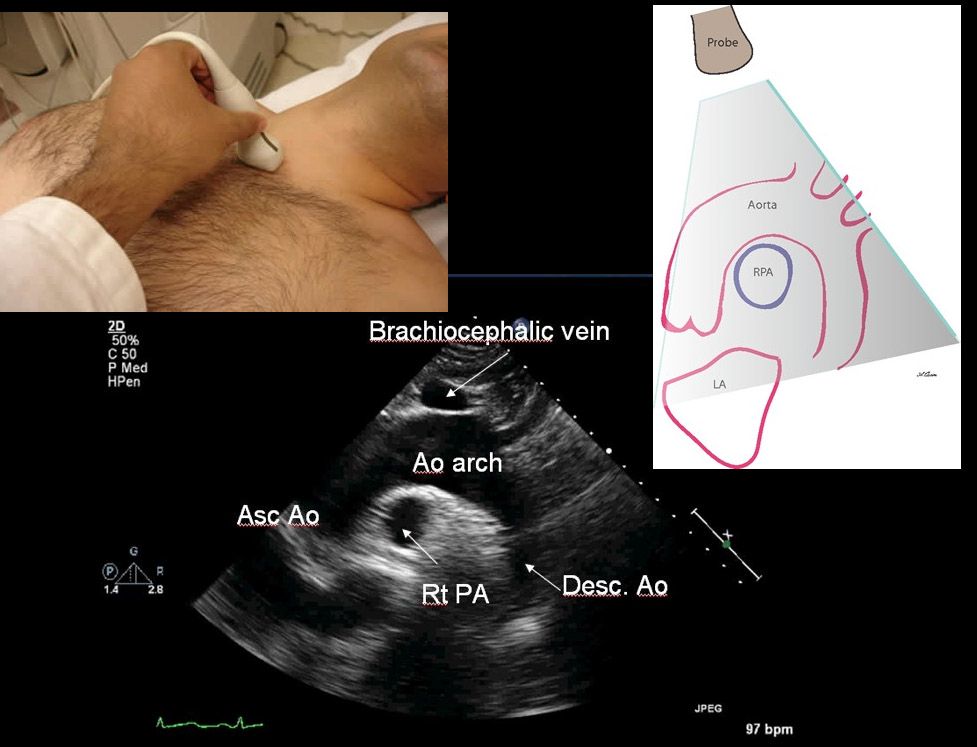
35yo M with history of rheumatic heart disease presents with fever. What disease process is suggested by the echo?
.JPG)
In 2001, Rivers et al. published a landmark article demonstrating an early-goal directed protocol of resuscitation that reduced mortality in septic Emergency Department patients.
Many questions have arisen throughout the years with respect to that trial; critics have complained about the overwhelming change in clinical practice based on this one single-center randomized trial.
Challenging Rivers data are the ProCESS (Protocolized Care for Early Septic Shock) investigators, who released the results from a multi-center randomized control trial of 1351 septic Emergency Department patients; the primary end-point was 60-day mortality. Click here for NEJM article.
Patients in this trial were randomized to one of three groups:
Protocol-based EGDT
Protocol-based standard (did not require central lines, inotropes, or blood transfusions
Usual care (no specific protocol; care was left to the bedside clinicians)
Bottom-line: The investigators did not find any difference in mortality between patients in the three groups and comment that the most important aspects of managing the septic patient may be prompt recognition and early treatment with IV fluids and antibiotics.
