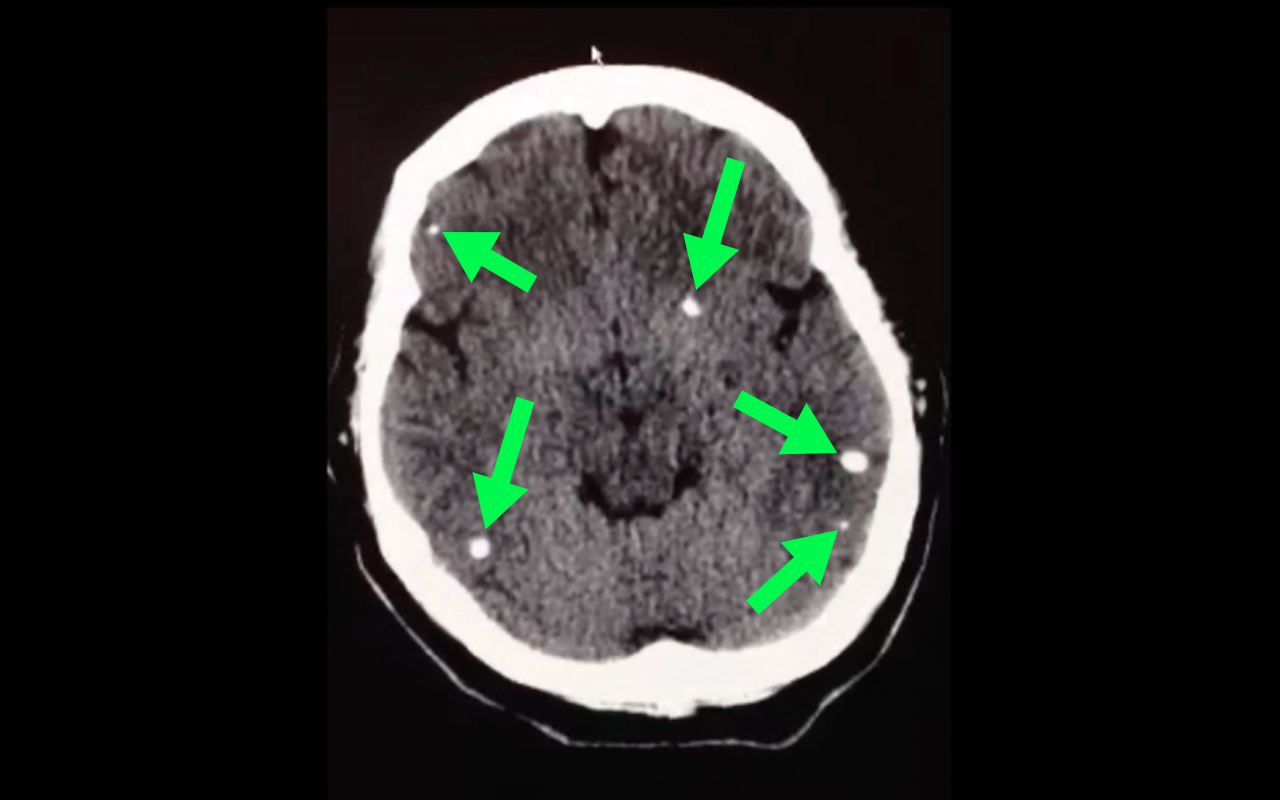
50 year-old with facial weakness and dysarthria. What's the diagnosis?
The clinical examination is often unreliable in ruling out septic arthritis in the ED.
Diagnostic arthrocentesis is often performed.
Traditional teaching involved very high WBC count thresholds as part of diagnosis.
In one 2009 study, synovial leukocyte counts in cases of MRSA were often less than 25,000 cells/uL
Have a low threshold for empiric antibioitics even in the face of low WBC counts (and incredulous consultants)
Passive leg raise (PLR) has been studied in adults as a bedside tool to predict volume responsiveness (see previous pearls from 5/7/13 and 6/17/2008). Can this be applied to children?
A single center prospective study looked at 40 intensive care patients ranging in age from 1 month to 12.5 years. They used a noninvasive monitoring system that could measure heart rate, stroke volume and cardiac output. These parameters were measured at a baseline, after PLR, after another baseline and after a 10 ml/kg bolus.
Overall, changes in the cardiac index varied with PLR. However, there was a statistically significant correlation in children over 5 years showing an increase in cardiac index with PLR and with a fluid bolus.
Bottom line: In children older then 5 years, PLR can be a quick bedside tool to assess for fluid responsiveness, especially if worried about fluid overload and in an under served area.
