Metoprolol Usage Cardioprotective
JNC8 (the Eigth Joint National Commission) released their recommendations for blood pressure management this week. The full article as published in JAMA can be found at http://jama.jamanetwork.com/article.aspx?articleid=1791497
Highlights from this report are
General Pearl: Remember to be cautious in acutely lowering the blood pressure in asymptomatic patients. Acute lowerings can cause watershed ischemia leading to strokes.
A new drug is coming onto the drug scene with some case reports beginning to build. The internet appears to have been a major driver or mode of distribution for this particular drug.
One study of users showed that this ketamine analog has more vivid hallucinations that would liken it to LSD. It has been theorized that this drug has the dissociative effects of ketamine but also has prominent serotninergic effects making additions more likely and hallucinations possible.
If you see a case in your ED, you can say you heard it here first!
In November 2013, the CDC issued multiple Alerts on various polio outbreaks in Asia and Africa. Countries currently with the heaviest burden are Syria, Pakistan, Somalia, Kenya, and Cameroon. Nigeria and Afghanistan have also had persistent epidemics.
General Information:
Relevance to the EM Physician:
The diagnosis can be made by detecting:
The CSF analysis results will resemble that of aseptic meningitis.
Bottom Line:
Have a high suspicion for travellers to affected regions and recognize the high prevalence of asymptomatic infection (and thus importable epidemic potential). Pre-travel vaccination is essential.
University of Maryland Section of Global Emergency Health
Author: Walid Hammad, MB ChB
Hepatic Encephalopathy (HE)
Pathogenesis: Several theories exist that include accumulation of ammonia from the gut because of impaired hepatic clearance that can lead to accumulation of glutamine in brain astrocytes leading to swelling in patients with hepatic insufficiency from acute liver failure or cirrhosis.
Clinical Features:
Diagnostic tests: Ammonia levels are routinely drawn but must be drawn correctly without the use of a tourniquet, transported on ice, and analyzed within 20 minutes to get an accurate result. Severity of HE does not correlate with increasing levels.
Management:
1. Airway protection as needed
2. Correct precipitating factors (GI bleed, infection-SBP, hypovolemia, renal failure)
3. Consider neuro-imaging if new focal neurologic findings are found on exam
4. Correct electrolyte imbalances
5. Lactulose by mouth (PO/Naso-gastric tube or Rectally)
a. 10-30 g every 1-2 hours until bowel movement or lactulose enema (300 mL in 1 L water)
b. Facilitates conversion of NH3 to NH4+, decreases survival of urease-producing bacteria in the gut
6. Rifaximin 550 mg by mouth BID (minimally absorbed antibiotic with broad-spectrum activity)
7. Do not limit protein intake acutely
8. TIPS reduction in certain patients with recurrent HE
9. Transplant referral as needed
10. Consider other causes if patient does not improve within 24-48hrs.
46 year-old female found unresponsive at a party. EMS transports the patient in cardiac arrest. A parasternal-long axis view of the heart is obtained during the pulse check. What's the diagnosis?
Treating knee osteoarthritis - from the American College of Rheumatology
Exercise whether it be aquatic, aerobic (land -based) or resistance can decrease pain and improve functional capacity. Exercise should be performed 3 to 5 times a week. Effects are usually noted after 3 to 6 months.
Weight loss of 5% or greater body weight is associated with a small improvement in pain and physical function. The main benefit of weight loss has more to do to effects on co-morbid conditions.
Walking aids: A single crutch or cane should be held on the side contralateral to the affected knee and should be advanced with the affected limb when walking to reduce the load on the affected joint.
Cane sizing: The distance from the floor to the patient's greater trochanter (brings the elbow to 15º to 20º of flexion.
Can acetaminophen concentrations < 100 mcg/mL obtained between 1-4 hours after acute ingestion accurately predict a nontoxic 4-hour concentration? NO!
Despite a high negative predictive value, a new study found there are still cases with toxic concentrations after 4 hours despite earlier levels < 100 mcg/mL.
The Rumack-Matthew nomogram is to be utilized starting at 4 hours after an acute acetaminophen ingestion. Unless the concentration is zero, a second level must be drawn at 4 hours if an earlier one is positive.
Clinical Presentation:
Diagnosis
Treatment
Bottom line:
Chikungunya virus can cause symptoms similar to dengue fever but is not as deadly. This week the first cases of CHIKV were reported in the Caribbean. Consider this in travelers returning from endemic areas.