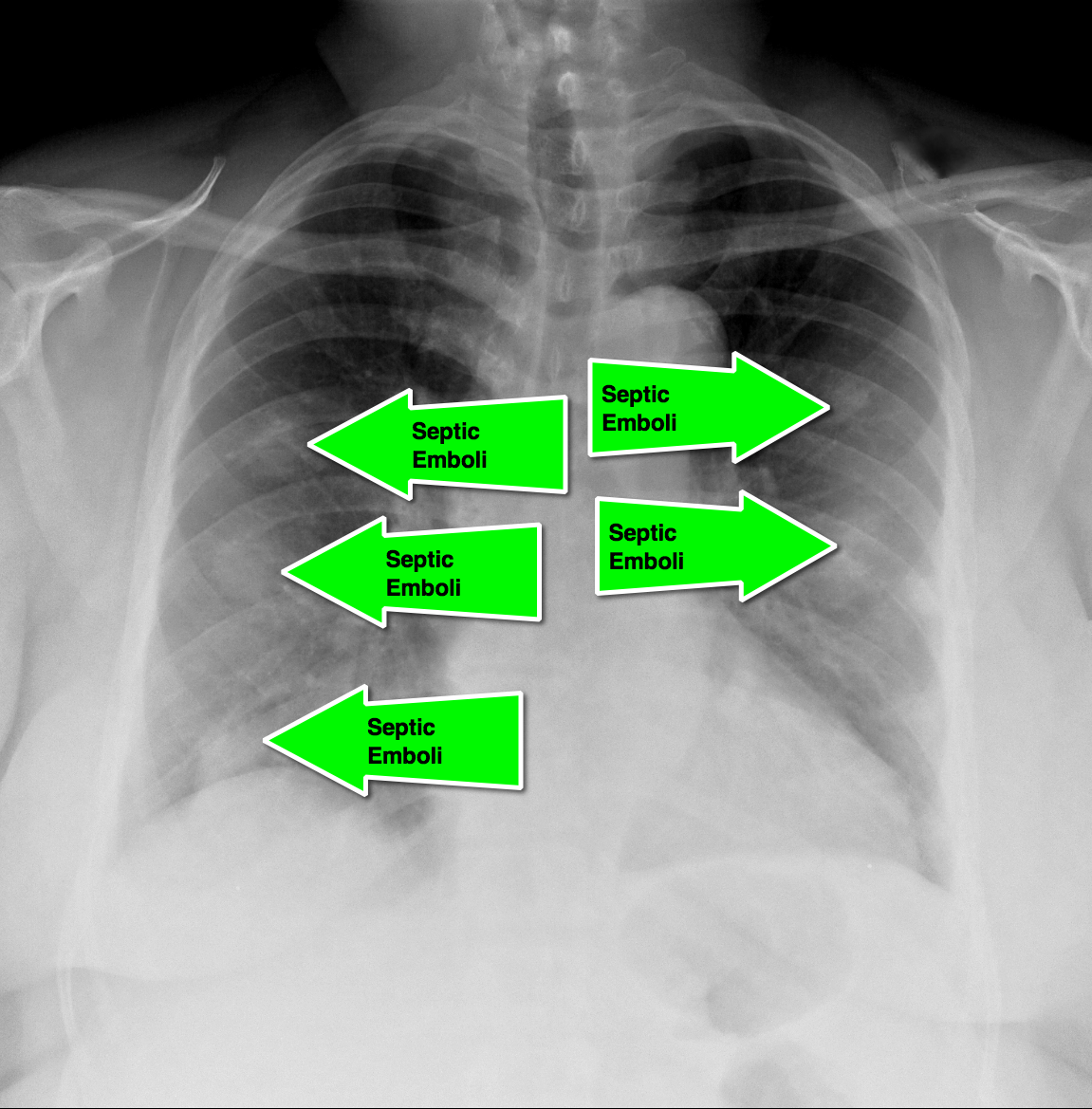
62 year-old male presents with weakness, chills, cough, and malaise. Recently, he had four teeth extracted but felt fine immediately after the extraction. Past medical history includes diabetes and hypertension; CXR is below. What’s the diagnosis?
The HEART Score
Acute coronary syndrome defines a spectrum of diseases (unstable angina, NSTEMI, STEMI), without clear ECG abnormalities the diagnosis and disposition can be challenging
Several scoring systems have attempted to risk stratify patients: TIMI, PURSUIT, and GRACE
The TIMI & PURSUIT scores were designed to identify higher-risk patients and long-term mortality
A pilot/observational study has utilized a novel scoring system to risk stratify low to intermediate risk patients
The HEART (History, ECG, Age, Risk factors and Troponin) score:
This scoring system is limited given the small study size and requires further study/validation, but may be an easy, quick, and reliable predictor of outcome in chest pain patients
Carbon Monoxide Half-Life:
35 year-old carpet-layer presents with swelling of the superior portion of his knee that has progressively gotten worse over one week. He has no fever and has full range of motion (although pain is worse with movement). The knee is not tender to touch and the area is not erythematous or warm. What's the diagnosis?

