Etiological agent is the parasite Trypanosoma cruzi
Congratulations to today's Baltimore marathoners and the medical race staff
In honor of them:
Marathons are becoming increasingly popular with participation rising from an estimated 143,000 US marathon finishers in 1980 to a record high of 507,000 during 2010.
Most victims of exercise-related sudden cardiac arrest have NO premonitory symptoms
Autopsy reports show that
1) 65 - 70% of all adult sudden cardiac deaths are attributable to coronary artery disease.
2) 10% due to other structural heart diseases (HOCM, congenital artery abnormalities)
3) 5 - 10% due to primary cardiac conduction disorders (prolonged QT, ion channel disorders)
4) Remainder are due to non cardiac etiologies
Overall risk of sudden cardiac arrest is approximately from 1 in 57,000 and the risk of sudden cardiac death is approximately 1 in 171,000. Mortality without intervention after sudden cardiac arrest is greater than 95%. The majority occur in middle to late aged males.
V fib/V tach are the most common arrhythmias leading to sudden cardiac arrest. Most events occur in the last 4 miles of the racecourse.
Survival decreases by 7 - 10% with each minute of delayed defibrillation. Defibrillation within 3 minutes can produce survival rates as high as 67 - 74%. After 8 minutes, there is a dramatic decrease in survival. Prompt CPR increases survival from 2.5% to greater than 8%.
Activated charcoal is most effective if given within 1 hour of overdose.
Prehospital administration of charcoal can be challenging, but may save significant time compared to waiting until arrival to the ED. The patient has to be transported by EMS, registered, seen by a provider, order for charocal placed...
Two studies evaluated the time difference between prehospital and hospital administration of GI decontamination.
Bottom line: Don't underestimate the amount of time that goes by before you evaluate non-crashing patients upon arrival to the ED. If the story supports an overdose and the patient doesn't have contraindications for receiving charcoal, recommend it be given in the prehospital setting for greatest potential benefit.
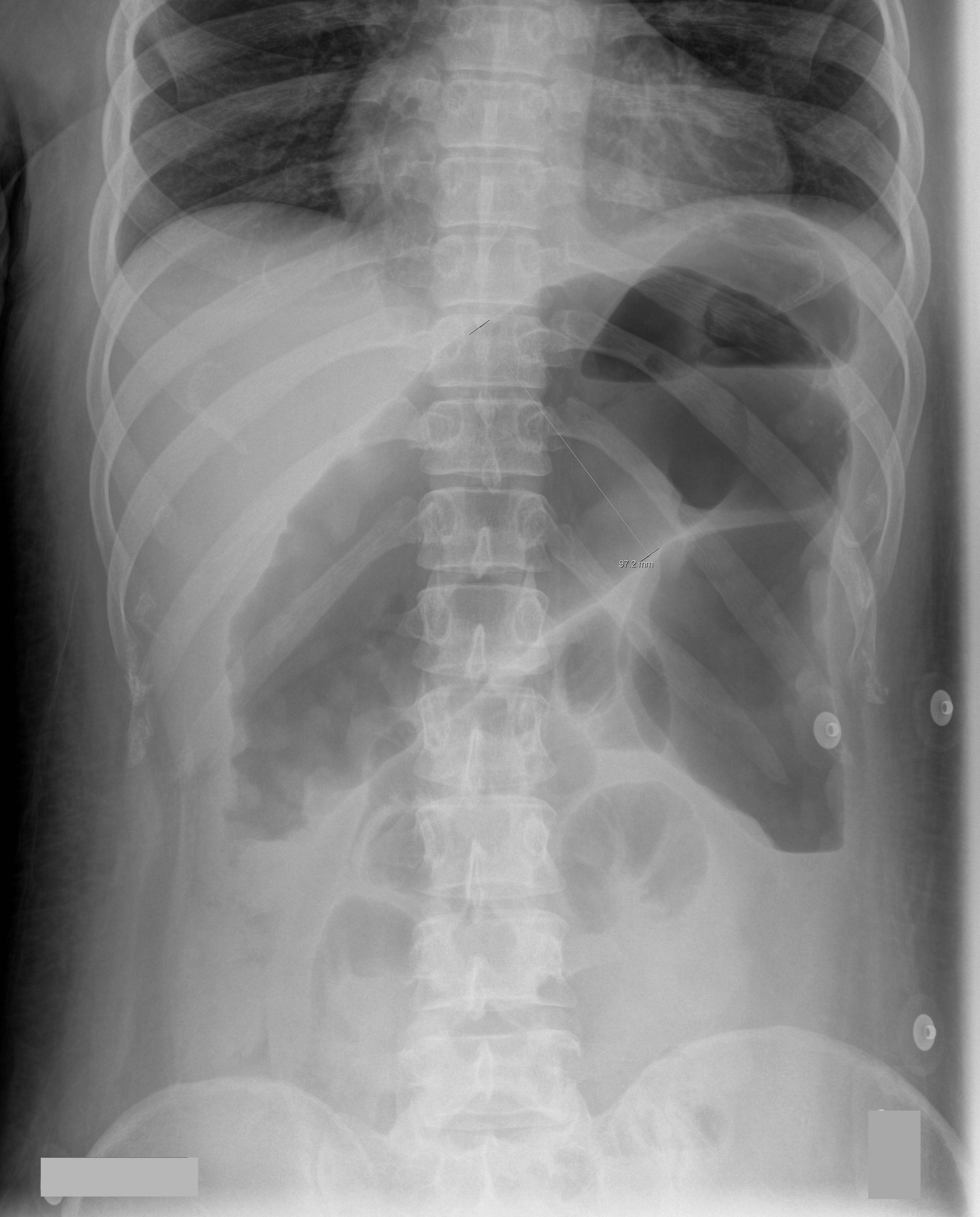
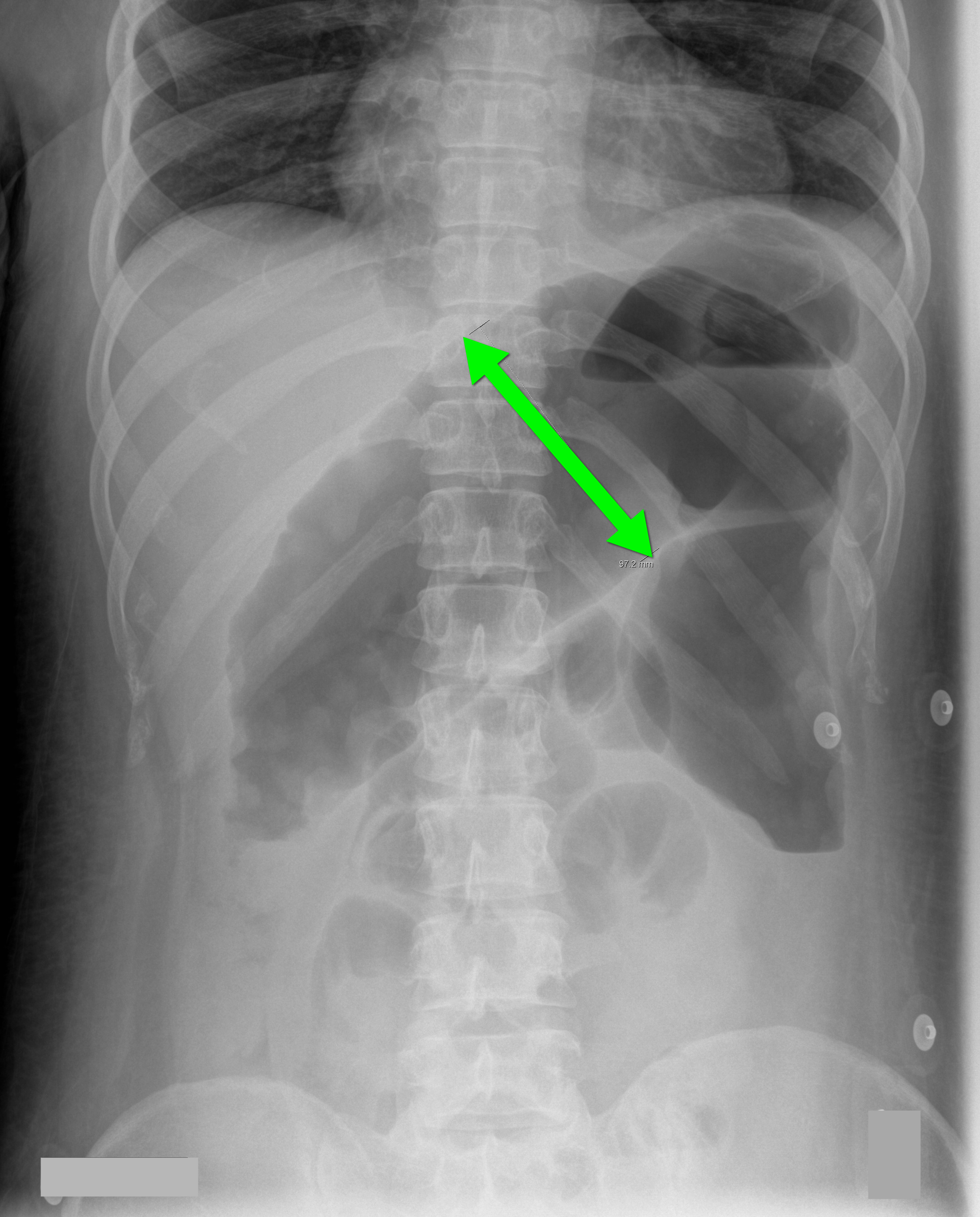
70 year-old male recently treated for community-acquired pneumonia presents with bloody diarrhea, fever, and severe abdominal pain. Abdominal Xray is shown below. Diagnosis?