General Information:
Bottom Line:
Tenofovir has already become standard therapy for HIV (contained in Truvada and Atripla). This HBV study shows promise that this drug can not only decrease progression of disease but also reverse the cirrhosis associated with long-term infection. Given the prevalence of chronic HBV, larger scale role-out of this drug could markedly change the epidemiologic landscape of morbidity and mortality due to hepatitis B.
University of Maryland Section of Global Emergency Health
Author: Emilie J.B. Calvello
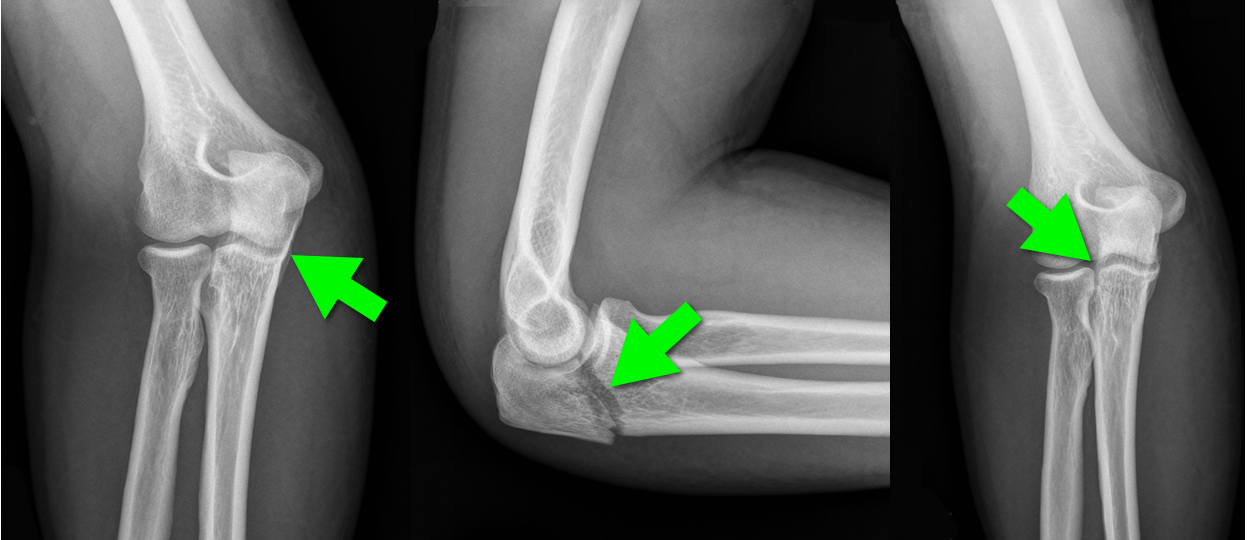
44 year-old construction worker fell off a ladder and presents with elbow pain. What's the diagnosis and what is the most commonly associated nerve injury?

Early Atherosclerosis Detection
50 middle-aged asymptomatic subjects free of vascular disease underwent carotid ultrasound (CUS) for risk stratification were also invited to undergo coronary computed tomography angiography (CCTA) or coronary artery calcium score (CAC) to identify which of the 3 imaging modalities was best at identification of early atherosclerosis
Atherosclerosis was observed in 28%, 78%, and 90% of subjects using CAC, CCTA, and CUS, respectively
36 patients with a CAC score = 0, 69% and 86% had atherosclerosis on CCTA and CUS, respectively
Concordance between modalities was highly variable
CUS and CCTA detection of plaque were significantly more sensitive than CAC
Considering the prevalence of subclinical disease on CUS and CCTA, the threshold at which to treat warrants further research
Inborn errors of metabolism (IEM) are rare, each typically affecting 1 in 5000 to 1 in 100,000 children, BUT collectively these disorders are more common because there are so many. If you are lucky…when they present to the ED they come with a letter from Dr. Greene (our world renowned metabolic geneticist) detailing exactly what to do. The rest of the time…you are on your own. Think about IEM in any neonate or child with history of feeding difficulties, failure to thrive, recurrent vomiting, unexplained altered mental status and/or acidosis. Pay particular attention to feeding difficulties that appear with changes in diet: switch from soy to cow’s milk formula (galactose), addition of juice or fruit or certain soy formulas (fructose), switch from breast milk to formula or foods (increased protein load), and longer fasting periods from sleeping or illness.
For this pearl, we will focus on primary hyperammonemia from an enzymatic block in ammonia metabolism within the urea cycle. It is important to remember that secondary hyperammonemia can result from metabolic defects such as organic acid disorders, fatty acid oxidation disorders, drugs that interfere with urea cycle, or severe liver disease. Amino acids liberated from excess protein breakdown (stress of newborn period, infection, injury, dehydration, surgery, or increased intake) release nitrogen which circulates as ammonia. Ammonia is then converted to urea via the urea cycle and excreted in the urine. With urea cycle defects (UCD) there is an enzymatic block in the cycle that results in accumulation of ammonia which has toxic effects on the CNS especially cerebral edema. The most common UCD is ornithine transcarbamylase deficiency followed by argininosuccinic academia, and citrullinemia.