Distinguishing features:
University of Maryland Section for Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
The Concentrated Overview of Resuscitative Efforts (CORE) Scan
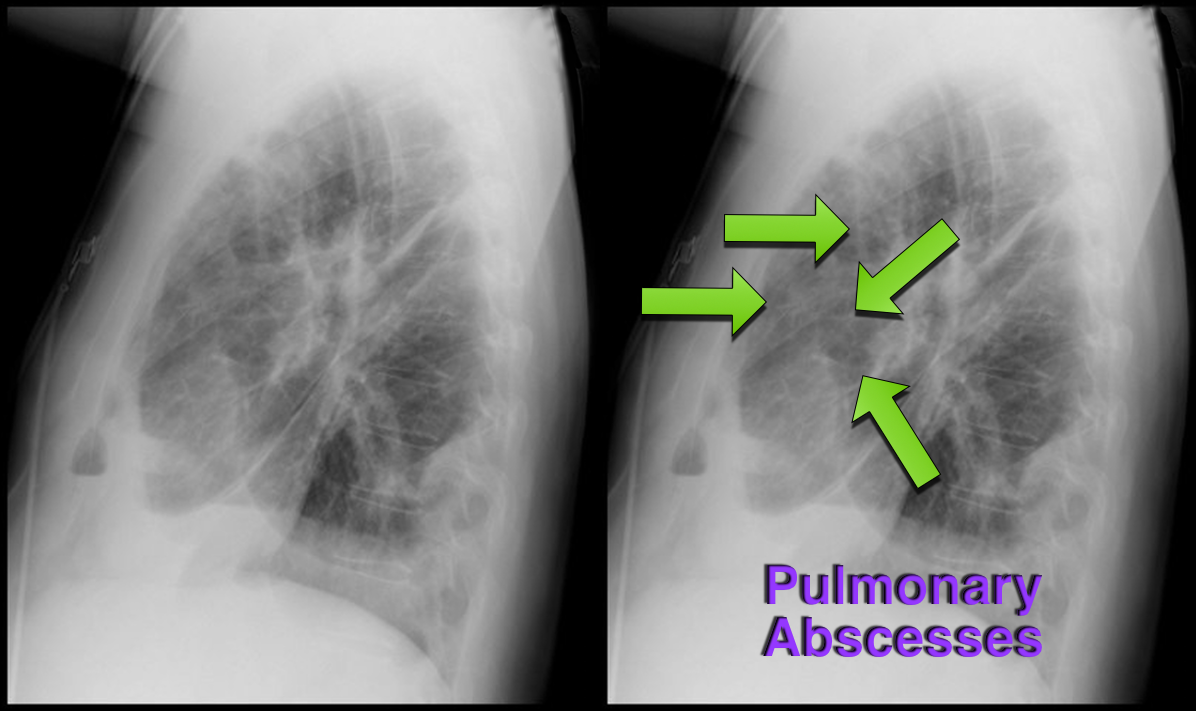
37 year-old male presents with cough and a fever. What's the diagnosis and name three risk factors assiciated with disease?

Bottom-line: The HEART score can help to objectively risk stratify ED patients with chest pain into low, intermediate, and high risk groups. Using the HEART score can also facilitate more efficient and effective communication with colleagues.
Want more emergency cardiology pearls? Follow me @alifarzadmd
In a potentially ground breaking study of healthcare-associated pneumonia (HCAP) patients, atypical pathogens were identified in 10% of cases!
Application to clinical practice: Add atypical coverage with a macrolide or respiratory fluoroquinolone for HCAP patients who have been in the community for any length of time.
The study also identified HCAP patients who may not require 3 'big gun' broad-spectrum antibiotics. This is a practice changing article for ED providers. For more analysis of the study, please note the bonus reading links below.
Bonus reading:
Dr. Emily Heil (@emilylheil) analyzes the full study in more depth at Academic Life in Emergency Medicine: http://academiclifeinem.com/new-treatment-strategy-not-so-sick-health-care-associated-pneumonia/
Dr. Ryan Radecki (@emlitofnote) critiques the study at Emergency Medicine Literature of Note: http://www.emlitofnote.com/2013/10/down-titrating-antibiotics-for-hcap.html
It has linear, predictable pharmacokinetics, achieves maximal concentration within 1-2 hours, is 50% renally excreted, and has a half life is 9-11 hours.
Edoxaban was evaluated in a recent trial comparing warfarin in patients with atrial fibrillation.
The primary end point or first stroke or systemic pulmonary embolic event occurred in 1.5% with warfarin, compared with 1.18% in the high dose edoxaban (HR 0.79; 97.5% CI 0.63-0.99, P<0.001). In the intention to treat there were trends favoring high dose edoxaban and unfavorable trends with the lower dose.
The principal safety end point of major bleeding occurred in 3.43% with warfarin versus 2.75% with high dose edoxaban (HR 0.86; 95% CI 0.71-0.91, P<0.001).
Bottom line: Both high dose (60 mg) and low dose (30 mg) edoxaban were non-inferior to warfarin with prevention of stroke or systemic emboli, and were associated with significantly lower rates of bleeding and death from cardiovascular causes.
Currently it is approved for use in Japan.
General Information:
Fever and headache or rash in those with close contacts from the affected universities should be considered for rapid, empiric meningococcal treatment.
Vent Management: Finding the AutoPEEP!
OK, so we all know not to, "...Fall asleep on Auto-PEEP" thanks to Dr. Mallemat's pearl that can be seen here. But now the question is, how do you know if your patient is air-trapping?
There are 3 ways you can look for evidence of Auto-PEEP on the ventilator:
Which view of the heart is this and can you name the structures from A-G?
ECG Following Cardiac Transplant