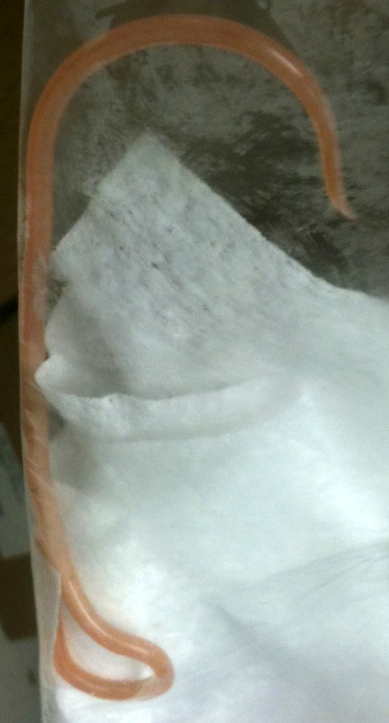
26 year-old male from Indonesia presents with severe abdominal pain and weight loss for the past two months. He also states he found this "worm" in the toilet (see below) after a bowel movement. What is the medical treatment for this condition?
Autoantibody-associated congenital heart block (CHB), also know as neonatal lupus, is responsible for the majority (~60-90%) of CHB
This is secondary to maternal antibodies that cross the placenta and may disappear postnatal
Neonatal lupus can result in diffuse myocardial disease both with and without conduction disturbances, structural defects, and electrophysiologic anomalies
Overall mortality is up to 30%, with 15% mortality before 3 months of age
More than 65% of surviving newborns require pacemakers
Maternal screening and fetal echocardiography has allowed routine prenatal diagnosis
Patients frequently report having a sulfa allergy. In most cases, the allergic reaction was secondary to a sulfonamide antimicrobial agent, such as sulfamethoxazole-trimethoprim.
The question is: Can I use furosemide (or other non-antimicrobial agents containing a sulfa component)?
There is minimal evidence of cross-reactivity between sulfonamide antimicrobials and non-antimicrobials.
Despite this, the U.S. FDA-approved product information for many non-antimicrobial sulfonamide drugs contains warnings concerning possible cross-reactions.
Bottom line: If a patient had a true IgE-mediated anaphylatic reaction to a sulfonamide antimicrobial, it may be best to avoid other sulfa-related medications (use ethacrynic acid if a loop diuretic is needed). Otherwise, the available literature does not support cross-reactivity between sulfonamide antimicrobials and non-antimicrobials.
We often ask our pediatric patients if there vaccines are up to date, but what does this mean?
Hepatitis B: birth, 2 and 6 months
Diphtheria/Tetanus and Acellular Pertussis: 2, 4 and 6 months
Pneumococcal vaccine: 2, 4 and 6 months
Haemophilus influenzae B : 2, 4 and 6 months
Polio: 2, 4 and 6 months
Rotavirus: 2 and 4 months or 2, 4 and 6 months depending on the brand.
Influenza: 6 months and older
Children less than 8 years old should receive 2 doses of flu vaccine at least 4 weeks apart during the first flu season that they are immunized. Children older than 2 years are eligible for the nasal vaccine if they do not have asthma, wheezing in the past 12 months or other medical conditions that predispose them to flu complications.