In a collaborative effort between the Illinois Poison Center and the Illinois Hospital Association, a new study sought to determine a poison center's effect on hospital length of stay (LOS) and hospital charges.
While the methodology was understandably complex, the authors compared ~5,000 toxicology inpatients with poison center assistance to 5,000 toxicology inpatients without poison center assistance.
After adjusting for confounders, the LOS among patients with posion center assistance was 0.58 days shorter compared to that of patients without poison center assistance (CI 95%: -0.66, -0.51, p<0.001). Though hospital charges for poison center-assisted patients in the lower quintiles were significantly higher than patients without poison center-assistance (+$953; p<0.001), they were substantially lower in the most costly quintile of patients (-$4852; p<0.001).
Poison center assistance was associated with lower total charges only among the most expensive to treat. However, this outlier group is very important when discussing medical costs.
1. A comet-tail artifact
2. Arising from the pleural line
3. Well defined
4. Hyperechoic
5. Long (does not fade)
6. Erases A lines
7. Moves with lung sliding
Technique
Hot off the press! Pediatrics March 2014 just published results of a meta-analysis that compared 1 or 2 dose regimens of Dexamethasone versus 5 day course of Prednisone/Prednisolone for management of acute asthma exacerbations in pediatric patients. The results showed that Dexamethasone was as efficacious as the longer course of Prednisone. End points used were return trips to the emergency department and hospital admissions. On further review of the literature, parents tend to prefer the shorter duration of therapy with Dexamethasone. Also, there is less vomiting associated with Dexamethasone. There have been several articles published that show Dexamethasone is more cost-effective than Prednisone. Bottom line: consider giving single dose of Dexamethasone in the ER and then sending patient home with 1 additional dose.
Early diagnosis and surgical consultation for dissection of the ascending aorta can be life saving. Emergency physicians are increasingly using focused cardiac ultrasound to assess chest pain patients in the ED.
The suprasternal notch view (SSNV), may provide additional information in the assessment of thoracic aortic pathology. A recently performed pilot study aimed to determine the accuracy of using the SSNV, in addition to the more traditional parasternal long axis view in assessing aortic dimensions as well as pathology compared to CTA of the chest.
Using a maximal normal thoracic aortic diameter of 40 mm, diagnostic accuracy in detecting dilation of the aorta was 100%. The study showed that the SSNV is feasible and demonstrates high agreement with measurements made on CTA of the chest.
Herpes Gladiatorum in Wrestlers
HSV causes non genital cutaneous infections primarily in wrestlers, commonly called herpes gladiatorum (HG)
Annual incidence in NCAA wrestlers is 20% to 40%
Most common cutaneous infection leading to lost practice time (40.5% of all infections)
Transmission is skin to skin.
Incubation period is 4 to 7 days from exposure. Healing usually occurs within 10 days after the initial lesion (without scaring).
Appearance: Numerous grouped uncomfortable (painful) vesicles/pustules on an erythematous base…evolve into moist ulcerations, followed by crusted plaques. Lesions typically get abraded during competition therefore may have an atypical appearance and may be mistaken for other infections such as staph. Distribution typically more diffuse than typical HSV infections. Occurs on body surfaces areas that typically come into contract with opponents (face, head, neck, ears, upper extremities). Lesion location typically on side of patient’s handedness. Recurrences occur at location of initial outbreak, a useful diagnostic aid.
Perform a thorough examination as ocular involvement was seen in 8% of high school wrestlers in one HG outbreak.
Typical treatment for primary infection is Valacyclovir 1g PO b.i.d. for 7 days. This is best started within 24h of symptom onset.
Aseptic meningitis is meningitis with negative bacterial cultures. Overall, viral infections are the most common etiology, however medications can also cause this illness.
Well known causes of aseptic meningitis include: antimicrobials (particularly sulfamethoxazole/trimethoprim), NSAIDS, antivirals (valacyclovir), and antiepileptics.