Clinical presentation includes poor feeding, lethargy, tachypnea, hypothermia, irritability, vomiting, ataxia, seizures, hepatomegaly, and coma. Hyperammonemic crises in neonates mimic sepsis! If you think about an IEM in your differential, send plasma ammonia (1.5 mL sodium-heparin tube on ice STAT), plasma amino acids, and urine organic acids. Other helpful labs include blood gas, CMP, urinalysis (looking at ketones), lactate, plasma acylcarnitines, and newborn screen if not already sent. Plasma ammonia is a direct index of CNS toxicity and important to follow for acute management. Serum level > 150 in sick neonate or > 100 in sick infant/child is concerning for IEM. The presence of hyperammonemia and respiratory alkalosis suggest urea cycle defect. The presence of metabolic acidosis and hyperammonemia suggests organic acid disorder.
Immediate treatment of hyperammonemia is critical to prevent neurologic damage. Cognitive outcome is inversely related to the number of days of neonatal coma caused by the cerebral edema.
1. Stop all protein intake! You need to stop catabolism.
2. Start D10 at 1.5 times maintenance rate with GIR at least 6-8. Start intralipids 1-3g/kg/day when able (typically in the ICU after central line placed).
3. Give ammonia scavenger medications sodium benzoate and sodium phenylacetate. These are available commercially as Ammonul.
a. 0-20kg: 2.5mL/kg IV bolus over 90 min followed by same dose as 24 hr infusion
b. >20kg: 55 mL/m2 IV bolus over 90 min followed by same dose as 24 hr infusion
4. HEMODIALYSIS! Dialysis is the most effective way to remove ammonia and should be done when level > 300. The decision to hemodialyze is crucial in preventing irreversible CNS damage; when in doubt in the face of elevated ammonia, HEMODIALYZE!
Seizures can be the presenting manifestation of acute poisoning in children.
A 3-year data set from the Toxicology Investigators Consortium (ToxIC) Case Registry identified 142 cases of drug-induced seizures in children < 18 years old. 75% were teenagers.
Antidepressants were most commonly associated with causing seizures, especially bupropion and citalopram. Diphenhydramine was also a commonly identified cause.
The authors conclude that clinicians managing teenagers presenting with seizures should have a high index of suspicion for intentional ingestion of antidepressants.
Bottom line
ED crowding remains a critical problem in the US and globally. It is frequently driven by the “boarding” of admitted patients. Improved patient flow is needed to be able to take care of patients presenting with acute care needs.
University of Maryland Section of Global Emergency Health
Author: Jon Mark Hirshon, MD, MPH, PhD
A 50yo man found dow in the snow was brought into our ER last week in cardiac arrest with a bladder temperature of 21° C. Let’s warm him up!
We were able to get ROSC with CPR and ACLS and then used Artic Sun to re-warm successfully.
Other tips/tricks:
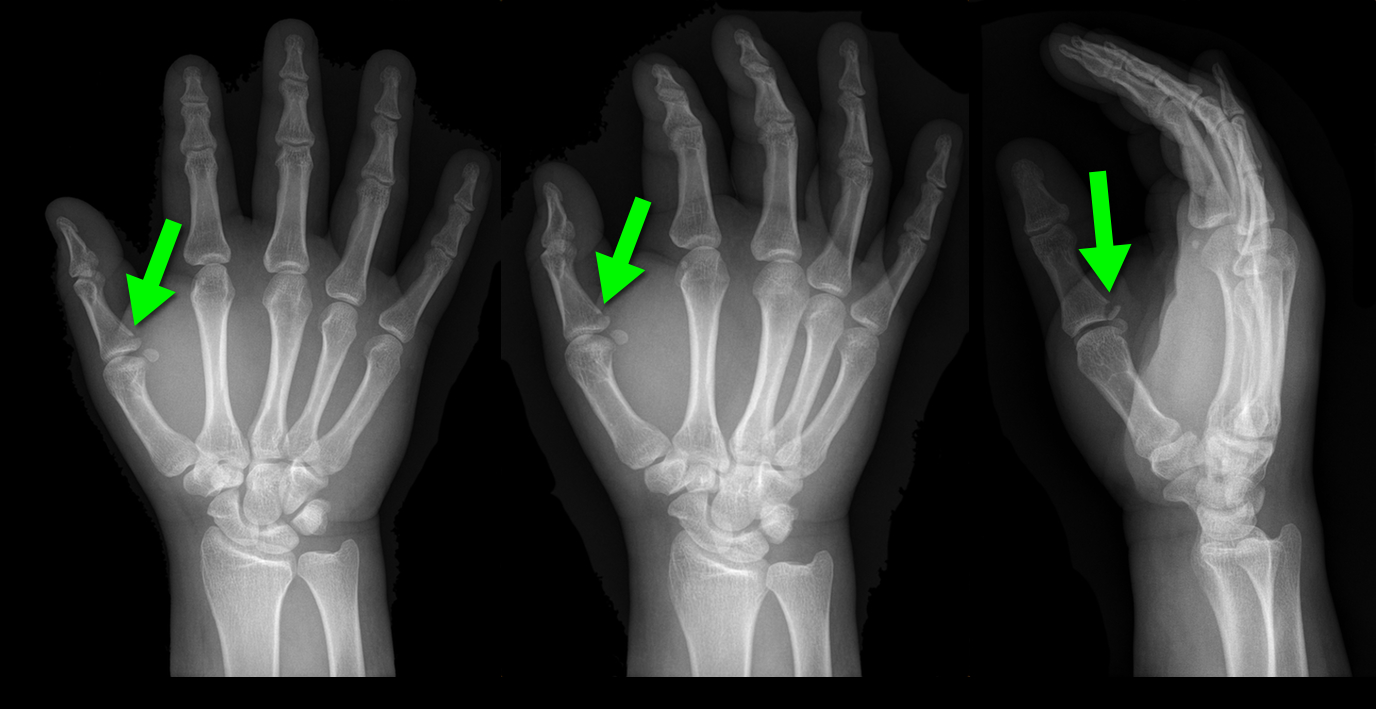
25 year-old male presents after falling off his bicycle. He complains of pain in his right-hand (he is right-hand dominant). What's the diagnosis?