To see the full vaccine schedule including exact time frames between doses and catch up schedules, see: http://www.cdc.gov/vaccines/
Ever have that alcholic who requires lorazapam doses that start to approach 10mg? 20mg? or even higher. The next step is usually a lorazepam infusion and then send them to the ICU. In the ICU, the patient develops an unexplained anion gap lactic acidosis.
Check a Lactate - lorazepam has 80% propylene glycol (PG). PG is metabolized to lactate which can accumulate when a lorazepam infusion at an elevated dose is running constantly. Hypotension, bradycardia and even other EKG changes have been reported. Simply discontinue the infusion and assess your acid-base status.
Other IV meds that contain PG:
lorazepam - 80% PG
Phenytoin - 40% PG
Phenobarbital - 67.8%
Diazepam - 40% PG
Thrombotic Thrombocytopenic Purpura (TTP)
Do you place central-lines?
Do you suture your central-lines into place?
Do you ever get worried that you are going to stick yourself with that needle?
If you answered yes to any of these questions, then maybe this pearl is for you; click here
Aortic valve (AV) stenosis associated with gastrointestinal angiodysplasia
Proteolysis of Von Willebrand (type 2A) as it passes through the stenotic valve is one culprit of bleeding
Hemostatic abnormalities e.g. GI bleed are often corrected after AV replacement
Valve replacement is only recommended for cardiac symptoms
Fight Bites
The incidence of pediatric syncope is common with 15%-25% of children and adolescents experiencing at least one episode of syncope before adulthood. Incidence peaks between the ages of 15 and 19 years for both sexes.
Although most causes of pediatric syncope are benign, an appropriate evaluation must be performed to exclude rare life-threatening disorders. In contrast to adults, vasodepressor syncope (also known as vasovagal) is the most frequent cause of pediatric syncope (61%–80%). Cardiac disorders only represent 2% to 6% of pediatric cases but account for 85% of sudden death in children and adolescent athletes. 17% of young athletes with sudden death have a history of syncope.
Key features on history and physical examination for identifying high-risk patients include exercise-related symptoms, a family history of sudden death, a history of cardiac disease, an abnormal cardiac examination, or an abnormal ECG.
Intubated patients may occasionally meet certain criteria for extubation while in the Emergency Department. Extubation is not without its risk, however, as up to 30% of patients have respiratory distress secondary to laryngeal and upper airway edema, with some patients requiring re-intubation.
Prior to extubation, Intensivists use a brief “cuff-leak” test (deflation of the endotracheal balloon to assess the presence or absence of an air-leak around the tube) to indirectly screen for the presence of upper airway edema and ultimately the risk of re-intubation. The cuff-leak test is performed by deflating the endotracheal balloon followed by one or more of the following maneuvers:
Ochoa et al. performed a systematic review to determine the accuracy of the “cuff-leak” test to predict upper airway edema prior to extubation. The authors concluded that a positive cuff-leak test (i.e., absence of an air-leak) indicates an elevated risk of upper airway obstruction and re-intubation. A negative cuff-leak test (i.e., presence of an air-leak), however, does not reliably exclude the presence of upper airway edema or the need for subsequent re-intubation.
Bottom line: No test prior to extubation reliably predicts the absence of upper airway edema. Patients extubated in the Emergency Department require close observation with airway equipment located nearby.
Guide-wires can be challenging to dispose of after central-line insertion because they are difficult to keep on the field, hard to place in the sharps box, and can splash nearby observers.
Click here for this little guide-wire disposal trick.
SLAP tear/lesion – Superior labral tear anterior to posterior
Glenoid labrum – A rim of fibrocartilaginous tissue surrounding the glenoid rim, deepening the “socket” joint and is integral to shoulder stability
http://www.orthospecmd.com/images/shoulder_labral_tear_anat_02.jpg
Injury is most commonly seen in overhead throwing athletes
Or from a fall on the outstretched hand, a direct shoulder blow or a sudden pull to the shoulder
Sx’s: A dull throbbing pain, a “catching” feeling w/ activity. Some describe clicking or locking of the shoulder. May also include nighttime symptoms. Pain is located to the anterior, superior portion of the shoulder.
Athletes may describe a significant decrease in throwing velocity
http://sitemaker.umich.edu/fm_musculoskeletal_shoulder/o_brien_s_test
{kind=link}