Recently an abstract was published that suggests that patients on levetiracetam have a higher risk of developing aseptic meningitis than those on topiramate and gabapentin. Lamotrigine has also been implicated, but appears to have a lower risk than levetiracetam, topiramate and gabapentin.
Recruitment Maneuvers for ARDS
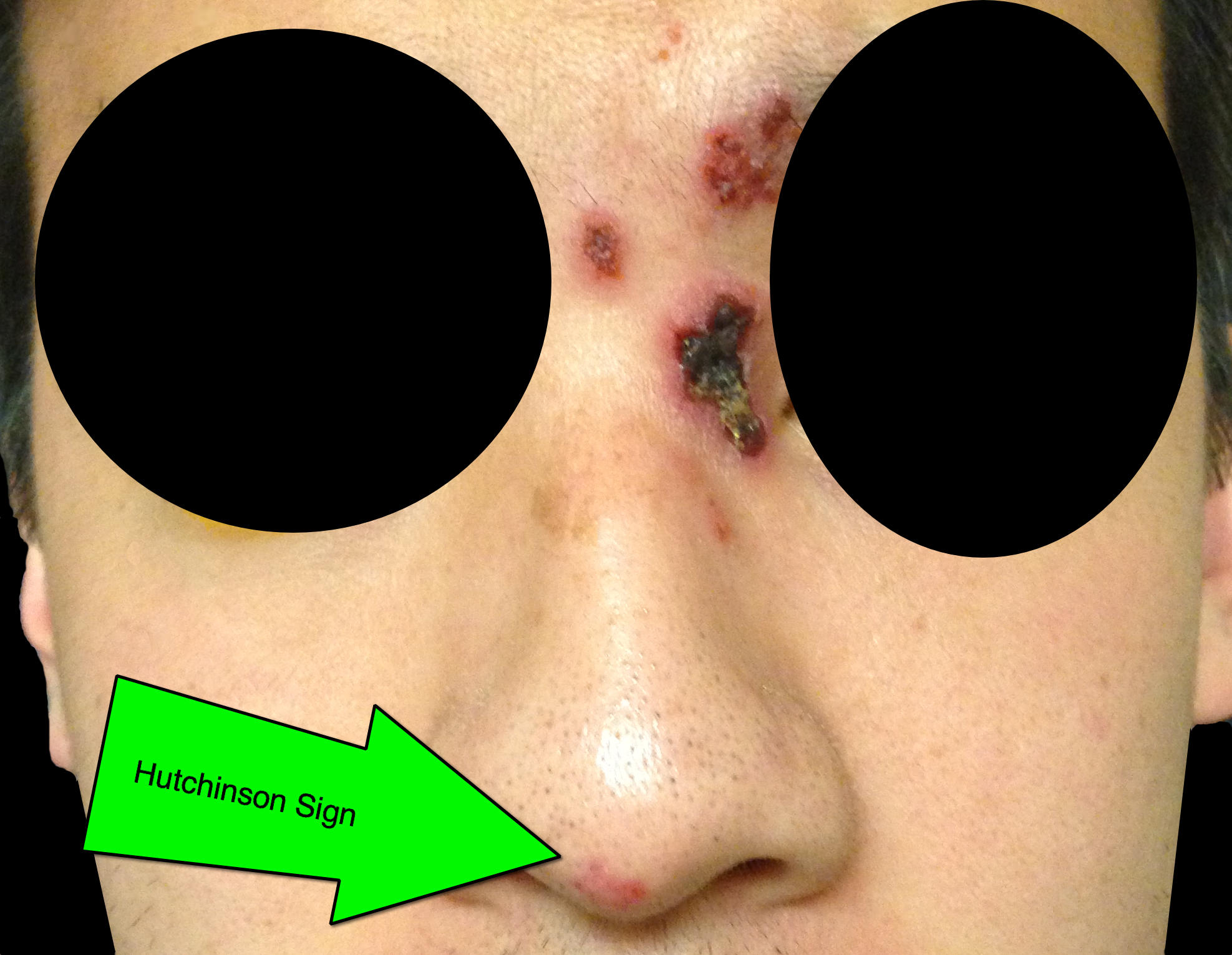
32 year-old male presents with the following. What's the diagnosis?

