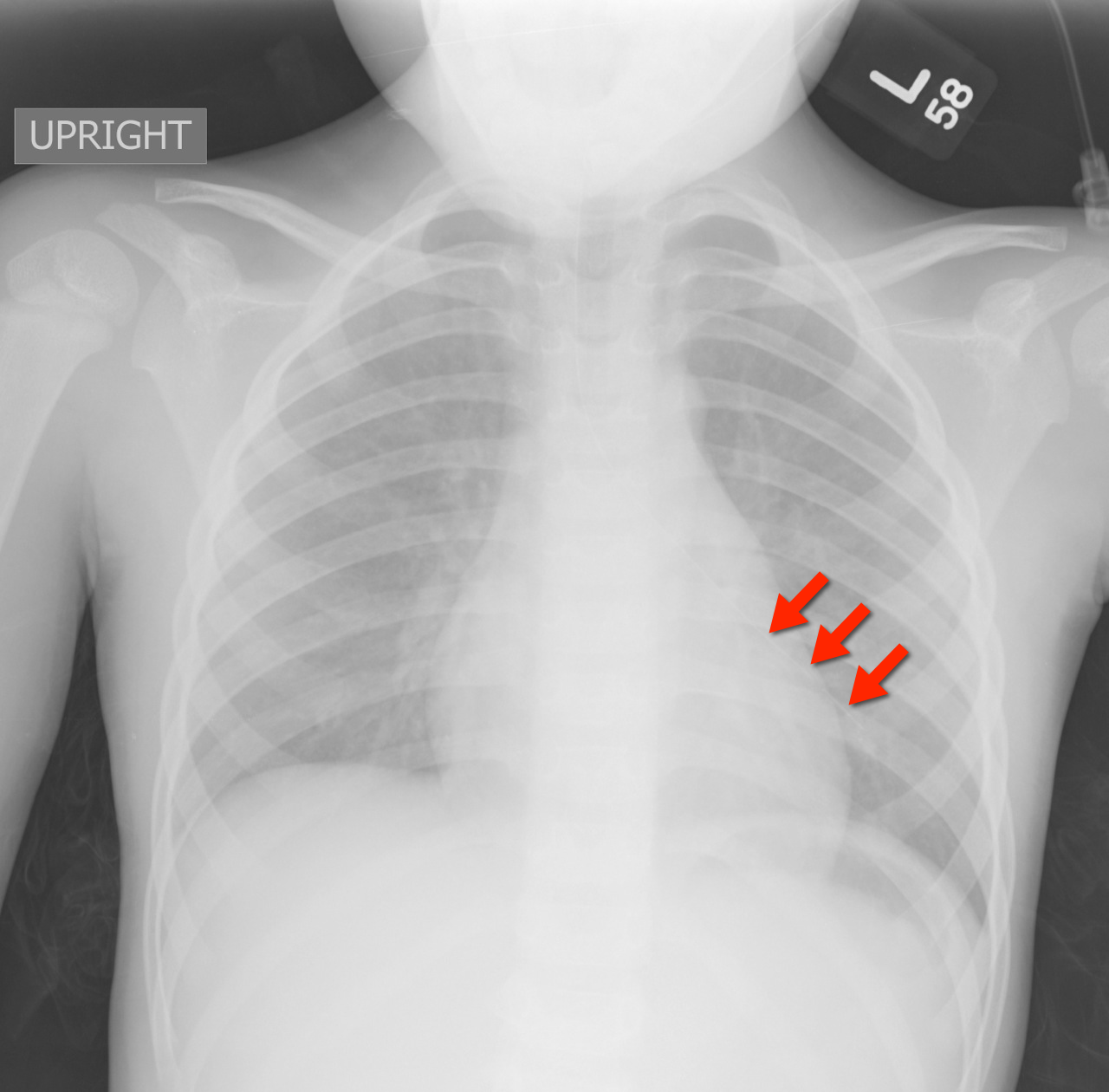
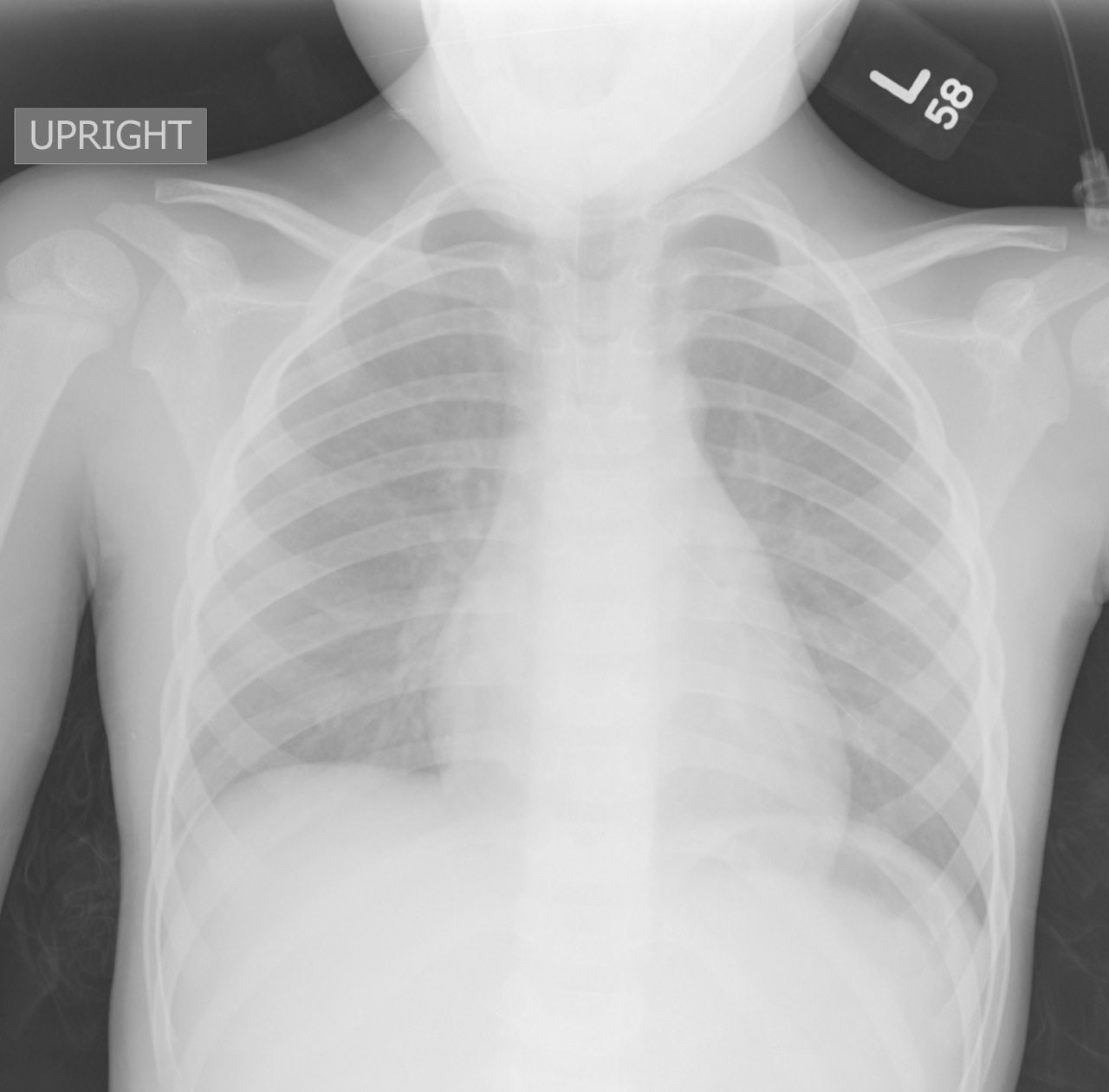
4 year-old female with the post-procedural CXR shown below. What's the diagnosis? (Hint: use the zoom...this one is tricky)
The two available Tetanus/reduced diphtheria toxoid/acellular pertussis (Tdap) vaccine products in the U.S. are Boostrix and Adacel. Neither were originally approved in older adults age 65 and older. Boostrix received FDA-approval for use in this age group in July 2011, but Adacel never has.
However, in June 2012 ACIP issued new guidance recommending Tdap for all adults age 65 years and older.
"When feasible, Boostrix should be used for adults aged 65 years and older; however, ACIP concluded that either vaccine administered to a person 65 years or older is immunogenic and would provide protection. A dose of either vaccine may be considered valid."
Bottom line: Regardless of which Tdap product is stocked at your institution, both are considered safe to use in adults 65 years and older.
Rotavirus is the leading cause of gastroenteritis worldwide and a leading cause of infant death in the developing world.
95% of U.S. children have had a rotavirus infection by the age of 5 years.
Most cases occur in late winter and early spring.
Route of transmission is mostly fecal-oral but may be airborne in cooler months.
Most common presenting signs and symptoms include fever (1/3 of cases), vomiting (in the first 1-2 days), and diarrhea (copious, watery, lasting 5-21 days).