The importance of new ST-segment depressions (STD) and/or T wave inversions (TWI) in lead aVL have not been emphasized or well recognized across specialties. Computer-assisted ECG readings typically report these findings as normal or nonspecific.
There is growing evidence that changes in lead aVL are abnormal, and that paying attention to that lead can be clinically useful. Reciprocal changes presenting as STD or TWI in lead aVL may be indicative of a significant coronary artery lesion and can sometimes be the only ECG manifestation of acute MI.
STD in lead aVL is considered a sensitive marker for early inferior STEMI, and has been shown to help differentiate STEMI from pericarditis. Another recent retrospective study suggests that TWI in aVL might be associated with significant LAD lesions.
Bottom Line: Paying close attention to subtle changes and abnormalities in lead aVL may help in early identification and initiation of therapy for patients who are having an acute MI.
Overtraining syndrome
A maladaptive response to excessive exercise without adequate functional rest
-Results in disturbances of multiple body systems (neurologic, endocrinologic, immunologic and psychologic).
- May be caused by systemic inflammation and resultant neurohormonal changes
- Multiple hypotheses exist
-Symptoms
Parasympathetic alterations: fatigue, depression, bradycardia
Sympathetic alterations: insomnia, irritability, agitation, tachycardia, hypertension, restlessness
Other: anorexia, weight loss, poor concentration, anxiety
Usual presentation is prolonged underperformance despite adequate rest and recovery (weeks to months).
Ondansetron (Zofran) is a great anti-emetic that, since it has gone generic, is also inexpensive. High dose ondansetron has been reported to cause QT prolongation and that practice is largerly discontinued now in the oncology world. Another uncommon adverse drug reaction may be dystonia. Though we think of ondansetron as a 5-HT3 blocker and should not cause the dystonic reaction like we see in metoclopramide, there are case reports of this reaction occurring.
Tranexamic Acid (TXA) topically applied was compared to anterior nasal packing in 216 patients with acute anterior epistaxis. Cotton pledgets (15 cm) soaked in injectable TXA (500 mg/5 ml) were inserted into the bleeding nostril and removed after bleeding had arrested. This was compared to standard anterior packing.
RESULTS
| TXA Anterior packing |
| % pts bleeding stopped in 10 min: 71% 31.2% |
| Discharge after 2 hours 95.3% 6.4% |
| Rebleeding in 24 h hours 4.7% 11% |
| Satisfaction scores 8.5 4.4 |
Bottom line: topical tranexamic acid looks promising for control of uncomplicated anterior epistaxis.
General Information:
Area of the world affected:
Relevance to the US physician:
Bottom Line:
VRU traffic injuries are the greatest challenge of today's worldwide road safety.
University of Maryland Section of Global Emergency Health
Author: Terrence Mulligan DO, MPH
Mechanical Ventilation During ECMO