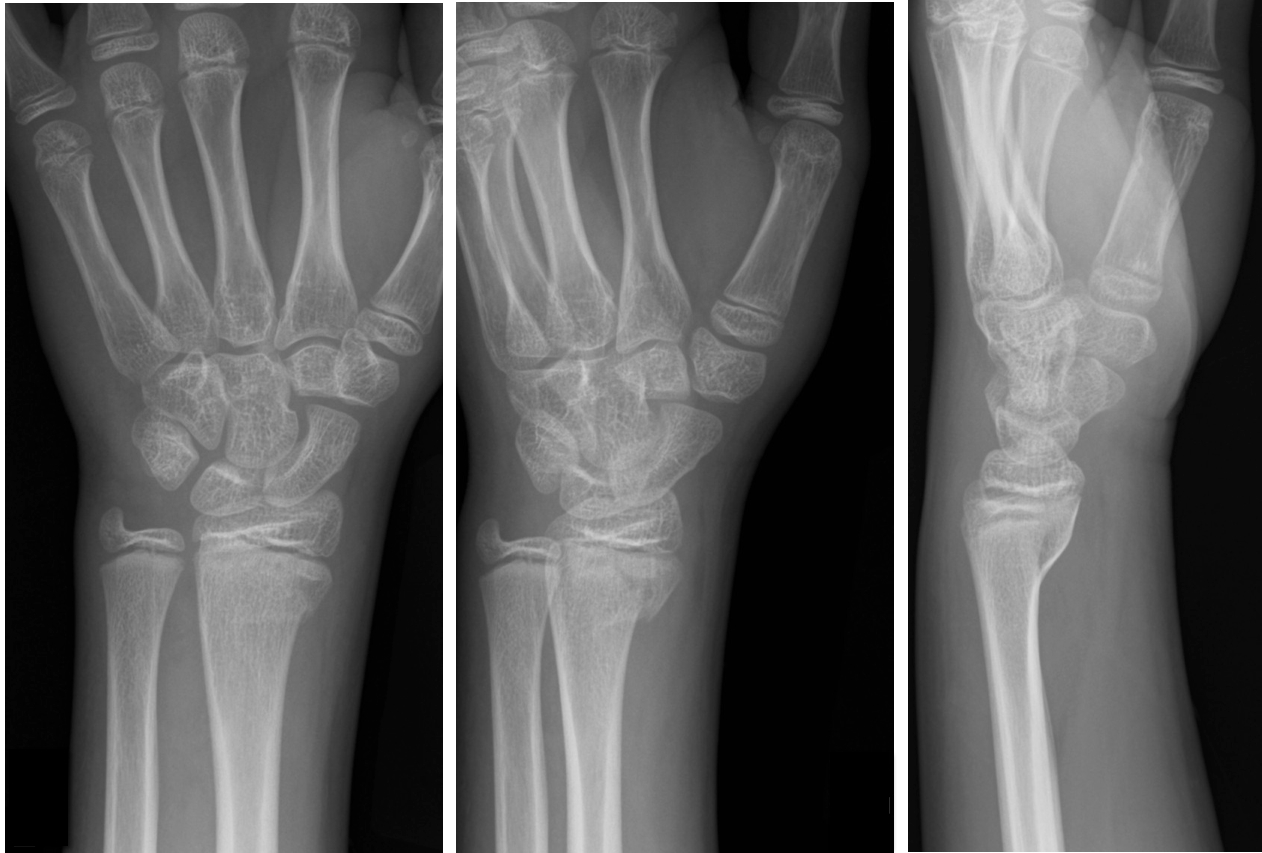
11 year-old male is tackled and falls on his outstretched hand while playing football. X-rays are shown below. What's the diagnosis?
An ECG pattern that signifies occlusion of the proximal left anterior descending coronary artery (LAD) without ST-segment elevation
It seems we've finally put to bed the myth that 10% of penicillin-allergic patients will also react to cephalosporins. Dr. Campagna, et al. recently published a review article concluding that the true cross-reactivity is negligible except when side-chains are similar [PMID 21742459].
This topic was also the subject of a recent post on the Academic Life in EM blog (http://academiclifeinem.blogspot.com/2012/08/busting-myth-10-cephalosporin.html).
But what about the reverse question? Can I give a penicillin to a cephalosporin-allergic patient?
Dr. Romano's group tested 98 patients with skin-test postitive cepahlosprin allergy (mostly IgE -mediated anaphylaxis). Patients were then skin tested for penicillin allergy. Those testing negative were challenged with a penicillin.
25% of patients reacted to the penicillin
Similar side-chain was a strong predictor of cross-reactivity
A Letter to the Editor response to this study pointed out that the authors used a smaller-than-standard size threshold for a positive response to the penicllin AND used a higher-than-standard dose of amoxicillin for testing. In light of this, the rate of subjects with cephalosporin allergy who do not have a history of penicillin allergy but with true IgE-mediated allergy to penicillin might be much closer to 5%.
Bottom line: The cross-reactivity of penicillins in cephalosporin-allergic patients is somewhere between 5-25%.
Conventional pediatric nasal cannula can safely deliver up to 4 lpm but are limited by cooling and drying of the airway. This leads to decreased airway patency, nasal mucosal injury, bleeding and possibly increase in coagulase negative staph infections.
HFNC delivers flow up to 40 lpm with 95-100% relative humidity at a controlled temperature. In infants, the initial flow rate is set between 2-4 lpm and can be increased to 8 lpm. Older children and can be started at 10 lpm and increased as high as 40 lpm. Oxygen is also adjustable.
Studies have shown improved comfort, respiratory rate and oxygenation compared to nasal CPAP.
Diagnosis should be considered in any individual over 5 years old with severe dehydration from diarrhea, regardless of exposure to an endemic area, and any patient over 2 years old with watery diarrhea in an endemic area.
Patients with severe cholera can stool as much as 1 L an hour. Replacing fluids is the most important part of treatment with oral rehydration being used as soon as possible. Oral rehydration therapy provides better potassium, carbohydrate, and bicarbonate replacement than most IV fluid solutions. Antibiotics will also decrease volume and duration of stooling but are only recommended in moderate to severe illness. Antiemetics are not useful because they can make patients sleepy and will reduce their ability to rehydrate orally. Antimotility medications will prolong the duration of illness.
University of Maryland Section for Global Emergency Health
Author: Jenny Reifel Saltzberg
Serotonin Toxicity in the Critically Ill
33 year-old male in respiratory distress. What's the diagnosis?

EPSS is an accurate and rapid bedside estimation of left ventricular function
First an image of heart should be obtained in the parasternal long-axis view
The ultrasound cursor should be placed through the anterior leaflet of the mitral valve
Subsequently, M-mode is applied and the distance between the anterior leaflet and the interventricular septum is measured during early diastole
A measurement of 7mm or greater indicates poor EF (see attachment below)
Distal radius fractures are common in children
Traditional management includes closed reduction +/- procedural sedation
The downside of this approach includes: patient risks, cost, physician time, ED bed time and tying up resources.
Kids have excellent bone remodeling potential...displaced and angulated fractures heal well without reduction
Crawford et al - 51 children aged 3 to 10 (avg 6.9 yrs) w/closed distal radius fractures.
Exclusions: open or growth plate fractures, metabolic bone disease or neurovascular injury.
No sedation, analgesia or fracture reduction was performed
Treatment: simple casting and gentle molding to correct angulation... i.e. fractures were left in a shortened, overriding position
Outcome: All patients had clinical and radiographic union and full range of motion of the wrist at one year w/ good patient (parent) satisfaction. This was associated w/ significant cost savings.
Consider this approach in consultation with orthopedist
Remember exclusions: open fractures, fracture dislocations, growth plate injuries and neurovascular injury.
Children w/ excessive angulation or rotational deformity should have standard care (closed reduction w/ sedation)
Multiple guidelines exist for "excessive angulation" but as a general rule
Age < 5 Up to 35 degrees
Age 5- 10 Up to 25 degrees
Age >10 Up to 20 degrees
As everyone knows by now the New England Compounding Company has been implicated in contaminated steroid vials that were used for epidural injections. Patients that have pleocytosis on CSF after lumber puncture will be admitted and started on liposomal amphotericin B and IV voriconozaole.
IV Voriconazole Adverse Effects:
Vivid visual hallucinations
Visual Disturbances - 30 min after administration: Blurry, photosensitivity
Hepatotoxitcity
Photoxicity - associated with increased risk of squamous cell CA of the skin
University of Maryland Section for Global Emergency Health
Author: Gentry Wilkerson
Trauma patient (...yes, that's the only history you're given). Diagnosis?
Cardiac amyloidosis can present along a spectrum from asymptomatic to severe CHF w/conduction abnormalities
ECG with low voltage + echocardiogram with thickened myocardium should heighten suspicion
Definitive Dx. is myocardial biopsy identifying the infiltrative lesion (MRI w/gad is also supportive)
AL (light chain) amyloidosis is an acquired disease from improperly functioning plasma cells
¨ Rapidly progressive and life threatening
¨ Tx. w/chemotherapeutic agents (+/- BMT)
Transthyretin-related (TTR) amyloidosis is produced by the liver (2 types)
Familial transthyretin-related amyloidosis (ATTR)
Senile systemic amyloidosis (SSA)
¨ Both are slowly progressive
¨ Tx liver transplant (ATTR) and supportive care (SSA)
Many who work in urban EDs and have a patient population that has a high rate of methadone use have probably wondered - why don't I see many STEMIs in the ED?
One study has actually attempted to answer the question - is methadone cardioprotective? Comparing 98 decedents with known long-term methadone exposure and compared autopsy coronary artery findings to match controls without, there was significant decrease in incidence of severe CAD:
5/98 Methadone Patients post-mortem had severe CAD vs 16/97 match controls
Better than a baby ASA, who knew?
[I thank Dr. Hoffman for citing this article to me]
Delirium in the Critically Ill
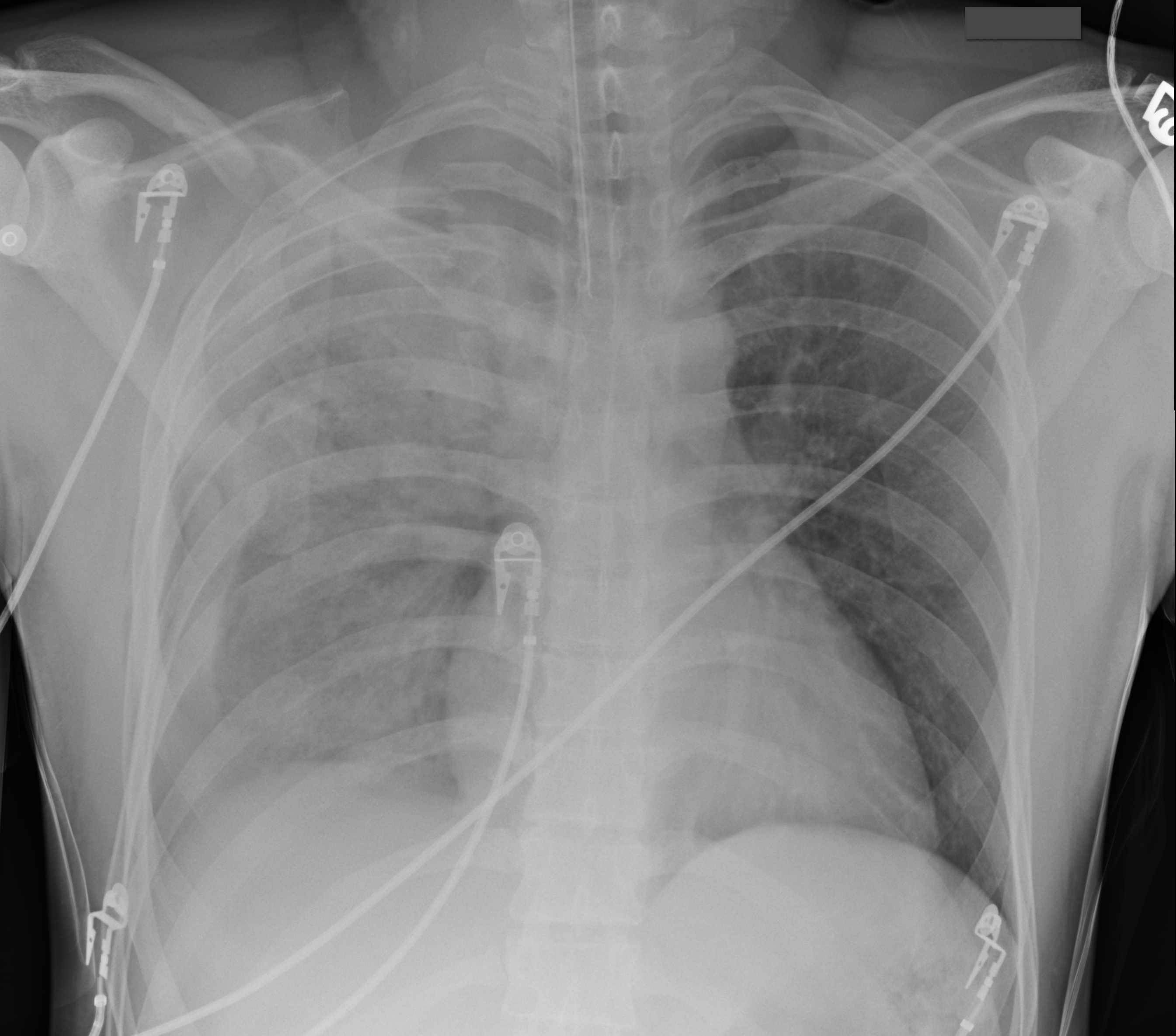
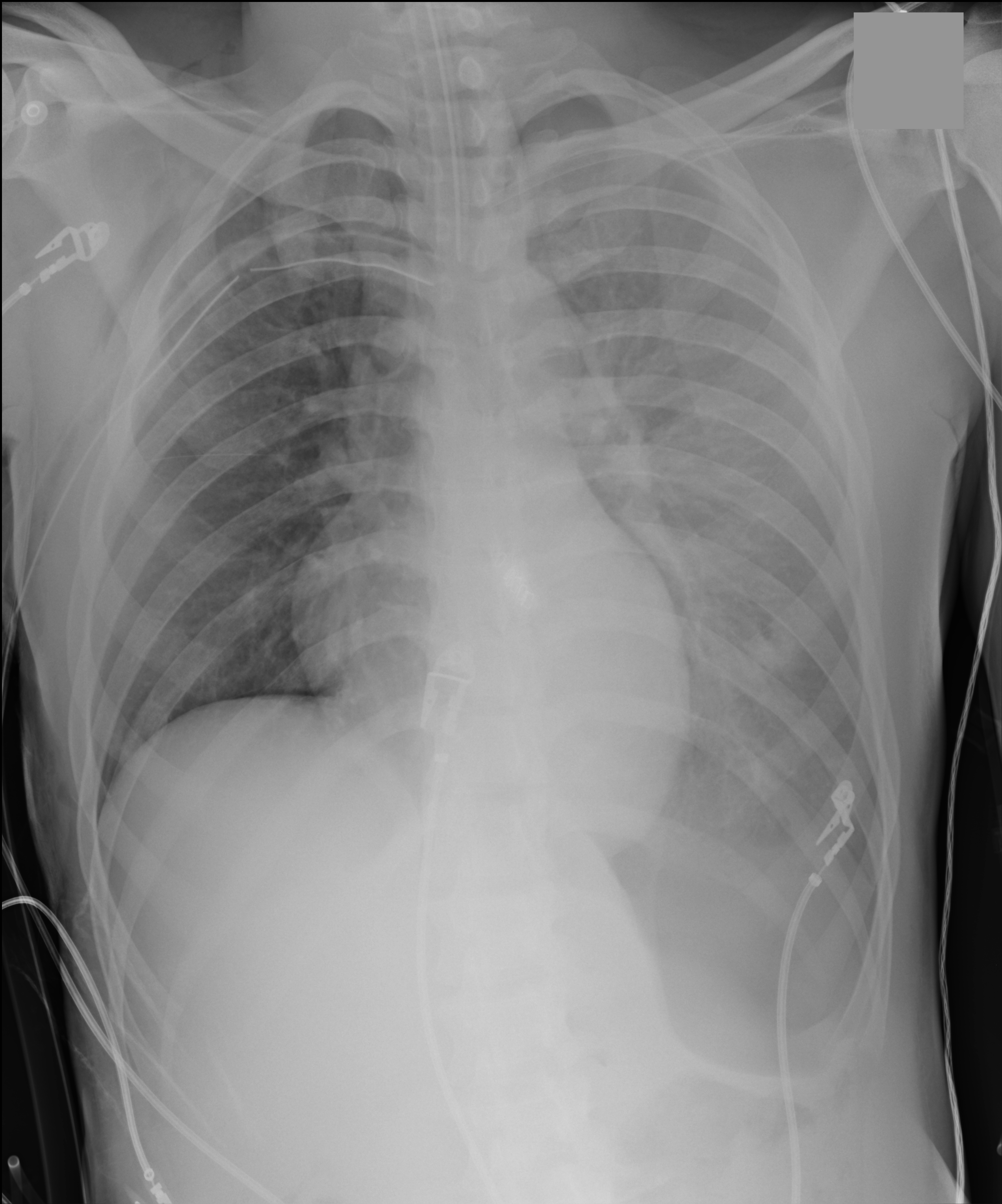
35 year-old male unrestrained driver following motor vehicle crash presents with blunt chest injury. There are multiple injuries on CXR (can you find them all?), but what's up with his right lung?