Diagnosis is largely based on clinical manifestations, but antigen assays are available and may be useful in patients with extraintestinal complications, such as hepatitis, pneumonitis, or encephalopathy.
Treatment is largely supportive with efforts to maintain hydration.
Prevention is key to disease control and accomplished with good hand hygiene and widespread vaccination.
Newly implemented vaccine programs worldwide have proven to be effective in decreasing hospitalizations and deaths in developing countries.
Creatine
Adverse effects: weight gain, edema, GI cramping, fatigue and diarrhea
General Information:
-Leptospirosis is a tropical infectious disease that is also endemic in the US. (Estimated 16% seroprevalence in inner city Baltimore!)
-The spirochete is spread through animal urine and can survive in water or soil for weeks.
-Risk factors: rural exposure to animal urine (farming, adventure sports) or urban exposure to rat urine.
-Infection is acquired through breaks in the skin or mucus membranes
-Outbreaks are often seen following rain or floods.
Clinical Presentation:
-Non-specific febrile illness (usually not diagnosed in these cases)
-If untreated, 5-10% progress to jaundice, renal failure, thrombocytopenia, hemorrhage, and respiratory failure.
Diagnosis:
- Primarily based on clinical presentation and history
- Paired serum sent to CDC (the acute serum sample should be drawn in the ED)
Treatment:
- Doxycycline, Ceftriaxone and Penicillin are all effective
Bottom Line:
Consider and treat for Leptospirosis in patients with possible exposure animal urine (especially after a flood) who present in extremis with renal failure, jaundice, and thrombocytopenia.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms) or DIHS (Drug-Induced Hypersensitivity Syndrome) is a potentially life-threatening adverse drug-reaction.
Incidence is 1/1,000 to 1/10,00 drug exposures. It occurs 2-6 weeks after the drug is first introduced, distinguishing it from other adverse drug-reactions which typically occur sooner.
The syndrome classically includes:
The most commonly implicated drugs are anticonvulsants (e.g., carbamazepine, phenobarbital, and phenytoin), sulfonamides, and allopurinol.
Recovery is typically complete after discontinuing the offending drug; systemic steroids may promote resolution of the illness.
31 year-old male with recently diagnosed hypertension presents with rapid lip swelling. He started taking an unknown medication for his hypertension last week. Further history reveals that he has had prior, although milder, episodes previously. Name two medications that may help treat him.

Metacarpal Neck Fractures (i.e.: Boxer’s Fracture if 5th Metacarpal)
Depending on the MCP joint involved a certain amount of angulation is permissible before it adversely affects normal function.
Wishing everybody a Happy and Healthy New Year.
Despite a paucity of data, pain management clinics are administering topical gel mixtures that have included ketamine, tricyclics, calcium channel blockers and baclofen. Internet blogs have already identified this gel mixture as a way to "get high". This is one of those google searches you have to do on your own.
Bottom Line: A mild increase in blood parasite count after initiation of treatment is not uncommon. Marked increases should indicated treatment failure and the treatment drug should be changed to another class.
University of Maryland Section for Global Emergency Health
Author: Emilie J.B. Calvello, MD, MPH
VV-ECMO for Refractory Hypoxemia
52 year-old male with diabetes complains of severe left foot pain for one month and now inability to ambulate. Vital signs are normal and X-rays are shown below. What's the diagnosis and why should you get a biopsy early?

NSAIDs are commonly used by professional and recreational athletes to both reduce existing and/or prevent anticipated exercise induced musculoskeletal pain
NSAIDs have potential hazardous effects on the gastrointestinal (GI) mucosa during strenuous physical exercise
Potential effects include mucosal ulceration, bleeding, perforation. and short-term loss of gut barrier function in otherwise healthy individuals
Intense exercise by itself has previously been shown to induce small intestine injury
Human intestinal fatty acid binding protein (1-FABP) is a protein found in mature small bowel enterocytes which diffuses into the circulation upon injury
Ibuprofen and endurance exercise (cycling) independently result in increased 1-FABP levels
When occurring together, ibuprofen ingestion with subsequent exercise causes significantly increased small bowel injury and intestinal permeability
Small bowel injury was found to be reversible in 2 hours
Taking empiric NSAIDs before endurance exercise may be an unhealthy practice and should be discouraged in the absence of a clear medical indication
Parents bring in their child who placed a bead, seed, or other object up her nose. What do you do? Who should you call?
Research suggests that a decades-old home remedy (of sorts) known as the “mother’s kiss” may do the trick for children 1-8 years of age. It’s also much less invasive or frightening than some of the tools and techniques used in emergency departments with a success rate approaching 60%
First described in 1965, here’s how the mother’s kiss technique works: