Current evidence does not support the use of fasciotomy or dermotomy following North American Crotalinae envenomation with elevated intracompartmental pressures. [1]
A new case report of a 17-month old bitten by a copperhead snake reinforces that early and adequate administration of crotaline Fab antivenin is the treatment of choice. [2]
Many experts recommend against measuring compartement pressures altogether; we know it will be elevated.
Background Information:
Infections by Staphylococcus aureus cause significant morbidity and mortality around the world, but up until now no effective vaccines have been developed. Some prior attempts at vaccination actually led to higher mortality in the vaccinated group. However, a group at University of Iowa developed a vaccine targeting S. aureus virulence factors that has shown promise in animal models.
Pertinent Study Design and Conclusions:
Bottom Line:
While not available for human use yet, this is the first promising vaccine against S. aureus infections (including MRSA). Stay tuned…
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Pearls for the Crashing LVAD Patient
37 year-old male presents after sustaining a burn from a pot of boiling water. He states that his skin started to blister a few hours after and it’s quite painful. What type of burn does he likely have?

Head lice infestation is a common problem in the United States with treatment costs estimated at 1 billion dollars and cases affecting millions of children each year. Many of these children present to the ED for care...lucky us! Traditional therapies containing permethrin and pyrethrins are having increased rates of treatment failure likely secondary to increasing resistance and medication noncompliance. The typical first line agents require multiple doses. There are safety concerns regarding therapies that contain malathion and lindane in children. Is there another option? Topical ivermectin 0.5% lotion applied to scalp in a single dose has been shown to be effective and safe for treatment of head lice infestation in children older than 6 months. It was FDA approved at the end of 2012. Considerations include cost. Sklice lotion is expensive!
The NEJM article was considered an "editors pick" by the AAP as one of the best articles of 2012-2013.
Assessment of Intermediate Coronary Lesions
- Coronary angiography alone to assess CAD is fraught with subjectivity
- Fractional flow reserve (FFR) has become the standard to assess/quantify obstructive CAD; it determines the myocardial flow in the presence of stenosis identifying the lesion responsible for ischemia
- FFR assesses focal stenosis, but does not consider diffuse atherosclerotic narrowing or microcirculatory dysfunction as contributors of ischemic heart disease
- An index of microcirculatory resistance (IMR) can be concomitantly measured with FFR during cardiac catheterization to specifically evaluate the microvasculature
- Coronary flow reserve (CFR) was the 1st proposed method for assessment of intermediate coronary lesion, but proved suboptimal because of its variability especially in patients with microvascular dysfunction (diabetes, prior MI, etc.)
- Utilization of FFR, IMR, and CFR together support the existence of differentiated patterns of ischemic heart disease & may help to determine future ischemic events
46 patients treated with high-dose droperidol (10-40 mg) were studied prospectively with continuous holter recording.
What they did
Patients initially received 10 mg droperidol as part of a standardized sedation protocol (for aggression). An additional 10 mg dose was given after 15 min if required and further doses at the clinical toxicologist's discretion.
Continuous 12-lead holter recordings were obtained for 2-24 hours. QTc > 500 msec was defined as abnormal (with heart rate correction - QTcF).
What they found
Only 4 patients had abnormal QT measurements, three given 10 mg and one 20 mg. All 4 had other reasons for QT prolongation. No patient given > 30 mg had a prolonged QT. There were no dysrhythmias.
What it means
There was little evidence supporting droperidol being the cause and QT prolongation was more likely due to pre-existing conditions or other drugs.
Tranexamic acid (TXA) is an antifibrinolytic that prevents clot breakdown by inhibiting plasminogen activation and plasmin activity
The CRASH-2 trial enrolled 20,211 adult trauma patients with significant hemorrhage (SBP <90 or HR 110) or at significant risk of hemorrhage
Patients were randomized to 1 gram TXA over 10 minutes followed by an infusion of 1 gm over 8 hours vs placebo
There was a significant reduction in the relative risk off all cause mortality of 9% (14.5% vs 16%, RR 0.91, CI 0.85-0.97, p = 0.0035)
The patients that benefited most were those most severely injured, and in those treated in less than 3 hours of injury.
Background Information: While the concept of Emergency Medicine is fairly well understood in the United States, it is less clear in countries where the concept is not as well established. This has caused quite a bit of confusion and hindered progress and collaboration.
Pertinent Study Design and Conclusions: In a recent consensus conference held at SAEM several definitions were standardized.
Bottom Line:
It is imperative that the same terminology be used when discussing the delivery of care on a time-sensitive basis.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
VAD thrombosis: A Must Know VAD Complication
The HeartMate left ventricular assist device (LVAD) is one of the most frequently placed LVADs today. Originally, it was thought to have a lower incidence of thrombosis due to its mechanical design. However, a recent multi-center study published in the NEJM reported a dramatic increase in the rate of thrombosis since 2011 in the HeartMate II device. The report found:
An increase in pump thrombosis at 3 months after implantation from 2.2% to 8.4%
The median time from implantation to thrombosis was 18.6 months prior to March 2011, to 2.7 months after.
Pump thrombosis is a major cause of morbidity and mortality (up to almost 50%!!) and is a can't miss diagnosis. It's important to keep thrombosis on the differential for any VAD patient presenting with:
Power spikes or low pump flow alarms on the patient's control box
Pump (VAD) failure
Recurrent/new heart failure
Altered mental status
Hypotension (MAP < 65)
Signs of peripheral emboli (including acute CVA)
Useful lab findings suggestive of thrombosis include:
Evidence of hemolysis
LDH > 1,500 mg/dL or 2.5-3 times the upper limit of normal
Hemoglobinuria
Elevated plasma free hemoglobin
Bottom Line: In the patient with suspected VAD thrombosis, it is important to contact the patient's VAD team immediately (CT surgeon, VAD coordinator/nurse, VAD engineer). Treatment should begin with a continuous infusion of unfractionated heparin, while other treatment options can be discussed with the VAD team.
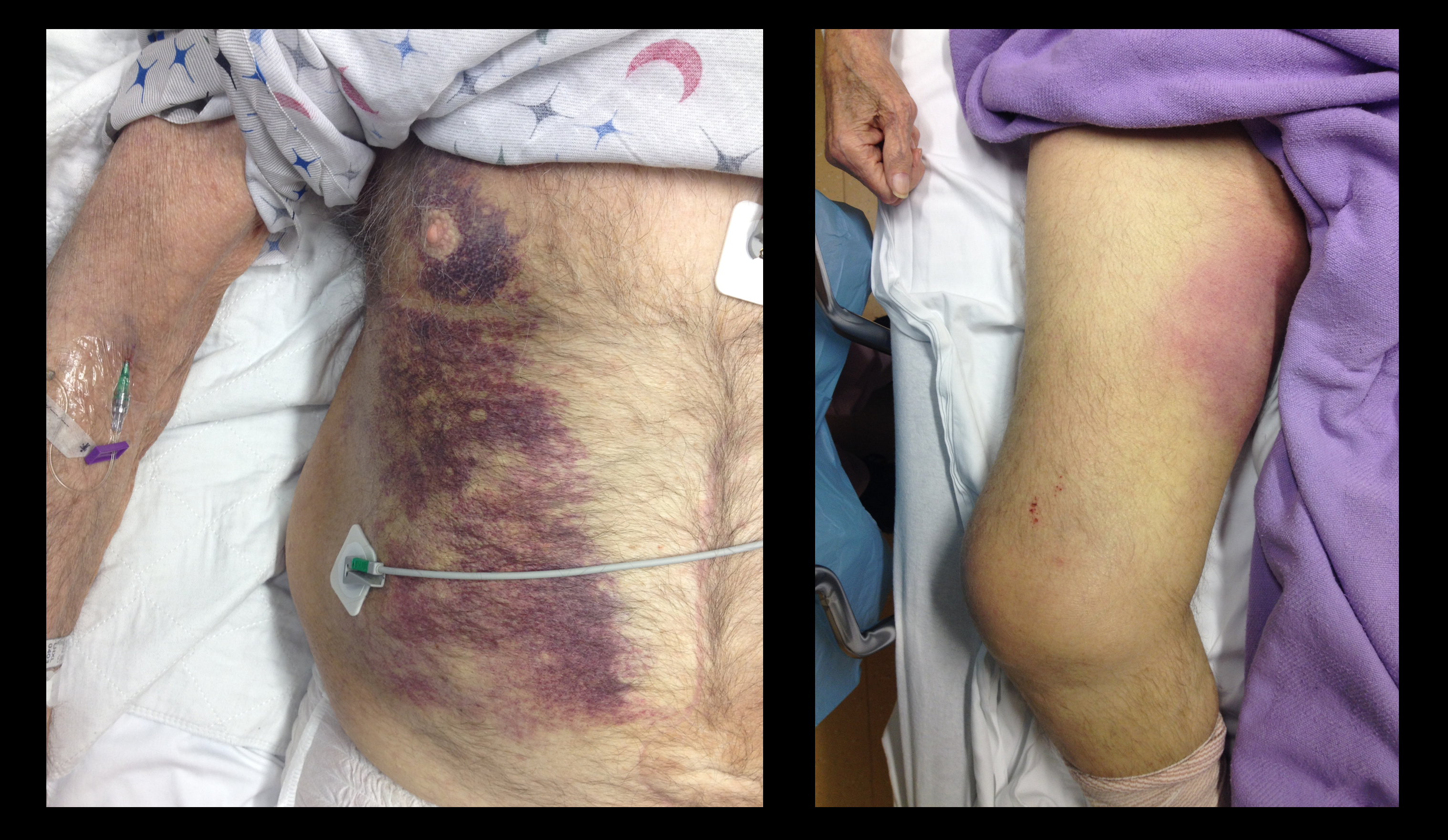
68 year-old male presents with weakness after surgical repair of his abdominal aorta. What’s the diagnosis and name at least one eponym for the signs displayed (there are five total)?