Pulseless Electrical Activity (PEA)
ACLS algorithm for PEA focuses on memorizing the “ H's & T's" without a systematic approach on how to evaluate & treat the possible etiologies
A modified approach to PEA focuses on “cause-specific” interventions utilizing two simple tools: ECG and Bedside Ultrasound (US)
Simplified PEA Algorithm
♦1st obtain the ECG and assess the QRS-complex length (narrow vs. wide)
♦ A narrow QRS-complex suggests a mechanical problem: RV inflow or outflow obstruction
Utilize bedside US to assess for RV collapsibility vs. dilation
A collapsed RV suggests tamponade, tension PTX or mechanical hyperinflation
A dilated RV suggests PE
The above listed etiologies all have a preserved/hyperdynamic LV Tx begins w/aggressive IVF’s followed by “cause-specific” therapy: pericardiocentesis, needle decompression, forced expiration/vent management, and thrombolysis respectively
♦ A wide QRS-complex suggests a metabolic (hyperK/acidosis/toxins), ischemic, or LV problem
Utilize bedside US to assess for LV hypokinesis/akinesis
For metabolic/toxic etiologies treat w/calcium chloride and sodium bicarbonate +/- vasopressors
For ischemia and LV failure treat w/cardiac cath. vs. thrombolysis +/- vasopressors/inotropes
♦Trauma and several other etiologies of PEA that are seldom forgotten in any critically ill patient (hypothermia, hypoxia, and hypoglycemia) are not included in this algorithm.
Background
The ACLS recommendation for epinephrine dosing in most cardiac arrest cases is 1 mg every 3-5 minutes. This dosing interval is largely based on expert opinion.
Primary Outcome
A new study reviewed 21,000 in-hospital cardiac arrest (IHCA) cases from the Get With the Guidelines-Resuscitation registry. The authors sought to examine the association between epinephrine dosing period and survival to hospital discharge in adults with an IHCA.
Methods
This pattern was consistent for both shockable and non-shockable cardiac arrest rhythms.
Acid and Alkali burns are all known for their caustic cellular injury to local tissue. Acid burns and specifically hydrofluoric acid has systemic toxicity. HF can be lethal even if there is only a 5-10% total body surface area burn. You can find HF in brick cleaner, glass etching and wheel cleaner. They main metabolic derangement is hypocalcemia which can lead to cardiac dysrrhythmias and death.
Treatment has ranged from IV calcium or even intra-arterial calcium in the affected limb to treat the local severe pain associated with an HF burn. Checking a serum calcium to be sure IV calcium replacement is also necessary.
Remember HF -> severe pain, minimal tissue damage, hypocalcemia, hyokalemia, dysrrhythmias
Bottom Line:
University of Maryland Section of Global Emergency Health
Author: Veronica Pei
Intensive BP Control in Spontaneous Intracranial Hemorrhage
Managing the patient with hypertensive emergency in the setting of spontaneous intracerebral hemorrhage (ICH) is often a challenge. Current guidelines from the American Stroke Association are to target an SBP of between 160 - 180 mm Hg with continuous or intermittent IV antihypertensives. Continuous infusions are recommended for patients with an initial SBP > 200 mm Hg.
An emerging concept is that rapid and aggressive BP control (target SBP of 140) may reduce hematoma formation, secondary edema, & improve outcomes.
Recently published, the INTERACT 2 trial (n=2,829) compared intensive BP control (target SBP < 140 within 1 hour) to standard therapy (target SBP < 180) found:
Study flaws: Patients treated with multiple drugs - combinations of urapadil, labetalol, nicardipine, nitrates, hydralazine, and diuretics. Management variability away from protocol seemed high. (Interesting editorial)
A Post-hoc analysis of the INTERACT 2 published just this month suggests that large fluctuations in SBP (>14 mmHg) during the first 24 hours may increase risk of death & major disability at 90 days.
Bottom Line: INTERACT 2 was a large RCT but not a great study (keep on the look out for ATACH II). However, in patients with spontaneous ICH, consider early initiation of an antihypertensive drip (preferably nicardipine) in the ED to reduce blood pressure fluctuations early with a target SBP of 140 mmHg.
Follow me on Twitter: @JohnGreenwoodMD