There is debate and confusion regarding where and how to measure ST elevation (STE). Do you measure the STE at the J-point? Or at 40 msec after the J-point? And how much STE is considered significant? The current guidelines have clarified this issue.
- STE should be measured at the J-point.
- STEMI is defined by STE ≥ 1 mm in at least 2 contiguous leads, with the exception of leads V2-V3.
- STEMI is defined by STE ≥ 2 mm in leads V2-V3 in men.
- STEMI is defined by STE ≥ 1.5 mm in leads V2-V3 in women.
For more cardiology pearls from the 2013 literature , check out Amal Mattu's Articles You've Gotta Know!
Want more emergency cardiology pearls? Follow me @alifarzadmd
No single feature of the history of physical examination reliably rules out ostemyelitis
Aids in making the diagnosis include:
An ulcer area larger than 2 cm2 (LR 7.2),
A positive probe to bone test (LR 6.4),
An ESR greater than 70 mm/h (LR 11)
Though an uncommon exposure, it can occur from chronic mercury exposure. One mode of exposure that I have seen is with elemental mercury thermometers that were broken to collect the beads of mercury - for entertainment. This occurred in a child's room and were forgotten. One child presented with personality changes and pink hands and feet. The patient suffered from severe mercury poisoning and acrodynia due to prolonged exposure to the mercury vapor.
Acrodynia or Pink Disease includes:
Irritability, shyness, photophobia, pink discoloration of the hands and feet and polyneuritis.
Case Presentation:
A 10 year old boy presents with a dog bite sustained 3 days ago, during a family trip to India. He has no prior history of vaccination and, at the time, he was taken to a local clinic where the wound was irrigated and he received a rabies vaccine.
Clinical Question:
Now that his has come to your ED 3 days later, is there anything further to be done?
Answer:
This patient should also receive rabies immunoglobulin (RIG) and complete his post-exposure prophylaxis. Post-exposure prophylaxis is a combination of rabies vaccine and rabies immunoglobulin (RIG).
RIG:
Vaccine:
Bottom Line:
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg
The morbidity and mortality from pseudomonas aeruginosa infections is high and empiric double-antibiotic coverage (DAC) is sometimes given; quality evidence for this practice is lacking.
Although there is little supporting data, the following reasons have been given for DAC:
The potential harm of antibiotic overuse cannot be ignored, however, and include adverse reaction, microbial resistance, risk of super-infection with other organisms (e.g., Clostridium difficile), and cost.
There may be a signal in the literature demonstrating a survival benefit when using DAC for patients with shock, hospital-associated pneumonia, or neutropenia. The IDSA guidelines, however, do not support DAC for neutropenia alone; only with neutropenia plus pneumonia or gram-negative bacteremia.
Bottom line: Little data supports the routine use of DAC in presumed pseudomonal infection. It may be considered in patients with shock, hospital-associated pneumonia, or neutropenia (+/- pneumonia), but consult your hospital’s antibiogram or ID consultant for local practices.
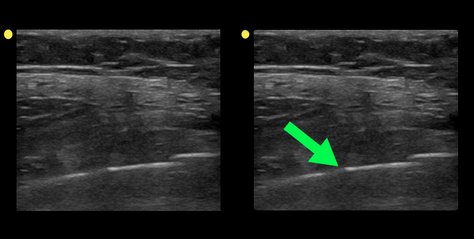
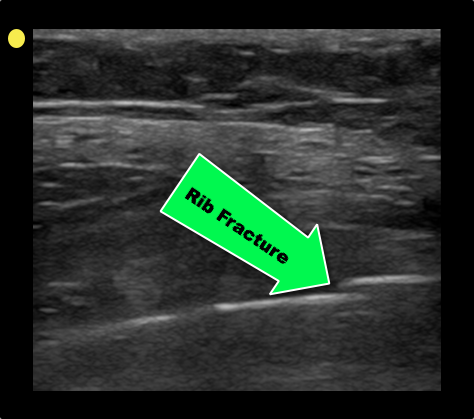
Patient with a history of osteogenesis imperfecta presents with right lateral chest pain following a sneeze. The ultrasound of his chest is shown (hint: arrow points to a rib). What's the diagnosis?